I’m continuing my deep dives into the genetic pathways to get actionable insights as the previous ones have been incredible precise and useful. This time I’m looking at the mitochondria related genetic pathways.
Here is the general description of the pathways and their variants. I will put the finding about my own genome below it as an example of what useful and actionable insights you can get.
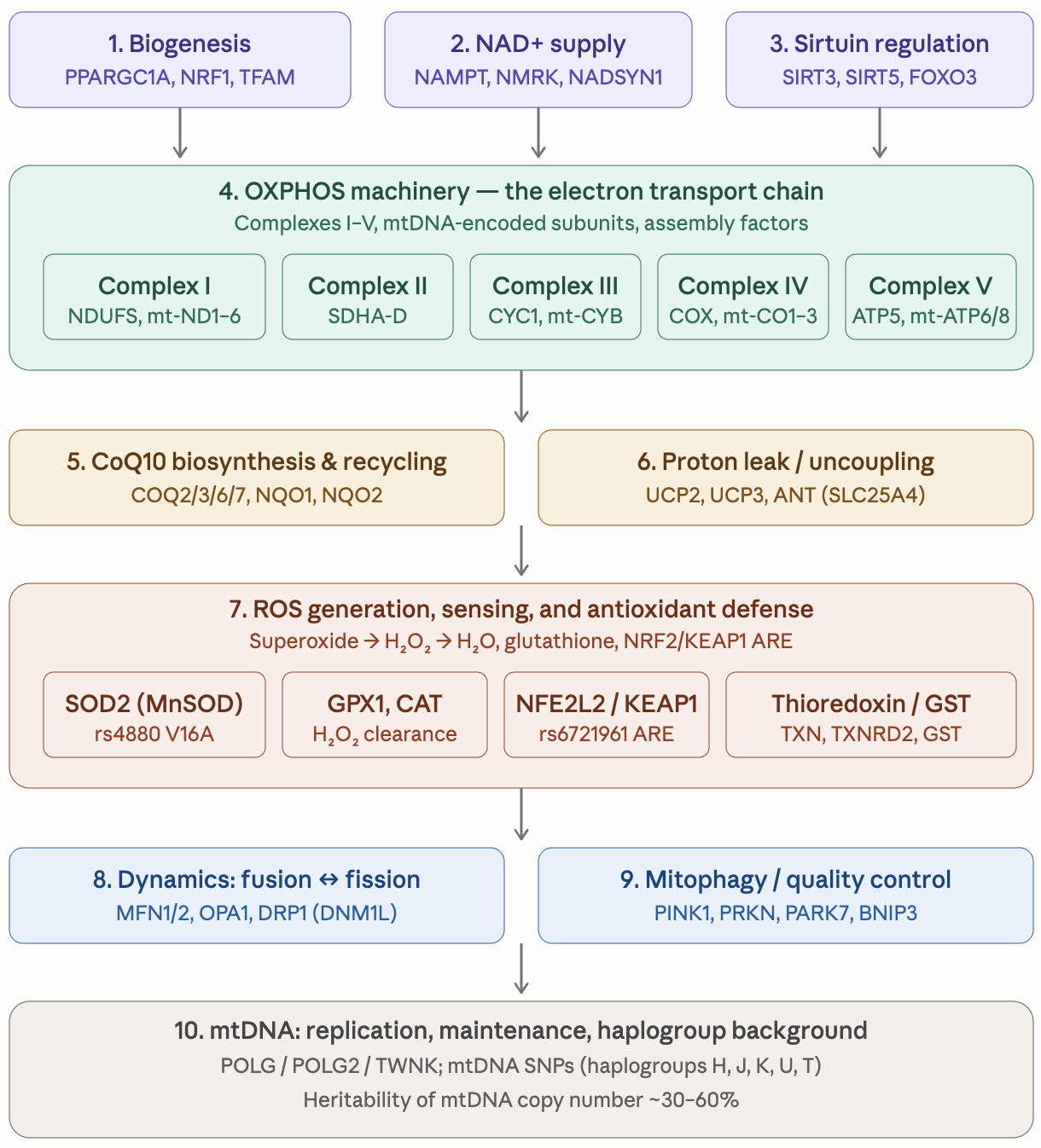
Mitochondrial_Genetic_Pathway_Reference.pdf (670.2 KB)
The pdf report above is valid for everybody but here is the summary of the findings I get when I apply it to my own genome.
Mitochondrial Pathway — Top 10 Findings
1. PPARGC1A rs8192678 G/G (Gly482/Gly482) — HOM-REF, highly favorable
Full-activity PGC-1α genotype. Substrate for inducible mitochondrial biogenesis maximally responsive to aerobic exercise, cold exposure, fasting, ketogenic state, and PGC-1α-targeted supplements. Reinforces favorable Endurance-report findings; supports the empagliflozin/imeglimin/tirzepatide/telmisartan stack which converges on AMPK→PGC-1α.
2. NQO1 rs1800566 P187S het (G/A) — pharmacogenomic flag, regimen-aligned
~50% NQO1 enzyme activity. Reinforces ubiquinol-form CoQ10 over ubiquinone-form (current Ubiquinol 100 mg q.o.d. is genotype-aligned). Communicate to oncology if anthracycline/mitomycin/platinum chemotherapy ever indicated (PharmGKB Level 2B/3). Modest NRF2 protein-stability impact partially compensated by sulforaphane (Avmacol).
3. FOXO3 longevity haplotype, 1-copy carrier (rs2802292 G/T HET; 5 LD-block SNPs HET concordantly) — favorable
Donlon 2018 dominant model: ~13–18% reduction in all-cause mortality, slower telomere attrition, ~1.9× odds of reaching 95+ years, replicated across 11+ populations. Benefit is NAD⁺-substrate-dependent through the SIRT1/FOXO3 axis.
4. SOD2 rs4880 V16A het (Val/Ala) — intermediate matrix MnSOD activity
~15–20% reduced matrix MnSOD vs Ala/Ala. OSA-severity association noted in Sleep report (Khani 2025). Compensatory levers in current regimen: Avmacol (NRF2→SOD1, GCLC/GCLM), NACET (GSH substrate), Mn 1 mg multivitamin. Direction managed; no specific change indicated.
5. POLG no pathogenic variants detected — valproate hepatotoxicity contraindication does NOT apply
Targeted check of W748S, A467T, Y955C all HOM-REF; whole-region scan returned no obvious additional pathogenic missense. Removes the PharmGKB Level 1A POLG-valproate restriction. Useful negative finding for any future neurology/psychiatry context.
6. NFE2L2/NRF2 promoter rs6721961 — homozygous protective allele (gene-strand C/C)
Strand-orientation note: VCF shows REF=T ALT=G GT=1/1 at chr2:177,265,309. GRCh38 reference at this position carries the MINOR allele; ALT=G on forward = C on gene strand = the major/protective allele. Homozygous for the protective allele — Marzec 2007 ARE-binding deficit ABSENT. NRF2 transcriptional capacity preserved.
7. GSTP1 rs1695 Ile105Val HOM-ALT (Val/Val) — reduced phase-II detoxification activity
Reduced GSTP1 enzymatic activity for electrophile/xenobiotic conjugation. Increases dependency on GSH substrate supply. Current NACET + glycine + sulforaphane stack provides genotype-aligned compensation.
8. NADSYN1 rs12785878 HOM-ALT — vitamin D level locus
Per-allele 25-OH-D-lowering effect (Wang 2010 Lancet). Currently takes vitamin D3 5000 IU q.o.d.; HOM-ALT genotype suggests measure 25-OH-D and titrate to 50–80 ng/mL — current dose may yield sub-target trough.
9. PINK1 / PRKN / PARK7 / MFN2 / OPA1 / DNM1L — no germline pathogenic variants
Mitophagy axis (PINK1–Parkin–DJ-1) genetically intact; CMT2A-class MFN2, dominant optic atrophy OPA1, DRP1 dominant-negative all absent. Caveat: PRKN exon-deletion CNVs are not detectable by standard SNV pipelines — MLPA targeted test if clinical indication ever arises.
10. CoQ10-pathway cumulative HOM-ALT/HET signals (NQO2 HOM-ALT, COQ3 HOM-ALT, COQ6 HOM-ALT, COQ7 HOM-ALT, NQO1 het, COQ2 het) — supports daily ubiquinol + plasma CoQ10 verification
Each individual signal is small; cumulative direction supports increasing Ubiquinol from 100 mg q.o.d. to 100–200 mg daily, especially given concomitant pitavastatin (HMG-CoA reductase inhibition upstream of CoQ10 biosynthesis). Plasma CoQ10 measurement (target 1.0–1.5 µg/mL) provides empirical titration anchor.