How do you like them apples?
Paper reference: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2846712
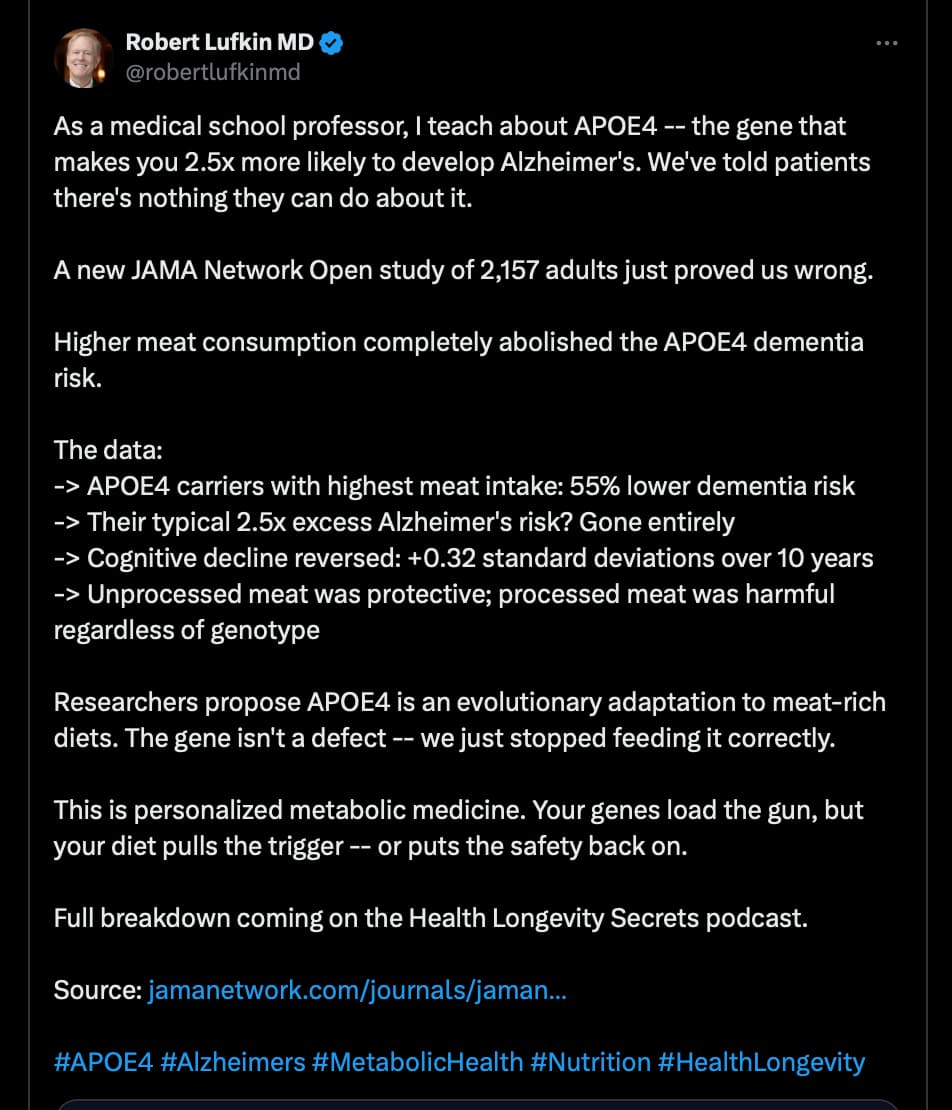
https://x.com/robertlufkinmd/status/2036399359495930268?s=46&t=4EadOlXmhNuHXx8rV1pc9g
I glanced at the paper. @DrFraser ?
How do you like them apples?
Paper reference: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2846712
https://x.com/robertlufkinmd/status/2036399359495930268?s=46&t=4EadOlXmhNuHXx8rV1pc9g
I glanced at the paper. @DrFraser ?
Interesting paper … but having a Mediterranean diet has more robust and varied sources supporting it, and consumption of meat results in multiple other bad health outcomes. I think the PRO-21 diet from Dr. Mischley is probably not only valid for PD but also AD … and read meat is among many items that results in faster neurodegeneration (others are really interesting like canned fruit, frozen vegetables).
I would be much more interested if this paper also controlled for methylmalonic acid and omega 3 index. I suspect those confounders would explain away the benefit. Those are items I monitor and optimize in my patients. These 2 factors likely explain excess late neurodegeneration in vegans.
I’ll go with Vera Health’s review of this topic.
But quite importantly as I remind my ApoE4 patients, the incredible focus on ApoE4 and neurodegeneraton only matters if you live long enough to get dementia. So doing things that increase heart disease and cancer risk and not optimizing all those things and unifocal view of just your ApoE4 is a bad strategy.
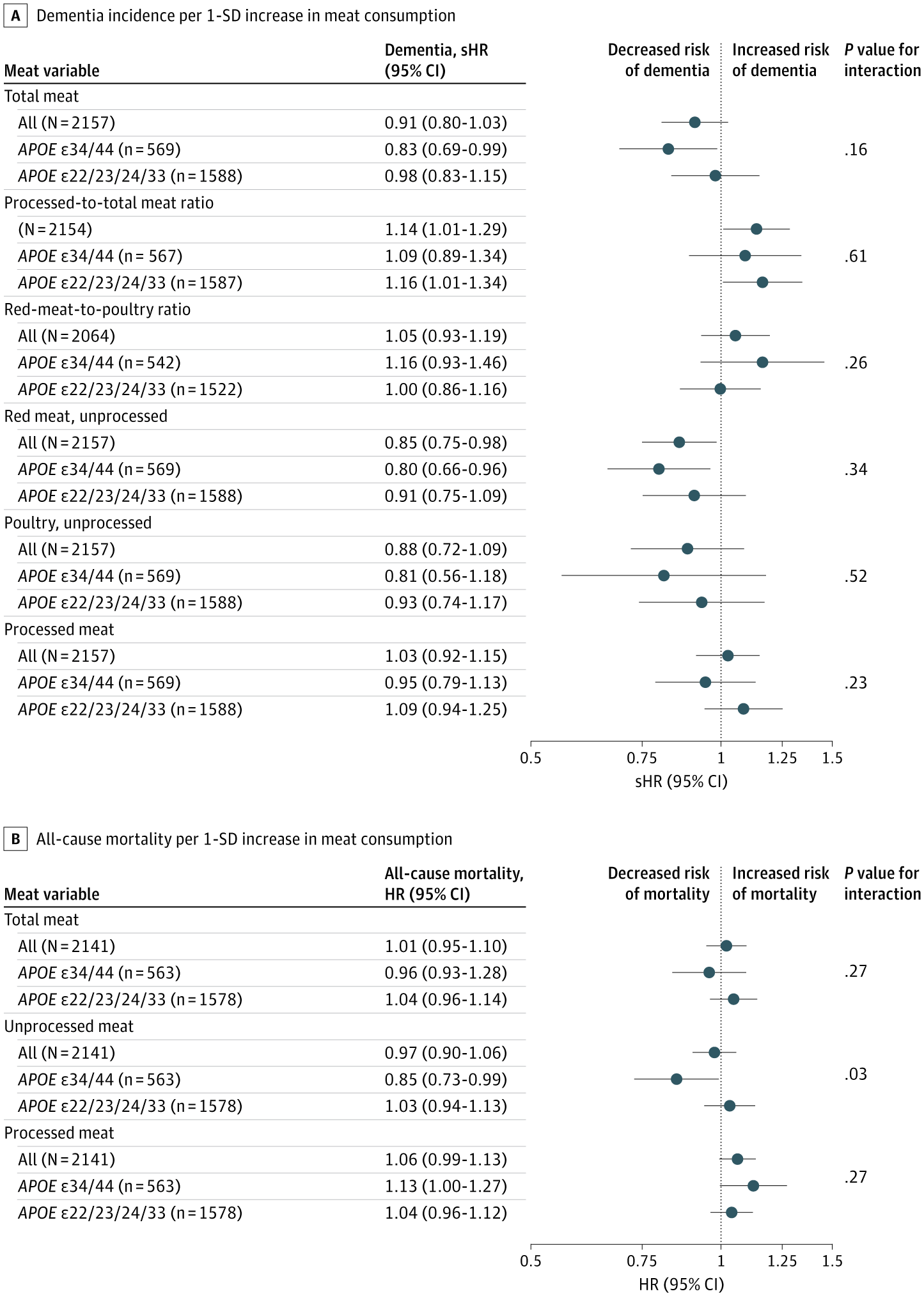
Higher meat consumption does not consistently decrease Alzheimer’s disease or dementia incidence; the most reproducible signal across large cohorts is higher risk with processed meat, while unprocessed red meat shows mixed (sometimes inverse) associations, and any apparent benefit may be genotype- and meat-type–specific rather than a general protective effect.
Clinical interpretation: if counseling on dementia prevention from this evidence base, prioritize limiting processed meat rather than increasing overall meat intake; any “protective” association for higher meat intake appears non-generalizable and may depend on meat processing and possibly APOE genotype rather than meat quantity per se.
I agree for the reasons you list also also the design that produced the headline findings. This study is definitely interesting but a very long way from determinative. In contrast, the sheer volume and degree of consensus on Mediterranean style eating is determinative.
As the title suggests, the findings are for a specific cohort, not the general population.
Study Population
The Swedish National Study on Aging and Care–Kungsholmen (SNAC-K) is an ongoing, longitudinal, population-based study targeting individuals aged 60 years or older in an urban area of Stockholm.22 In the first wave (2001-2004), 3363 of 5111 randomly selected individuals were enrolled; 2157 participants met the inclusion criteria for this analysis: baseline data on diet, cognition, and APOE status and no dementia at baseline.
Nordic, 60+, urban area dwellers.
Conclusions
In this cohort study, we found that the APOE34/44 group exhibited the anticipated excess risk of cognitive decline and dementia progression compared with participants with other genotypes when consuming meat at levels consistent with current dietary guideline targets. However, this disadvantageous association was absent at higher consumption levels, equivalent to more than twice the target.33 Viewed alongside reinterpreted evidence from NHS37 and UK Biobank21 focusing on unprocessed meat, these findings point to a consistent gene-diet interaction, with important implications for public health. Results reinforce the urgency of investing in precision nutrition research with a focus on APOE, which could ultimately inform future policy development.
However, our findings align with underappreciated patterns in 2 large cohorts. In the UK Biobank (493 888 participants), unprocessed red meat was inversely associated with dementia (P = .01), driven by APOE4 carriers (HR, 0.64 per 50-g/d increase; P < .001), with no associations in noncarriers (HR, 0.93; P = .59).21 In the Nurses’ Health Study (NHS) and Health Professionals Follow-up Study (133 771 participants), supplementary analyses revealed an APOE4 interaction (P < .001) for unprocessed red meat, showing favorable trends among carriers and adverse trends among noncarriers.
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2846712
I kinda fit that cohort-ish. ![]()
Midwest dinner, beef meat, tators and whole milk. Maybe some ![]() corn or lettuce.
corn or lettuce.
One supporting perspective is the lower prevalence of APOE4 , suggesting adverse selection, in agricultural regions.15 In Europe, APOE4 allele frequency decreases gradually from up to 27% in the north to as low as 4% in the south.
I find the Pro 21 diet to be very interesting. Folks on this who score well have seen little if any progression of their PD.
I don’t have data to support, but as much as the pathology is somewhat different between PD and AD, I suspect that this data is to at least some extent applicable to AD.
Now in regard to B12 measured by MMA and Omega 3 optimization, in vegans leading to late neurodegenerative disease and excess hemorrhagic stroke, the data supporting this is yet to be published from the AHS.
Manage these things and the risk is likely mitigated.
I worry about those who rely on the LPC omegas, particularly if homozygous E4. It’s not at all convincing that these get into the brain. This the advice is having a few serves of fish that are small and wild caught, which is problematic for vegans.
We are doing this now and have given up this component of being WFPB, but for cause. Sorry to all the fish.
I like them apples. This is the natural diet of man as far as I am concerned.
While my diet is not strictly carnivore or keto, I eat red meat 2 or 3 times a week.
My diet leans toward low-carb, not because I necessarily think it is the best diet. It is the diet I have evolved to eat. In other words, I eat what I want, and that results in my particular low-carb diet.
@desertshores But I’m apoe3/4 and apparently I am not evolved enough to rely on plant based diets and should thrive on meat. I’ve got no diet dogmas but don’t seem to love the taste of it. Shouldn’t I naturally prefer it more? You’ve mentioned elsewhere that you don’t have an apoE4 allele so you’re more evolved than me, and supposedly would do better with less meat and more plants, according to that study. Yet you prefer the opposite.
Maybe it’s not true that our natural tastes and proclivities lean towards what’s phenotypically best for us. Maybe they’re established differently or more by nurture than nature.
At any rate, Dr. Fraser makes interesting points. However I don’t think they account for the cognitive decline of apoe 2-3 carriers being associated with more fresh meat intake, because if said intake is indeed just a messy proxy for omega3 index, the same association (more meat —> more omega 3s —> better dementia protection) should hold for all genotypes. The fact that the relationship is switched suggests to me that the authors might be right about their hypothesis. But I have to read it more carefully.
Yes I noted those nuggets too and found them very persuasive.
Also… I’m from the Mediterranean and was reared on the diet. There’s plenty plenty of unprocessed meat in it. People in North America seem to think it’s all olive oil doused salads. My husband and I are both apoe3/4. He eats a ton of steak because he loves it. I eat very little meat as I don’t seem to enjoy it. Aside from that my diet is much healthier than his but I have to note he functions better now than I do, mentally. He didn’t when we first met 20 years ago.
Can you please comment more on this. I started taking LPC because you recommended them as a form to get into the brain. Are you saying you no longer believe this to be true, or are you just saying you eat fish as insurance but still believe in taking LPC if you have a copy of apoe4?
But are you apoE4? THAT is the cohort.
It also exasperates me to see apoE4 functional differences from the other genotypes presented as modifications — “apoE4 changes how XYZ gets done, introduces defective handling of ABC,” etc. You’d never know from the way it’s presented that apoE4 is the ancestral genotype and the others are the innovations, therefore the modifications. Obviously they’ve evolved due to selective pressures. One obvious one would be the grandmother / grandfather hypothesis, the evolutionary advantage to someone surviving well into old age, past child rearing years, to be helpful 2-3 generations down the road, and you can’t be helpful if you’re demented by then. So that is one simple hypothesis that can account for the development of the other genotypes, simply as a vehicle to stave off dementia until much later, practically until after something else kills you first.
But I don’t see why such a pressure wouldn’t have existed millions of years earlier, at least hundreds of thousands of years earlier, before Homo sapiens split from the common ancestral stock. Also apoE4 women are more prone to dementia yet it’s the grandmothers way more than the grandfathers who did any grandchild rearing traditionally. AND there’s the fact that Alzheimer’s is virtually unknown in primitive societies so how could such pressure have even played out?
It seems very plausible that these genotypes evolved under the selective pressure of different dietary sources and patterns INSTEAD, since apoe is involved in a lot—from lipids to metabolism. And then the geographic distribution of its prevalence overlapped with agricultural prevalence becomes very interesting indeed.
Ahhh… no I meant older, strong North European roots. No alzheimer’s in my paternal or maternal descendants.
And my mind very sharp, thanks to rapamycin.
“We could perform gut microbiota analysis on patients or conduct fecal metabolite analysis,” explained Nishiwaki.
“Using these findings, we could identify individuals with specific deficiencies and administer oral riboflavin and biotin supplements to those with decreased levels, potentially creating an effective treatment.”
Full study below.
https://www.nature.com/articles/s41531-024-00724-z
Taxonomic analysis showed that species Akkermansia muciniphila was increased in PD, while species Roseburia intestinalis and Faecalibacterium prausnitzii were decreased in PD.
I too added fish to my decade plus of WFPB diet. I have Hashimoto’s hypothyroid, as well as a slew of other autoimmune diseases, including osteoporosis, rheumatoid arthritis, Sjogren’s syndrome, lupus, and celiac disease. I have read that soy products I contraindicated with Hashimoto’s, which have been my main source of protein and calcium for a long time. So about a month ago, I added wild caught sardines, with bones and skin, 1 can twice weekly to increase my protein intake, as well as calcium and zinc. Sardines are low on the chain so less mercury and other toxins. Sardines also provide some vitamin B12.
FWIW: ChatGPT-5
"Findings like this in microbiome studies of Parkinson’s disease almost always have multiple potential confounding factors. The observation that Akkermansia muciniphila is increased while Faecalibacterium prausnitzii and Roseburia intestinalis are decreased is reported in several PD microbiome studies, but it does not necessarily mean Akkermansia contributes to the disease. Here are the main confounders researchers worry about.
So the microbiome pattern may simply reflect slow intestinal transit, not the disease itself.
Both depend heavily on fermentable fibers for growth.
Effects reported in studies include:
So the microbiome differences may reflect treatment rather than disease.
This could partially explain the pattern observed.
Less activity (common in PD) is associated with:
Athletes, in contrast, often show higher levels of Faecalibacterium.
6. Gut inflammation
Parkinson’s patients often show intestinal inflammation and barrier dysfunction.
In that environment:
butyrate producers decline
mucin-degrading species like Akkermansia may expand
So the shift may reflect a damaged gut ecosystem, not the cause of the damage.
How researchers interpret the pattern now
The most common interpretation today is:
↓ Faecalibacterium and Roseburia → reduced butyrate production
↑ Akkermansia → response to mucus barrier stress
This suggests a dysbiotic gut environment, but the direction of causality is unclear.
Why this matters for supplementation
This finding is one reason some microbiome researchers caution against assuming more Akkermansia is always beneficial. Its role may depend heavily on the surrounding ecosystem.
In contrast, bacteria like Faecalibacterium prausnitzii and Roseburia intestinalis are generally considered protective because they produce butyrate, which supports:
![]() Bottom line:
Bottom line:
Yes—there are several strong confounding factors (constipation, diet, medications, age, inflammation). The microbiome pattern seen in Parkinson’s patients may reflect secondary changes from the disease and lifestyle factors, rather than Akkermansia being harmful or causative.
The study only observed that akkermansia is elevated in PD. It did not conclude that it is causative.
I only highlighted it, because if I had a relative with PD (like one participant here), I would recommend not supplementing with akkermansia. I would recommend the riboflavin and biotin. At worst, they would have no effect and would only produce expensive urine. . But they are harmless, and could benefit the PD afflicted.
Back to the study about risk reduction for APOE4 carriers by meat consumption.
Looking at the confidence intervals crossing (or touching) 1.0 in relative risk / hazard ratio.
Interestingly, red meat to poultry ratio is a total mess
.
The data shows more or less statistical non-significance.
How can the authors conclude then a 55% risk reduction for APOE 4 carriers?
I may be overlooking something, but I find it surprising that such a strong claim was drawn from these data and allowed to be published.
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2846712