Interesting MS findings… Thank you for sharing ![]()
Are there trials ongoing to delete CCR5 via CRISPR? Seems like by doing so, they could address memory loss and HIV.
Have also requested quote from my (thankfully non-judgmental) Indian suppliers ![]()
1 Like
Very interesting discussion, and new information to me.
Among the steps I go through in recommending interventions to patients is a Risks, Benefits, and Alternatives approach.
The human brain has failed to do the same thing that the mouse brain does (in regard to neurodegeneration or neuroregeneration) on most substances tested.
I suspect the muscle effects and senescent cell effects would however be similar.
We ultimately need a trial on this specific question - or even looking at patients with HIV on this drug vs. those on alternative drugs and tracking of cognition, muscle strength, measures of senescent cell burden.
There are potential significant side effects with this medication - not too common … but I’d not be mixing it with other agents, so one would have to consider the loss of potential benefit of some other agents I might prefer to be taking … such as sirolimus.
Need more human data that looks at the questions that are being asked. I think the data might be out there, and just not utilized for this specific reason. If anyone finds research on these questions in humans, please get those to me.
4 Likes
Yes, if we were mice, things would look better when it comes to life extension and brain health.
Talking about mice’s neurons I read this recently.
1 Like
See the links posted by @RapAdmin, especially the Alzheimer’s Drug Discovery Foundation, for data signals in humans (admittedly not very strong signaling, but not noise either). It all points in the same general direction. Still might not be worth the risks, or it might be worth considering as a periodic pulsed treatment as opposed to ongoing. Or might be worth considering for intranasal delivery only, like the rifampicin protocol (for nearly identical reasons — by the way, how is THAT going for you or any patients of yours who have taken the plunge, if you don’t mind my asking?).
If I were a baller and didn’t care for my own life in the process of finding ways to extend life in general, I’d pair me Maraviroc with mild intermittent hypoxia conditioning to see what happens.
1 Like
It seems in 98%+ that the side effects are pretty benign. Are you really dissuaded by this side effect profile? If a person is a healthy 50 or 60 year old with no pre-existing conditions, perhaps pausing rapamycin during a maraviroc trial, would you view the risks differently? I dove into greater depth with ChatGPT 5.0 on the risks, see below:
Here’s a concise, evidence-based safety profile for maraviroc (SELZENTRY® / CELSENTRI®), covering what tends to happen, how often, how severe, and whether effects can last.
The “big” risks to have on your radar
- Hepatotoxicity (with allergic features): Boxed warning. Can present with rash, fever, eosinophilia, ↑IgE and liver injury; reported cases often appeared ~1 month after starting. Get baseline LFTs and recheck if any symptoms; stop immediately if hepatitis or severe hypersensitivity is suspected. Severe liver failure is rare but can be life-threatening and may leave lasting damage.
- Severe skin/hypersensitivity reactions (e.g., SJS/TEN): Post-marketing reports exist; discontinue at once if severe rash/systemic symptoms occur. Potential for long-term sequelae (scarring, ocular issues).
- Cardiovascular events (ischemia/MI): In treatment-experienced trials, 11/ ~609 patient-years (≈1.3%) on maraviroc vs 0 on placebo; absolute rates were low, but use caution in those with cardiac comorbidity or on BP-lowering drugs. Long-term follow-up also found low MI rates (~1.1 per 100 patient-years). (PMC)
- Postural hypotension/syncope: Risk rises with severe renal impairment and concomitant potent CYP3A inhibitors/inducers (contraindicated in such combinations). Dose reduction may be needed if symptoms occur. Usually reversible but increases fall risk.
How often do adverse effects happen?
Regulatory data give two complementary views: exact event lists by percent in FDA tables and frequency bands(common/uncommon/rare) in the EMA SmPC.
Common, usually mild–moderate (often ≥5–10%)
- Upper respiratory infections, cough, pyrexia, dizziness, rash (more frequent than placebo in treatment-experienced trials).
- GI symptoms (nausea/diarrhea/abdominal pain/constipation); in one pediatric cohort: vomiting 12%, abdominal pain 4%, diarrhea 4%, nausea 4%, dizziness 3%. Typically self-limited.
- Lab shifts: Grade ≥3 AST >5× ULN ~4.8%, ALT >5× ULN ~2.6%, bilirubin >2.5× ULN ~5.5% (similar to placebo overall). Usually resolve with continued therapy or discontinuation.
- Other “common” per SmPC: anemia, anorexia, depression, insomnia, rash, asthenia; ALT/AST increases. Generally reversible. (European Medicines Agency (EMA))
Uncommon (≥0.1% to <1%) / notable
- Postural hypotension; seizures; hyperbilirubinemia/GGT↑; renal events (proteinuria/renal failure)—mostly reversible; evaluate for confounders and DDIs. (European Medicines Agency (EMA))
Rare / very rare / post-marketing
- Toxic hepatitis, hepatic failure/cirrhosis (rare); hepatic failure with allergic features (very rare). Potential for permanent injury. (European Medicines Agency (EMA))
- Severe cutaneous reactions (SJS/TEN)—frequency not precisely known; stop immediately; risk of long-term sequelae.
- Neoplasms: Early theoretical concern because CCR5 modulates immune surveillance, but no increased malignancy rates observed versus comparators in trials (exposure-adjusted malignancies per 100 pt-years: 4.6 MVC vs 9.3 placebo in experienced; 1.0 MVC vs 2.4 efavirenz in naïve).
Permanence / long-term impact
- Most common AEs (URI symptoms, GI upset, dizziness, mild rash, lab bumps) are transient and fully reversiblewith symptomatic care or dose/therapy changes. Discontinuation rates due to AEs were ~5% and similar to placebo at 48 weeks.
- Hepatotoxicity with hypersensitivity can be severe; early recognition and drug cessation are key. Some cases can progress to lasting liver impairment or failure.
- SJS/TEN can leave permanent cutaneous/ocular sequelae.
- Cardiovascular events (rare) may have permanent consequences; overall long-term rates were low in extended follow-up. (PMC)
- Infections/malignancy (theoretical CCR5 concerns): Large trials show no increase vs controls; long-term observational data (>5 years) report low rates and no new safety signals. (PMC)
Who is at higher risk?
- Severe renal impairment (CrCl <30 mL/min) plus potent CYP3A inhibitors/inducers → contraindicated(exposure spikes; hypotension risk).
- Pre-existing liver disease / HBV or HCV coinfection → monitor more closely; lower threshold to stop if LFTs rise with rash/systemic symptoms.
- Concomitant BP-lowering agents / cardiovascular comorbidity → greater susceptibility to hypotension-triggered events.
- Formulation note (EU/UK): tablets contain soya lecithin; contraindicated in peanut/soya allergy (excipient). (European Medicines Agency (EMA))
Practical monitoring & mitigation (brief)
- Before start: Confirm CCR5-tropic HIV (when used on-label), baseline LFTs, renal function; review CYP3Adrug interactions.
- Early on (first 2–8 weeks): Watch for rash, fever, malaise, jaundice, RUQ pain; check LFTs if symptomatic. Most hypersensitivity/hepatitis cases cluster here.
- BP / falls: Ask about dizziness/syncope; if severe renal impairment without DDI, dose reduction from 300→150 mg BID is advised if hypotension occurs. Avoid DDI-contraindicated regimens.
- Infections/malignancy: Routine vigilance, but no special screening beyond standard HIV care is recommended based on current data.
Bottom line
Maraviroc’s typical side effects are mild–moderate and reversible (URI symptoms, GI upset, dizziness, mild rash). Serious risks—idiosyncratic hepatotoxicity with allergic features, severe skin reactions, postural hypotension (esp. with renal impairment + DDIs), and rare CV events—are uncommon to rare, but warrant front-loaded monitoring and strict DDI management. Long-term datasets (≥5 years) show low rates of hepatic failure, MI, and malignancy, with no new safety signals emerging over time. (PMC)
If you’d like, I can turn this into a one-page monitoring checklist (baseline labs, week-by-week watch-outs, and DDI flags) tailored to on-label or off-label use.
======================
when you say that Maraviroc’s risk of oxic hepatitis, hepatic failure/cirrhosis; hepatic failure with allergic features, are rare or very rare, what exactly does this mean in terms of risk? Is this 1 out of 1,000 or closer to 1 out 100,00 patients frequency?
Great question — the regulatory terms “rare” and “very rare” have standardized frequency bands in drug safety language:
- Common: ≥1/100 to <1/10
- Uncommon: ≥1/1,000 to <1/100
- Rare: ≥1/10,000 to <1/1,000
- Very rare: <1/10,000
- Not known: cannot be estimated from available data
For maraviroc specifically (per EMA SmPC and FDA labeling):
- Hepatic failure, toxic hepatitis, cirrhosis → classified as rare (≈1 in 1,000–10,000 patients).
- Hepatic failure with allergic features (the boxed warning scenario) → classified as very rare (<1 in 10,000 patients).
- The “not known” category is sometimes used post-marketing if there aren’t enough cases to calculate a frequency.
So in practical terms:
- Routine mild ALT/AST elevations are relatively common (a few percent).
- Clinically significant hepatotoxicity is very uncommon — closer to 1 per several thousand to tens of thousands treated patients.
- Fulminant hepatic failure is extremely rare — closer to 1 per ≥10,000, though precise rates are hard to pin down because they’re based on spontaneous case reports rather than prospective trial counts.
![]() Put another way: the vast majority of patients never experience severe liver injury on maraviroc, but the risk is taken seriously because the outcome (if it occurs and is missed) can be life-threatening or permanent. That’s why regulators mandate baseline and symptom-triggered monitoring rather than routine frequent labs in all patients.
Put another way: the vast majority of patients never experience severe liver injury on maraviroc, but the risk is taken seriously because the outcome (if it occurs and is missed) can be life-threatening or permanent. That’s why regulators mandate baseline and symptom-triggered monitoring rather than routine frequent labs in all patients.
====================
Are certain types of patients with certain health profiles, ages or disease processes more likely to experience Hepatic failure than others?
Yes — the risk of clinically significant hepatic failure with maraviroc isn’t evenly distributed. The regulatory guidance and post-marketing experience highlight several patient profiles where the risk is higher:
1. Patients with Pre-Existing Liver Disease
-
Chronic viral hepatitis (HBV or HCV coinfection):
In HIV populations, coinfection is common, and these patients already have a higher baseline risk of hepatotoxicity. Maraviroc’s labeling specifically notes more frequent transaminase elevations in this group. -
Alcoholic liver disease, cirrhosis, NAFLD/NASH:
Any condition with compromised hepatic reserve means that even modest injury can tip the patient toward failure.
2. Patients with Hypersensitivity/Allergic Predisposition
- The boxed warning highlights hepatitis with systemic allergic features (rash, eosinophilia, fever, ↑IgE).
- Individuals with a history of severe drug hypersensitivity or autoimmune-like reactions may be at higher risk, though precise rates aren’t quantified.
3. Older Age & Polypharmacy
-
Ageing liver: Older patients may have reduced hepatic reserve, slower regeneration, and more comorbidities (diabetes, metabolic syndrome).
-
Polypharmacy and CYP3A4 inhibitors/inducers:
Maraviroc is metabolized via CYP3A4; interacting drugs (e.g., certain antifungals, macrolides, rifampin, anticonvulsants, antiretrovirals like ritonavir) can raise or lower levels significantly.- ↑ Exposure → higher risk of toxicity.
- ↓ Exposure → loss of efficacy, viral breakthrough.
4. Renal Impairment (Indirect Risk)
- Severe renal impairment plus potent CYP3A inhibitors raises maraviroc plasma levels several-fold, increasing the chance of systemic adverse events (including hypotension and possibly hepatotoxicity).
- This combination is contraindicated, but sometimes arises in complex HIV patients.
5. High Baseline Inflammatory/Immune Activation
- Because some hepatotoxic cases were tied to immune-allergic phenomena, patients with active immune dysregulation (autoimmune disease, eosinophilia, atopy) may be more susceptible.
6. Advanced HIV Disease
- Patients with very low CD4 counts or long treatment history may have more comorbid viral hepatitis, polypharmacy, and fragile physiology, compounding risk.
Who tends to tolerate maraviroc best?
- Younger patients without HBV/HCV coinfection,
- No prior severe hypersensitivity history,
- Normal baseline LFTs,
- No severe renal impairment or major CYP3A interactions.
![]() Key clinical practice point:
Key clinical practice point:
Hepatic failure from maraviroc is rare (<1 in 10,000), but most cases cluster in those with pre-existing liver disease or hypersensitivity features. That’s why the label stresses baseline LFTs, vigilance in the first 4–8 weeks, and rapid discontinuation if systemic hypersensitivity signs appear.
Here’s a structured risk stratification table for hepatic failure on maraviroc — combining regulatory labeling, trial data, and post-marketing insights:
 Maraviroc Hepatic Failure Risk Stratification
Maraviroc Hepatic Failure Risk Stratification
| Risk Level | Patient Profile | Key Risk Drivers | Clinical Implications |
|---|---|---|---|
| Low Risk | - Age <60, normal baseline LFTs - No HBV/HCV coinfection - No history of severe drug allergies - Normal renal function - Limited or no CYP3A interacting drugs |
- Healthy liver reserve - Low background hepatotoxic risk - Predictable maraviroc pharmacokinetics |
- Routine baseline LFTs - Symptom-triggered monitoring |
| Moderate Risk | - Age >60 - Mild chronic liver disease (e.g., NAFLD, mild fibrosis) - Stable HBV or HCV with normal LFTs - Polypharmacy with potential CYP3A4 modulators (careful dose adjustment possible) - Moderate alcohol use |
- Reduced hepatic reserve - Higher susceptibility to drug-induced injury - Possible drug interactions raising maraviroc exposure |
- Baseline & periodic LFTs (e.g., every 1–3 months) - Educate patient about early hypersensitivity/hepatic symptoms |
| High Risk | - Active HBV or HCV with elevated transaminases - Cirrhosis, prior hepatic failure, or autoimmune hepatitis - Severe renal impairment + potent CYP3A inhibitors (contraindicated if both present) - History of severe drug hypersensitivity (e.g., DRESS, SJS/TEN) - High alcohol intake, metabolic syndrome with advanced liver disease |
- Strong baseline vulnerability to hepatic injury - Risk of immune-mediated hepatotoxicity - Increased likelihood of severe or irreversible liver failure |
- Avoid maraviroc if alternatives available - If used: baseline LFTs, monitor closely in first 4–8 weeks - Discontinue promptly if systemic allergic/hepatic signs emerge |
 Key Takeaways
Key Takeaways
-
Most patients fall in the Low → Moderate risk range.
-
High-risk groups are where true hepatic failure cases cluster in post-marketing reports.
-
Monitoring intensity should scale with risk:
- Low risk: baseline labs, then symptom-driven.
- Moderate risk: baseline + routine periodic labs.
- High risk: avoid or monitor very intensively if no alternatives.
5 Likes
I agree with you that most are minor and self limited with removal of the drug. I’m pretty cautious, especially with drugs that I’m not already highly familiar with. Many that I use have potential significant side effects, but I’m familiar with those, know how to guard against them and manage them.
The other issue is polypharmacy as I’m already utilizing other drugs to work on accomplishing the same thing (at least the goal end point) albeit through other mechanisms. What is the marginal benefit/risk of adding more.
I’m not saying this might not be a better choice, I’d like to see other physicians have a go at it for a while and see what happens, or see additional data.
If I had a patient get a significant hypersensitivity reaction … and I’m prescribing it for this indication, I’m not sure the medical board would be kind to my license. Doesn’t mean that groups of biohackers won’t have a go at it - and the comfort level will get greater.
5 Likes
It makes perfect sense from a prescribing physician’s point of view. Any update on intranasal rifampicin?
1 Like
With regard to safety and tolerability of this drug, it seems like 300mg/day is well tolerated in this study of using it for post-stroke depression: ( admittedly a small sample size).
Methods
We conducted a 10-week clinical trial in which ten patients with subcortical and cortical stroke, suffering from PSD. were administered a daily oral dose of 300 mg Maraviroc. Participants were then monitored for an additional eight weeks. The primary outcome measure was serious treatment-emergent adverse events (TEAEs) and TEAEs leading to discontinuation. The secondary outcome measure was a change in the Montgomery-Asberg Depression Rating Scale (MADRS).
Results
Maraviroc was well tolerated, with no reports of serious adverse events or discontinuations due to intolerance. The MADRS scores substantially reduced from baseline to week 10 (mean change: -16.4 ± 9.3; p < 0.001). By the conclusion of the treatment phase, a favorable response was observed in five patients, with four achieving remission. The time to response was relatively short, approximately three weeks. After the cessation of treatment, MADRS scores increased at week 18 by 6.1 ± 9.6 points (p = 0.014).
Conclusions
Our proof-of-concept study suggests that a daily dosage of 300 mg of Maraviroc may represent a well-tolerated and potentially effective pharmacological approach to treating PSD. Further comprehensive placebo-controlled studies are needed to assess the impact of Maraviroc augmentation on PSD.
Key Findings
- Safety: Maraviroc was well tolerated. No serious adverse events or discontinuations were reported. Minor side effects (e.g., dry mouth, insomnia, dizziness) were mild, resolved during treatment, and deemed unlikely to be drug-related BioMed CentralPubMed.
- Efficacy:
- MADRS scores dropped significantly by a mean of −16.4 ± 9.3 points by Week 10 (p < 0.001).
- Response: 5 patients responded, with 4 achieving remission.
- Time to response: ~3 weeks.
- Post-treatment effect: MADRS scores rose by 6.1 ± 9.6 points by Week 18 (p = 0.014), suggesting partial relapse after stopping treatment PubMedBioMed Central.
Full paper (open access) here:
3 Likes
This study demonstrated some significant neuro-cognitive benefits of Maraviroc in humans (albeit in an HIV-infected population):
Background & Rationale
- HIV-associated neurocognitive disorders (HAND): Despite effective combined antiretroviral therapy (cART), 20–50% of HIV patients continue to show cognitive impairment, especially in psychomotor speed, working memory, learning, and executive function.
- Challenges: HAND persists due to chronic inflammation, low-level CNS viral replication, and variable CNS penetration of drugs.
- CCR5 role: HIV replication in the brain heavily depends on CCR5. The CCR5 antagonist maraviroc (already approved for HIV treatment) has:
- Good CNS penetration.
- Anti-inflammatory effects.
- Shown neuroprotective potential in animal and early human studies.
- Objective: Test whether maraviroc-intensified cART improves neurocognition in virally suppressed HAND patients
Results
- Participants:
- 17 randomized (9 maraviroc, 8 control).
- 14 completed study (9 maraviroc, 5 control).
- Mostly middle-aged White males (~55 years), moderate education, long-term HIV with stable suppression.
- Primary Outcome (Neurocognition):
- Improvement in maraviroc arm:
- 6 months: large effect size (d = 0.77).
- 12 months: moderate effect size (d = 0.55).
- No baseline differences between groups.
- Suggests sustained cognitive benefit from maraviroc intensification.
- Secondary Outcomes:
- MRS brain metabolites: No significant treatment-related changes.
- CSF biomarkers: No treatment-related changes in neopterin or β2-microglobulin.
- Indicates clinical improvement occurred without measurable biomarker/metabolite changes
Abstract:
Full paper on Sci-hub
3 Likes
Is anyone trying / using this?
I would try it, if I could get the medications. Given that India and most other countries shipping medications are shut down right now, its very difficult I think.
3 Likes
"C-C chemokine receptor type 5, also known as CCR5 or CD195, is a protein on the surface of white blood cells that is involved in the immune system as it acts as a receptor for chemokines.[5] " (CCR5 - Wikipedia)
“In addition to playing a major role in the activation of host immune responses, chemokines are important for biological processes, including morphogenesis and wound healing, as well as in the pathogenesis of diseases like cancers.[1][3]” (Chemokine - Wikipedia)
Seems like its main systemic functions point to the same direction as growth (aka displacement) signals. So, blocking another one abnormal growth signal reverses some aging and senescence outcomes.
But rapamycin also does the similar thing (blocks abnormal growth signal).
Are rapamycin effects on cognitive function less effective?
1 Like
One of the primary regulators of CCL5 expression is TLR4 signaling (e.g by bacterial LPS), which can induce >800-fold expression in macrophages. This regulation is quite stringent compared to other TLR4-induced genes (requiring both NF-κB and IRF3 for promoter remodeling), which suggests that CCR5 (and/or other activities of CCL5) signaling must be precisely regulated.
There’s also evidence that TLR4 variants govern longevity, although of course this doesn’t prove a CCL5-dependent mechanism.
The role of lipopolysaccaride receptor TLR4 is paradigmatic. It initiates the innate immune response against gram-negative bacteria; and TLR4 polymorphisms, as ASP299GLY, suggested to attenuate receptor signaling, have been described. We demonstrated that TLR4 ASP299GLY polymorphism shows a significantly lower frequency in patients affected by myocardial infarction compared to controls, whereas centenarians show a higher frequency.
Interesting to see this self-report on Maraviroc helping in CFS below. Note that it seems that Maravoc was one of the best treatments…
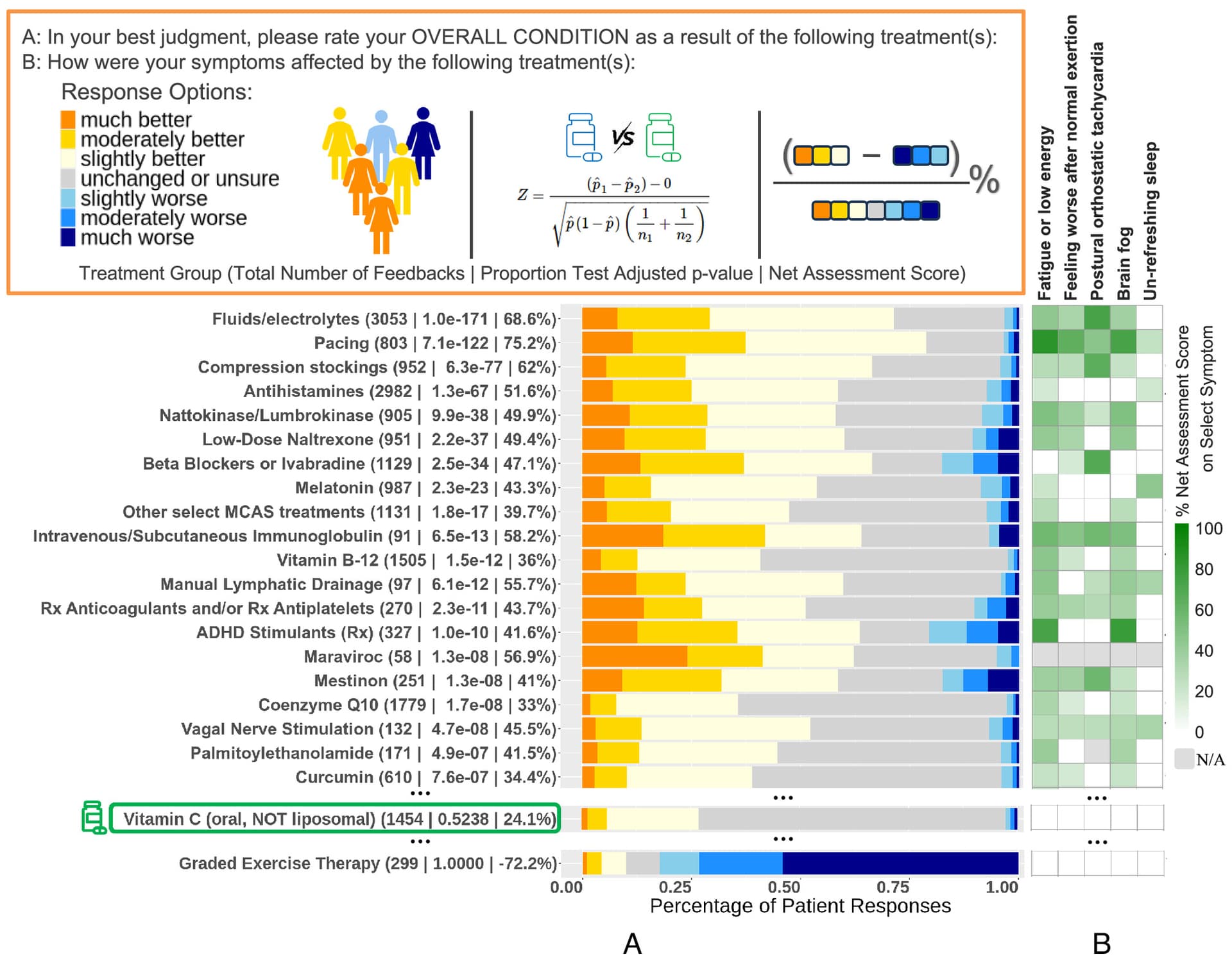
Source:
Patient-reported treatment outcomes in ME/CFS and long COVID
https://www.pnas.org/doi/10.1073/pnas.2426874122
Related:
3 Likes
This is looking like a “No Brainer”.
And at a reasonable{in my view] cost at Walgreens with the discount code below, a prescription is required
U.S. Prescription Discount Coupon _ PharmacyChecker.com.pdf (282.8 KB)
1 Like
The challenge would be to get a prescription… perhaps via Push? Or if you have a very open minded doctor.
1 Like
Hire a physician that work for You, not the other way.
This is not that difficult to locate{a physician]
As it appears this is going to be the Maravircoc Thread…
Review
My view…
Cost{out of pocket in the US]is less the $10.00 per day.
This is not unreasonable to try for several months.
Review the following ;
“Potential application of maraviroc in the therapy of neuropathic pain”.
Sojka P 1, Właszczuk A 1, Olakowska E 1
Author information
Polski Merkuriusz Lekarski : Organ Polskiego Towarzystwa Lekarskiego, 01 Oct 2021, 49(293):379-381Language:pol
PMID: 34800029
Abstract
According to International Association for the Study of Pain (IASP) neuropathic pain is defined as a pain caused by a lesion or disease of the somatosensory nervous system. In general population 7-8% adults suffer from chronic pain with neuropathic characteristic. The most common causes include: lumbar radiculopathy, postherpetic neuropathy, HIV infection, autoimmune diseases (multiple sclerosis), metabolic diseases (diabetic neuropathy), stroke or spinal cord injury. Current pharmacotherapy of neuropathic pain has insufficient effectiveness, so comprehension of neuropathic pain mechanism is necessary for research of new therapeutic methods. In the study we verify the analgesic effect of maraviroc (antagonist of the chemokine receptor - CCR5) and its potential role in the treatment of neuropathic pain. In the study we focused on dependency between opioid and chemokine receptors, because of similar structure between this receptors occurs cross-desensitization phenomenon. Chemokine antagonist maraviroc belongs to a group of entry inhibitors, antiretroviral drug. It enhances analgesic properties of opioids by inhibition of crossdesensitization of opioid’s receptor. Application of maraviroc with morphine can reduce effective dosage of morphine 2,3 fold. Moreover, research show that prophylactic administration of maraviroc without opioid analgesics suppresses development of neuropathic pain symptoms. It has influence on glial phenotype, decreases secretion of proinflammatory cytokines and increases anti-inflammatory cytokine secretion. Furthermore it decreases expression of chemikine receptor mRNA and chemikine ligand’s secreted by microglia and astrocytes as a result of nerve injury. We conclude that maraviroc has immunomodulatory properties, potentiates opioid analgesics effect, and can be used in neuropathic pain therapy as a potential co-analgesic.
Citations & impact
Impact metrics
1
Citation
Jump to Citations
Alternative metrics

Altmetric
Discover the attention surrounding your research
Article citations
Li SL, Li J, Xu HC, Liu YC, Yang TT, Yuan H
Ibrain, 8(1):23-36, 02 Mar 2022
Cited by: 8 articles | PMID: 37786421 | PMCID: PMC10529196
Review![]() Free full text in Europe PMC
Free full text in Europe PMC
Similar Articles
To arrive at the top five similar articles we use a word-weighted algorithm to compare words from the Title and Abstract of each citation.
-
Beneficial properties of maraviroc on neuropathic pain development and opioid effectiveness in rats.
Kwiatkowski K, Piotrowska A, Rojewska E, Makuch W, Jurga A, Slusarczyk J, Trojan E, Basta-Kaim A, Mika J
Prog Neuropsychopharmacol Biol Psychiatry, 64:68-78, 16 Jul 2015
Cited by: 49 articles | PMID: 26190414
-
Comparison of the beneficial effects of RS504393, maraviroc and cenicriviroc on neuropathic pain-related symptoms in rodents: behavioral and biochemical analyses.
Kwiatkowski K, Ciapała K, Rojewska E, Makuch W, Mika J
Int Immunopharmacol, 84:106540, 11 May 2020
Cited by: 21 articles | PMID: 32402949
-
Bidirectional Action of Cenicriviroc, a CCR2/CCR5 Antagonist, Results in Alleviation of Pain-Related Behaviors and Potentiation of Opioid Analgesia in Rats With Peripheral Neuropathy.
Kwiatkowski K, Pawlik K, Ciapała K, Piotrowska A, Makuch W, Mika J
Front Immunol, 11:615327, 21 Dec 2020
Cited by: 22 articles | PMID: 33408720 | PMCID: PMC7779470
Molecules, 28(15):5766, 30 Jul 2023
Cited by: 16 articles | PMID: 37570736 | PMCID: PMC10421203
Review![]() Free full text in Europe PMC
Free full text in Europe PMC
–
Above from:
2 Likes