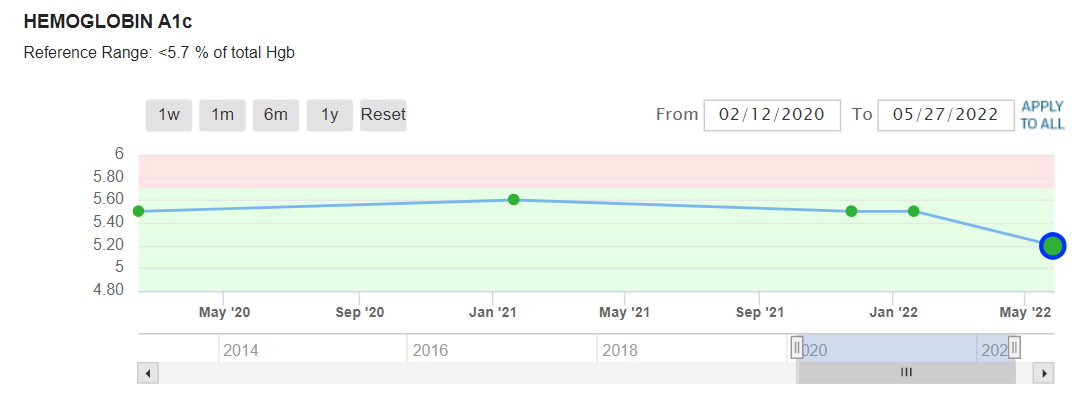
I take metformin and I have been taking high pulse dosing rapamycin. (Currently on a wash-out period) As I am 81 yrs old and my age group is more prone to hyperglycemia. It appears, n=1, that the combo of rapamycin and metformin actually lowers A1c.
Maybe I am an outlier, but I have not experienced an excessive rise in lipids even after high bi-weekly dosing with rapamycin. Some disparage taking metformin, but as I have posted before it has more benefits than just keeping blood sugar in bounds.
The last point on this chart was taken approx 7+ months of taking rapamycin and while I was at my highest dose levels, 20 mg with grapefruit juice and olive oil.
3 Likes
The debate about dosing has me in a quandary about what my dosing regimen should be when I start again in a few weeks.
First, let’s dispense with weekly and bi-weekly dosing. My understanding is that you want to wait for five half-lives before starting your next dose if you are using the pulse dose regimen.
The main side effect of overdosing from taking 20mg rapamycin with grapefruit juice was mild diarrhea for 2-4 days.
When I start again I may try taking 10 mg rapamycin with grapefruit juice and EVOO on two consecutive days and then waiting for 15 days, ~ 5 half-lives, before the next dose.
Because I didn’t start taking rapamycin until I was 80+ years old, I feel I have to take the maxim doses possible without severe side effects.
4 Likes
It is rare, but note we are shooting blind on how much the therapeutical dose is while minimizing side effects while shooting blind on BBB pharmacokinetics. We know continuous dosing is more likely to have side effects without getting to a high Cmax.
The side effects for single high dose one-time in transplant patients originally seemed to have no issues in the short term.
We also have a few informal “case reports” with ultra high dosing (ie 60 mg) if you consider “grey literature”.
And we have enough informal “open label” with Dr. Green that side effects are probably low. At least it seems he hasn’t gotten bad press from any severe side effects with over >1000 patients on 6-8 mg per week.
We are also shooting blind with Prozac in terms of MoA, albeit dosing is not too difficult nor is BBB pharmacokinetics, since it definitely goes past BBB at the levels used. If anything - there is enough evidence for intermittent high dose psilocybin such that the FDA gave it a breakthrough therapy designation. The NNT for GAD for example is 2, much better than Prozac…so far. And I can tell you from my own use intermittent high dose (same as clinical trials, but spread out further at the 2 month mark) works for me and my SO for GAD.
On the other hand, “micro-dosing” or “low dose” every day has only case reports without much formal testing and I do not see much evidence beyond anecdotes - if anything, I would worry about theoretical continuous 5HT2B stimulation severe side effects if done long enough based on frequent MDMA use case reports of valvular disease if someone did that with increasing doses, because there is tolerance.
I’m not measuring rapamycin tissue levels. Just some way to figure out mTORC1 and mTORC2 inhibition levels in one organ crudely with minimal invasiveness (well I don’t consider this one invasive in my circumstance) , but as mentioned only under consideration. Wonder if you can cite the studies you’re referring to showing poor correlation for rapamycin dose vs biopsy mTORC1/2i.
Plus, I have a few normal looking small mole areas that I would be removing anyway for punch biopsy sites. I have enough moles which puts me at elevated risk of skin cancer even though none of them appear melanoma-like from annual full body skin exam so far. I have all the tools and local anesthesia to perform multiple instead of $250 each (basically $1000+/hr if I do it myself) at the derm office out of pocket. ![]()
I’m not waiting on a cancer diagnosis with metastasis before taking higher amounts but if it is localized it could slow a local tumor down on top of a different cocktail I have thought of that might reduce the risk of metastasis enough to get a diagnosis and treatment “early”. I have enough data from WGS to look out for the deadly ones and stratify risk based on the incidence stats (ie age). Not doing this anytime soon though.
1 Like
Rapamycin Pharmacokinetic and Pharmacodynamic Relationships in Osteosarcoma: A Comparative Oncology Study in Dogs
“Results of this study demonstrate that rapamycin can be administered to dogs at pharmacokinetic exposures that are safe and translationally relevant (i.e. achievable in human cancer). These exposures modulate the proximate targets of the mTOR pathway in canine tumors and PBMC without inducing AKT phosphorylation. Inhibition of S6RP phosphorylation was a highly sensitive marker of exposure to rapamycin, even in the lowest dose cohorts, such that its pharmacodynamic modulation was not dose dependent. The biological behavior and histological features of canine and human osteosarcoma are indistinguishable. Many questions remain regarding the optimal use of mTOR inhibitors in cancer and in pediatric osteosarcoma in particular. Responses in clinical trials using mTOR inhibitors have been sporadic and not necessarily predicted by cancer histology. Furthermore modulation of traditional PD biomarkers such as phospho-S6RP, as found in this study, is unlikely to define clinically relevant exposures of rapamycin or rapalogs. This finding was supported by recent PK-PD evaluations(1) in human
patients with solid tumors that found phosphorylation of S6RP in skin surrogates did not correlate with rapamycin dose or response”
"The pharmacodynamic end point was skin phospho-P70 change after 28 days. Pharmacodynamic effect was defined as at least 80% inhibition from baseline. Pharmacodynamic effect occurred across dose levels, and toxicity boundaries ultimately drove dose selection. No objective responses occurred, but five previously progressing patients received at least 12 cycles. However, the selected pharmacodynamic end point did not correlate with dose. Toxicity ultimately drove dose selection
A pharmacodynamic study of rapamycin in men with intermediate to high risk localized prostate cancer:
Results—Thirty-two subjects were accrued, 20 at 3 mg, 2 at 6 mg, 10 controls. No dose-limiting
toxicities (DLTs) were observed at 3 mg; however, 2/2 men enrolled at 6 mg experienced DLTs
including thrombocytopenia and fever with grade 3 stomatitis. Adverse events observed at 3 mg
included stomatitis, rash, ileus, and neutropenia. PD studies demonstrated tumor S6
phosphorylation inhibition in 50% of 10 evaluable rapamycin treated men with sufficient paired tissue (median 58% decline, p=0.049 vs. 2% decline in controls, p=0.75) with no significant effect on AKT activity. There was no change in Ki-67 or caspase-3 cleavage but we noted a reduction in cytoplasmic p27 staining with increased nuclear localization with rapamycin. Prostate tissue rapamycin concentrations were 3–4 fold higher than blood. We found that rapamycin inhibited the activity of a downstream target of TORC1, S6 kinase, in over half of evaluable patients without dose limiting toxicity, thus demonstrating the intended target inhibition and meeting our primary endpoint. However, we found no physiologically relevant effects of rapamycin on tumor cellular proliferation, post-treatment tumor grade or stage, PSA, or apoptosis over a 2 week exposure period. We did not find a correlation between PTEN expression in biopsy and RP specimens, despite using a validated PTEN assay with genetic controls, indicating that different heterogeneous tumors were sampled and analyzed before and after rapamycin, that PTEN expression may have been altered by rapamycin, or a limited power to detect these changes. We additionally found that many of the PD biomarkers such as Akt, p27, caspase-3, Ki-67, and PTEN have wide variability in this setting during specimen collection and processing across multiple centers, highlighting the challenges inherent in these pharmacodynamic studies and the need for standardized collection, processing, and ascertainment of these markers, with consideration of final sample size based on evaluable tissue"
Conclusions—At 3 mg daily, rapamycin successfully and safely inhibited PC S6
phosphorylation and achieved relatively high prostate tissue concentrations. No effect on AKT
phosphorylation or tumor proliferation or apoptosis was observed"
Yeah, better hope on other meds or higher level treatments…the clinical history of rapamycin alone and metastatic cancer is not good. I think we need to think primary prevention with rapamycin…stopping cancer from starting.
4 Likes
Unfortunately, the best options will probably end up involving gene therapy.
1 Like
“An exciting study discovered that elephants have 20 copies, that is, 40 alleles, of the TP53 genes, compared with the typical number of one copy found (so far) in all other mammals. Despite the large body size and long-life span, elephants exhibit a high resistance to cancer as cancer mortality is estimated to be <5%, as compared with humans reaching up to 25%”
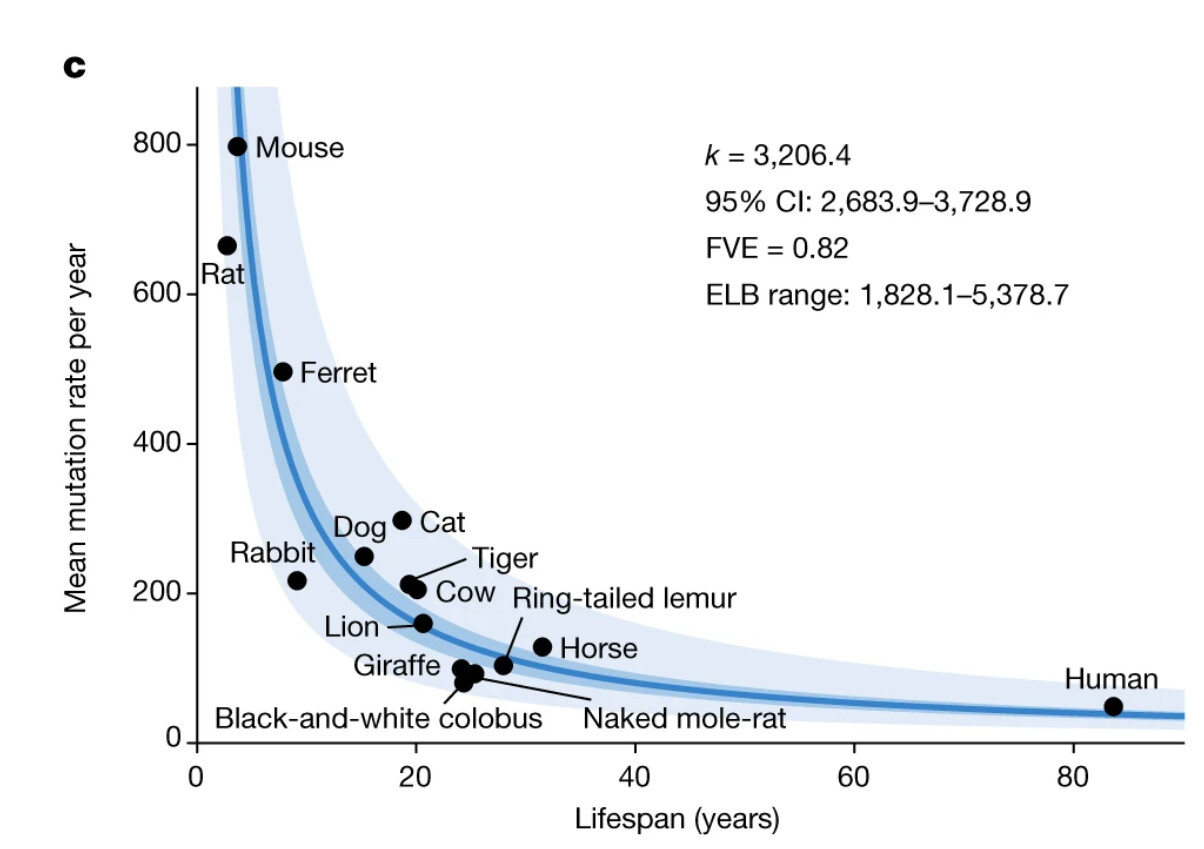
Lifespan is also inextricably tied to somatic mutation rate. Elephant was not studied. We know mice have insanely high mutation rates, yet live a very short lifespan. Rapamycin extends that lifespan…mechanistically, what’s in play? Is it actually SLOWING down the intrinsic aging rate…or perhaps deferring the impact of these mutations to later? Looking at human way down the mutation rate axis (vs mouse)…how is rapamycin going to reveal itself within our lifetimes?
https://www.nature.com/articles/s41586-022-04618-z
@tongMD how to reconcile our (human) heterogeneity in genes, cancer, somatic mutations, rapamycin, and lifespan extension? Btw, it’s ok if you don’t know the answer ![]()
1 Like
To be clear, elephants (non captive) in those studies have lifespans of up to 70+ without cancer. Considering their body size and no healthcare system, it’s pretty impressive relative to humans
6 Likes
Indeed, maybe we can learn something for translation other than gene therapy! ![]()
Bowhead whales can live 200 yrs…massive size.
But nothing compares to the naked mole rat re longevity/pound and cancer free life. Maybe we could learn more from them? 20+ yrs for a 30g rodent.
“The mortality rate of the species does not increase with age, and thus does not conform to that of most mammals. Naked mole-rats are highly resistant to cancer and maintain healthy vascular function longer in their lifespan than shorter-living rats. The combination of p16 and p27 in naked mole-rat cells is a double barrier to uncontrolled cell proliferation, one of the hallmarks of cancer”
3 Likes
Well for the bowhead whale one of the many parts is adaptive changes in HDAC1 (and 2) which are associated with senescence, aging, and cancer.
Ultimately, “preventing cancer” isn’t easily separated from “slowing aging” as a mutually exclusive.
1 Like
@tongMD - Agree with this premise. Optimizing tumor suppressors like p53 does seem make sense
2 Likes
Is this the most important post on the forum so far?
I’ve flip flopped on dosing two or three times now but have been slowly building it back up over the last month or so. Next week I will be up to 14mg or exactly 2mg/kg/wk.
5 Likes
Nothing in what @MAC said is disputed. If anything he has one of the most extensive knowledge base on Rapamycin I have seen including the “experts”. I would like to think that the following are points of agreement by most, but always willing to learn with better information.
- We are all guessing at optimal dosing for longevity.
- We do not know exactly what the aging processes does that creates mTOR to be stuck in the “on” position - or lose its flexibility of modulation that it had in our youth.- but descent repeat studies do show impressive longevity results in mice and dogs.
- Most drug dosing has its higher side effect profiles in the peak levels and lower effective therapeutic value in the trough levels. - Rapa seems unique in that even at suicide attempted levels is tolerated well by the body which allows for pulsed dosing as an option.
- Rapa does not completely shut down or inhibit mTOR, but may allow it to rest, reset or improve modulation - so the argument of it completely shutting down mTOR I don’t think is being made
5 If we had a better understanding of the measurable outcomes we are hoping to achieve, then we would better be able to judge different dosing - daily vs. every other day vs. weekly, biweekly, monthly or even a few large pulses through out the year.
I appreciate both @mav and @mac who I think make some of the most sound and logical arguments on this site.
3 Likes
I’ve come to appreciate that the contributors on this site are well informed and make sound arguments. As far as dosing:
- Our end goal is longevity, which in humans will be nearly impossible to determine, so strike one.
- This forces us to search for biomarkers, of which there are few, and are health- related. So we wonder about energy, muscle, inflammation and immunity.
- Or we oddly seek out side effects as possible markers of efficacy like mouth sores, lipids and glucose elevations.
- We rely heavily on mice since that’s where the preponderance of studies have been done, but mice have enormous growth signals, long telomeres with rapid cell divisions, and an insane metabolism of 961KJ per kg as opposed to our 138 KJ.
It may take a walloping dose of rapamycin to slow things down enough in a mouse, and in males it seems almost impossible to overly inhibit mTOR. It’s truly the more the merrier. - The best human examples we have are renal transplant patients and they don’t exemplify the general population…
- What we seem to know so far in humans is that at just 5 mg’s per week the immune system is affected in a positive manner per the Mannick study. We also know that moderate daily dosing gives enough T cell inhibition in renal patients so that they don’t reject foreign organs.
All else at this point is educated guesswork on our part regarding dosing and longevity in humans, and there’s no expert with clear insight into this at this point. And there may never be.
11 Likes
I agree. I think in a couple more years this forum will have enough experience and data regarding the impact of Rapa on human physiology that collectively we’ll actually be ahead of the experts.
9 Likes
@rivasp12 Yes! Well said and totally agree.
Although has been said multiple times previous, we may not know the best dose to use, we do know what doing nothing will do:)
5 Likes
Amen to that. We absolutely know what will happen if we do nothing!
6 Likes
"The time is now unless it’s too late
The overwhelming evidence suggests that rapamycin is a universal anti-aging drug – that is, it extends lifespan in all tested models from yeast to mammals, suppresses cell senescence and delays the onset of age-related diseases, which are manifestations of aging [discussed by me in"
[148,149,158,192].
~ Mikhail V. Blagosklonny
From;
4 Likes
Sometimes I feel 20% is amazing. Most of the time I feel that it’s not enough. But if it’s either 0% or 20%, I’ll take my Rapamycin.
I am so frustrated that the majority of the world just doesn’t care about fighting aging. It seems so obvious to me that this should be a global priority! Most people I talk to about this tell me they’d rather just die at a ‘normal’ age.
9 Likes
Hahaha - 20% of health in average life expectancy of 80 years is 16 years. Think of what has happen in the past 16 years of your life - for me it is a lot!
I will take 16 years more of good health. However, personally I think I am going to get at least 20 more years. Because my family usually is pretty healthy into their early 90’s (Czech stock). One more generation of my family to enjoy!
5 Likes