Hi - I am 61 years old and at the highest risk for heart disease as I got 4 stents in Jan 2023 and had a STEMI in early April and got another stent.
I had Lp(a) of 285 and it seems to be the major factor. I joined Olpasiran trial and must be on low dosage (better than being on placebo) and it is lowered to 154. But still much higher than the required 75nmol/L or lower.
So to lower LDL and ApoB, I am taking
Rosuvastatin 20mg
Ezetimibe 10mg (This was added in April)
My LDL has dropped down 37 from 58 and ApoB 50 from 64
However just following Dr Attia I believe that my numbers should be as low as below 30 for LDL and below 40 for ApoB.
One option is to increase the dosage of Rosuvastatin but I think it would be better to add Bempedoic Acid to the cocktail.
So it would be Nexlizet (180mg of Bempedoic Acid and 10 mg of Ezetimibe) with Rosuvastatin 20mg. If LDL drops too low, I could reduce Rosuvastatin dosage.
Am I evaluating this correctly? Am I missing something?
One of the issues is whether your cardiologist agrees with need for APOB in the 40’s. It would seem sensible, and usually what I’d be goaling for in this situation. It is naturally quite important to be aware that even with this, you are still at significant risk of more events for probably the next 5-10 years. Getting something you can follow for vascular disease regression/stabilization would be nice - such as carotid intimal thickness, as most of the time what is happening with those is going to happen elsewhere.
I’d talk with your Cardiologist on their thoughts of whether to maximize the statin or add another agent, in the event they agree of benefit to lowering this more. I personally would maximize the statin.
Alternatively, a PCSK9 might be on offer. Kaiser does a pretty good job of being sensible. If you don’t meet their criteria, the secondary question would be, “would it be harmful for me to take a PCSK9 inhibitor if I paid for it myself?”
If the answer is that it would be fine and not harmful, then you could chat with others on the board as to where they obtain their’s cost effectively and choose if you go off shore for these.
You have lots of options - I think the big ask is having the cardiologist feel you need an APOB in the 40’s. I think that is the correct target - but they will be stuck within certain guidelines.
You can also ask, “outside of the guidelines that typically apply evidence based cost effective care, if you were making a decision for your spouse and money was no object and you didn’t have to stick with any guidelines, what would you do?”
Dr Fraser - your diagnosis and analysis is ALWAYS SO CONCISE and right on the mark.
Why do you believe in maximizing statin?
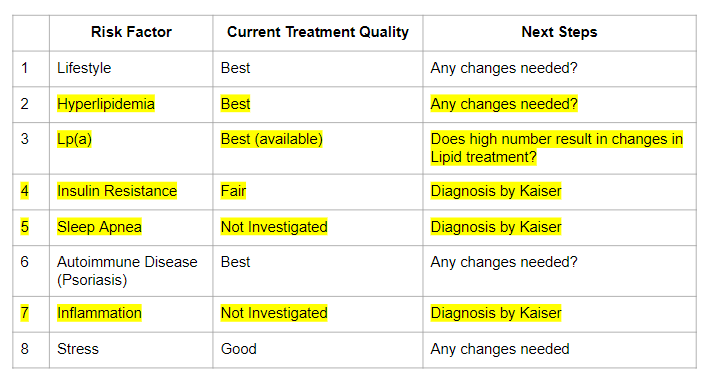
You have given me enough to have great conversation with my cardiologist. I am also looking at all other Risk Factors but I think Lp(a) is probably the most dangerous for me…
From a plaque stabilizing standpoint, and anti-inflammatory perspective, I feel we have the best data for someone who already has disease. Along with that, making sure you maximize insulin sensitivity comes hand in hand with this. This is where I often use a combination of things together that each have a beneficial effect and mitigate the bad parts of another drug. For example an SGLT2-i with a statin and rapamycin, +/- a GLP or acarbose. Add some Telmisartan if you have enough blood pressure for it’s improving of insulin sensitivity and neurocognition … Those a simple measures to consider as a package deal with each having unique longevity benefits, vascular health benefits while blunting the bad aspects of another drug.
Don’t forget the “new” medicine that was just approved as the first (and only) anti-inflammatory medication for cardiovascular disease event reduction – colchicine 0.5 mg/day (in its branded variation called Lodoco), or 0.6 mg/day generic. This should have additive benefit to what you’re doing to lower lipids.
Also, getting a PCSK9 inhibitor from overseas won’t work unless they can ship it under refrigeration. Maybe Canada?
That’s strange. What would be the mechanism? For bempedoic acid, this review says:
“the incidence of UTI was 9.3% and 9.6% among women receiving bempedoic acid and placebo, respectively; the corresponding incidence in men was 3.0% and 3.3%.”
So if anything, a nonsignificant decrease in UTI from BA. And I’ve never seen ezetimibe associated with UTIs (and again, can’t think of a mechanism). Could it have just been a coincidence that you got a UTI after starting the combo?
It could be a coincidence, but I don’t think so as it’s not typical for me to have a UTI. I’m very sensitive to medications in general and often have rare reactions.
Side Effects:
While UTIs are not commonly associated with bempedoic acid/ezetimibe (Nexlizet), some side effects reported include:
Urinary tract infections (UTIs): Seen in about 5.9% of patients taking Nexlizet.
Yep you’re right – 5.9% vs 2.4% in the placebo group, per the full prescribing info for Nexlizet, but increased risk of UTIs weren’t seen in clinical trials of ezetimibe or BA alone. Strange.
My thoughts on this are that regardless of guidelines if I were you I’d want my ApoB/LDL as low as possible.
I don’t think you will find significant improvement by moving from 20 mg to 40 mg of Rosuvastatin, 90% of the benefit of this medication is achieved in the 10-20 mg dose range, then the curve flattens out. But the stress on your liver will be significantly increased by doubling the dose.
Ezetimibe stresses your liver also so if you find your LFT’s bumped with Ezetimibe and Rosuvastatin I’d probably look for other drug categories. Bempadoic acid can cause gout too so again, risk benefit here doesn’t compare with a PCSK9-i
You may be surprised but with the right formatting a letter to Kaiser requesting preauthorization for PCSK9-i use may do the trick. PCSK9-i should lower lp(a) as well and since there are no other FDA approved treatments they may accept use of a PCSK9-i. I’d recommend Repatha since the approved dose can be higher and if you don’t have side affects (very few do) you should maximize the dose (140 mg). You may want to check with your Olpasiran trial as it may not be ok with them since it can reduce your lp(a).
The only other thing worth considering in my opinion is Niacin. Niacin can lower lp(a) significantly if you can tolerate the flushing seen especially with the higher doses. Again your trial may not want you on it and it can have insulin resistance as a side effect in addition to the flushing.
if you aren’t already on aspirin (81 mg) high lp(a) is an indication for that as well.
Unfortunate for you. I couldn’t find any studies to confirm that it is a problem for the combo.
I did ask Dr. Oracle.
“Specifically, it is mentioned that in one study, urinary tract infection was among the most common treatment-emergent adverse events (TEAEs), occurring in ≥3% of patients in any treatment group”
Though it didn’t cite a study, maybe someone else can find one?
I buy the 600 mg Now softgels from Amazon
"NOW Supplements, Pantethine (Coenzyme A Precursor) 600 mg, Double Strength, “Cardiovascular Health*, 60 Softgels
Visit the NOW Store
$29.19 with 42 percent savings-42% $29.19 $0.49 per Count($0.49 / Count)”