Two days after a dose of around 20 mg rapamycin + grapefruit seed extract + 500mg metformin, I had
CK-MM (creatine kinase muscular) 3948 (reference range <171)
CK-MB (myocardial CK) 44 (<25)
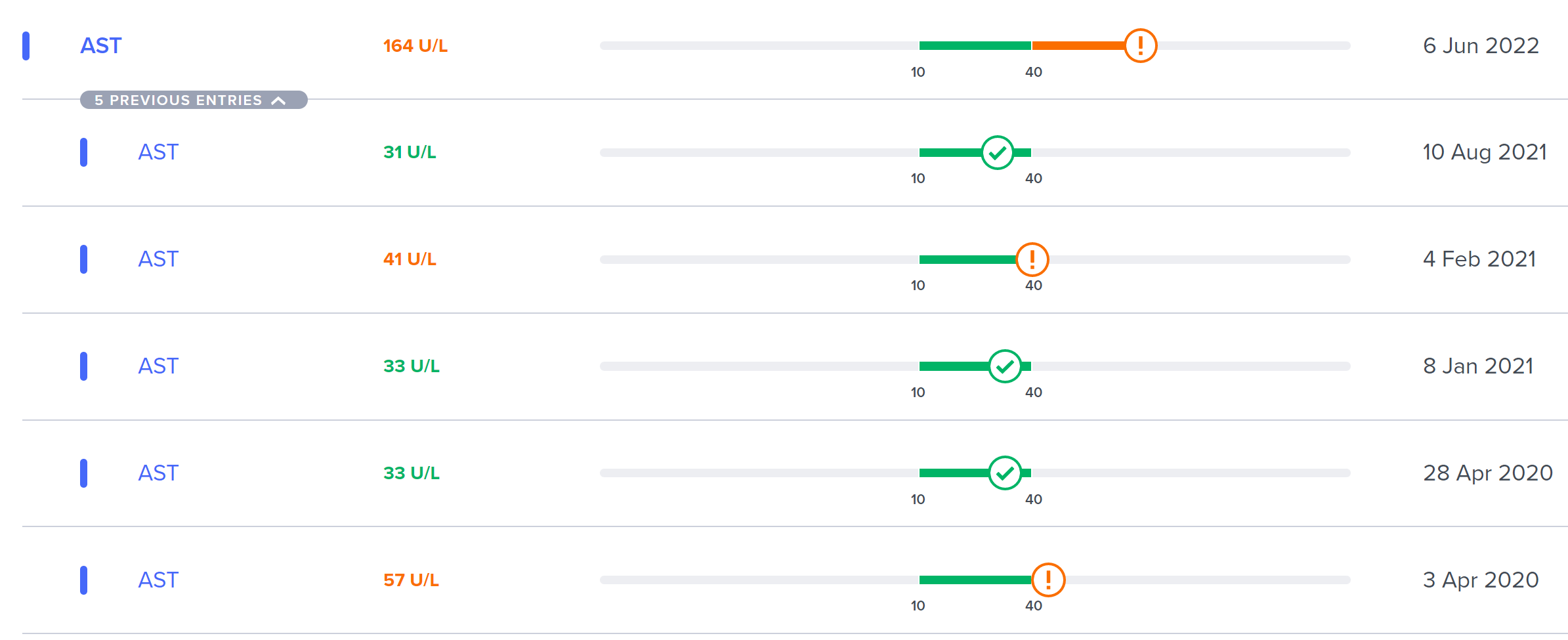
AST 164 (0-35)
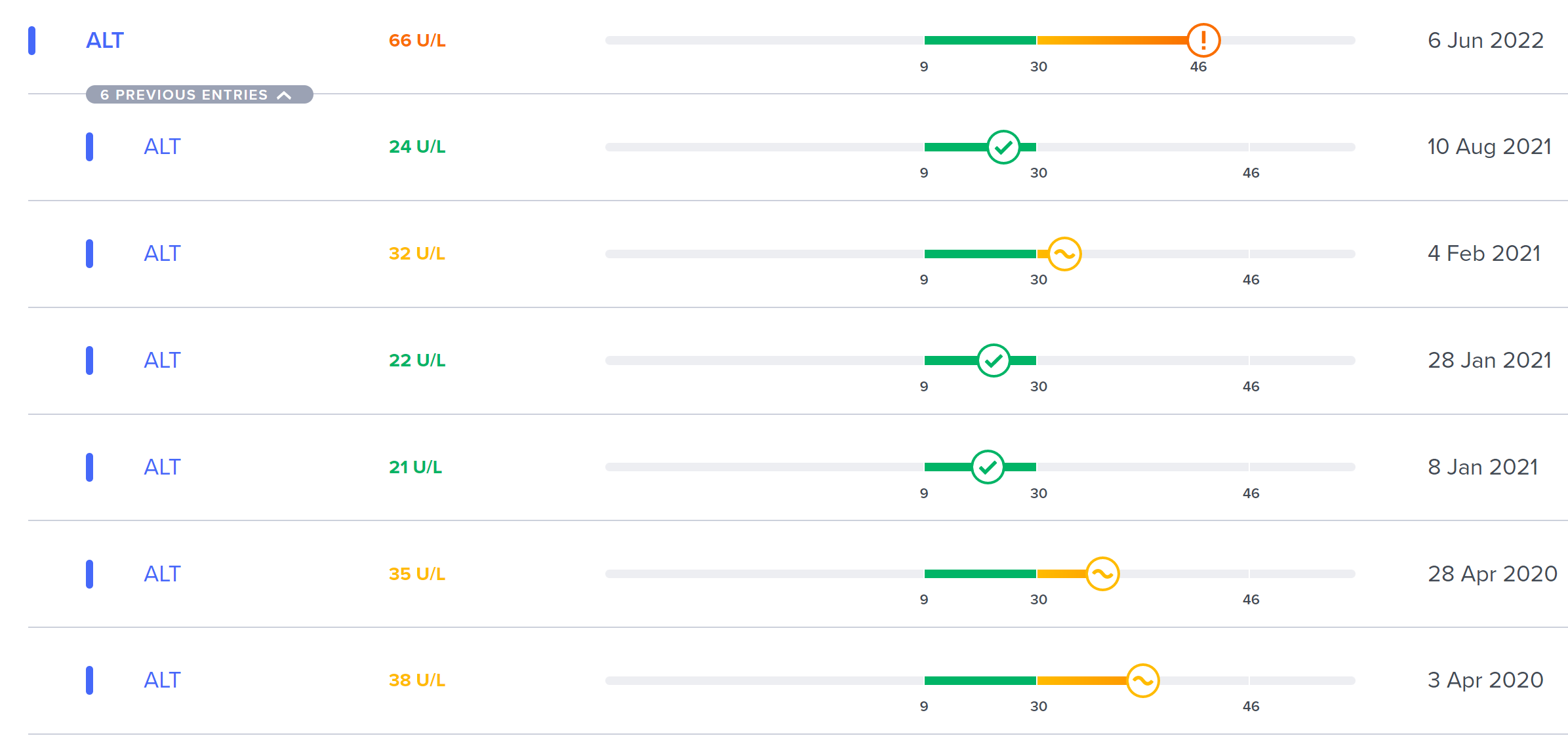
ALT 66 (0-45)
LDH 498 (230-416)
38, male. Full results here: https://docdro.id/A7wzAnW
Taken almost daily: metformin or acarbose with the two meals, depending on what I’m eating.
Should I worry? Anyone has had a similar experience? What should I do next, on top of retesting after two weeks? Note that I’ve always had high CK, yet never at this level:
What is your BMI?
What about health is general? Metabolic health?
What was your exercise history for the week prior to the test?
Any other drugs or supplements? Even Tylenol?
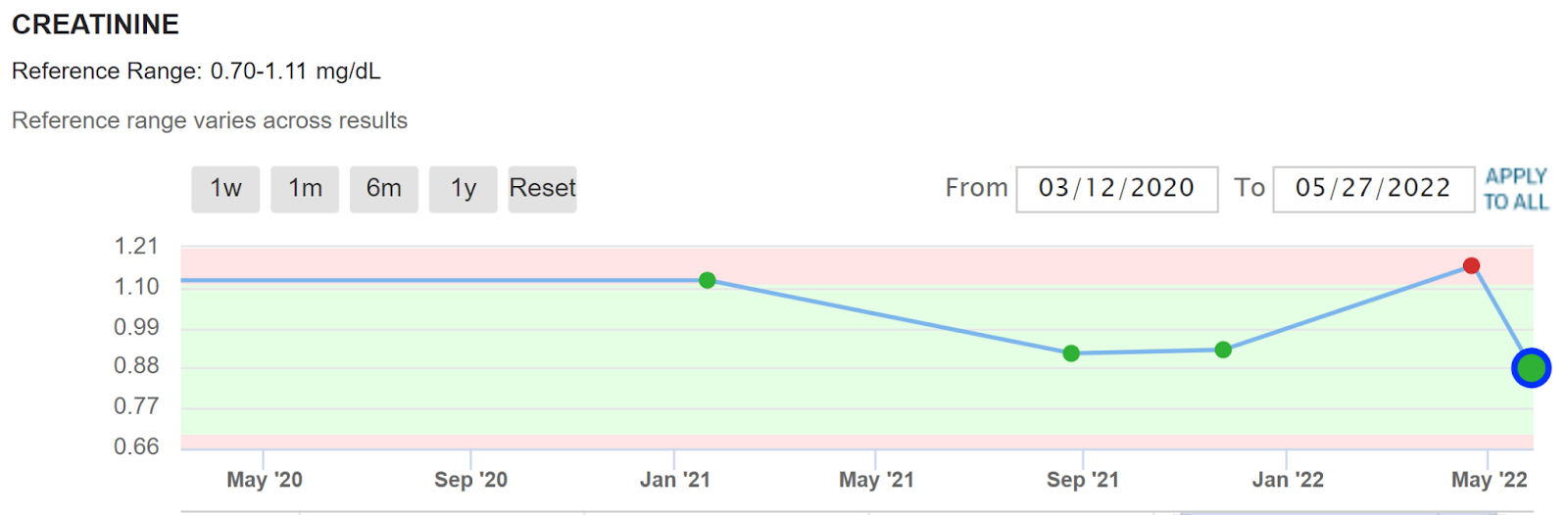
What is your creatinine? (Edit: normal 1.02)
Alcohol use?
didn’t exercise much (I felt weak, maybe because I had a small surgery to remove a molar, and was taking NSAID’s rarely - not in the day before doing the blood work tho’ - and more Metformin or Acarbose than usual)
in the week before I didn’t take much else (except standard stuff like vit. D, zinc at times, magnesium)
The case that you linked seems too far removed from my starting situation.
I did measure BP the night before at 20:27 → 95/44, pulse 62
And two hours before doing the blood draw → 92/48, pulse 64
These kinds of low BP values are normal for me.
And while I’m not proposing there’s a smoking gun here, this is certainly a case that gives me some hesitation on higher doses, especially with grapefruit.
I guess we will have to wait a while for the studies to be completed to actually know the full range of side effects and their frequency.
Meanwhile, when I upped my rapamycin dose from 5 mg/week to 10 plus/week, my creatine levels took a nose dive into the more normal range.
(My dose has varied from 10 to 20mg/week with grapefruit juice to find the max dose I can take without adverse side effects)
I plan to test every two months.
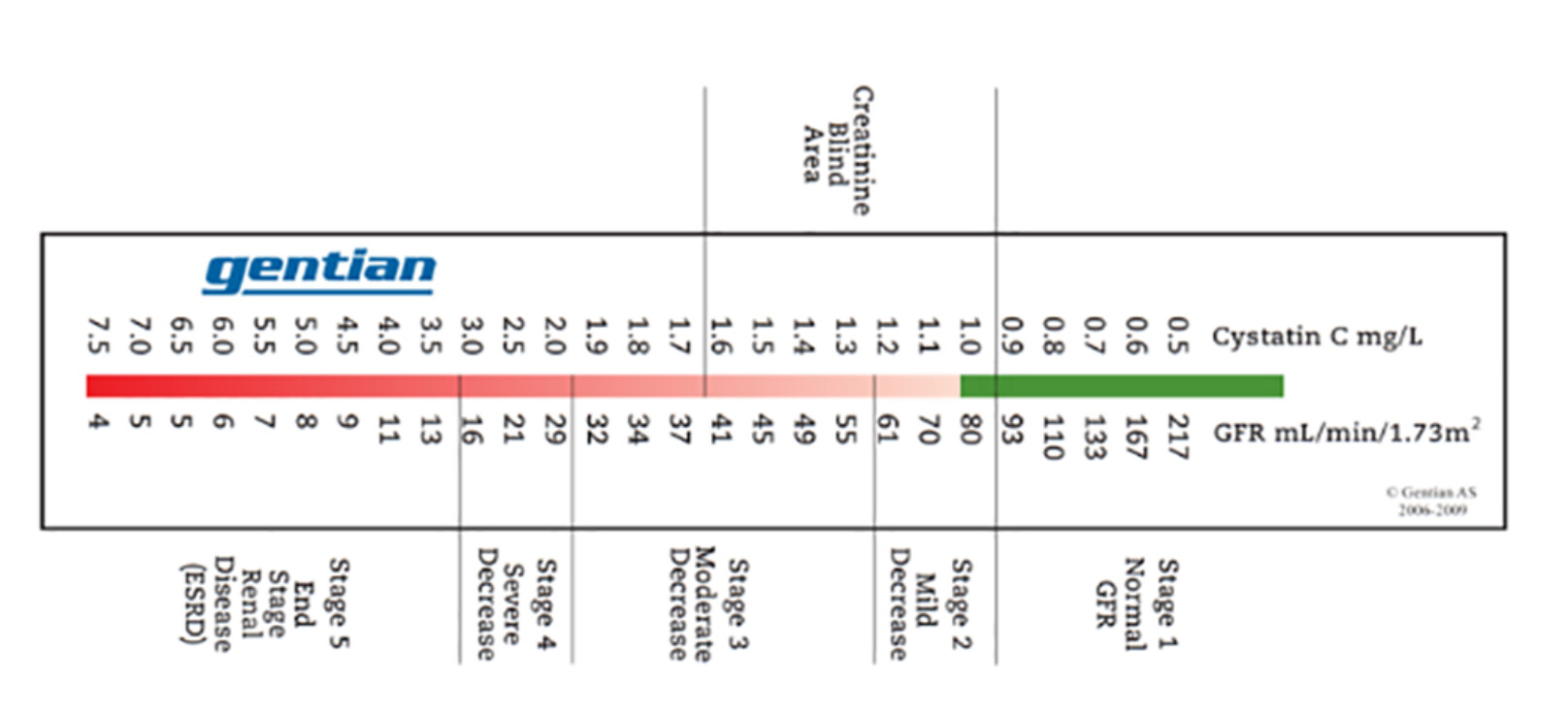
In many rapamycin/kidney transplant/cancer studies, all manner of kidney function is measured for efficacy. Any insight if Cystatin C could be an efficacy/mTOR marker?
I certainly think Cystatin C is a more sensitive test for GFR than creatinine, especially in the “blind area” where creatinine has proved unable to accurately correlate to early stage KD. Without other diagnostic criteria being met, creatinine alone is almost meaningless for GFR ~45-85. For someone who is showing very mild renal impairment (perhaps age 70+), tracking improvement in renal function against Cystatin C will probably be a more reliable and stable marker to track.
This graph nicely shows the “creatinine blind” region where GFR isn’t really reliable based on creatinine alone. If you’re in that zone and looking for faint markers of improvement, Cystatin C is your best bet.
Serum cystatin C as a marker of renal function in detection of early acute kidney injury
“We studied 200 healthy subjects and 130 AKI (acute kidney injury) patients over a period of 2 years at a tertiary care hospital. Serum creatinine and serum cystatin C were studied and analyzed in relevance to early AKI. We found that 56.2% of patients of AKI group had normal levels of serum creatinine in early phase, while all patients had elevated serum cystatin C at same time. Multiple logistic regression analysis revealed cystatin C-based GFR reflecting decline in GFR with worsening AKI in better than creatinine-based GFR”
But what I’m looking for is how to use sensitive kidney (or liver) markers as a MARKER of mTOR inhibition.
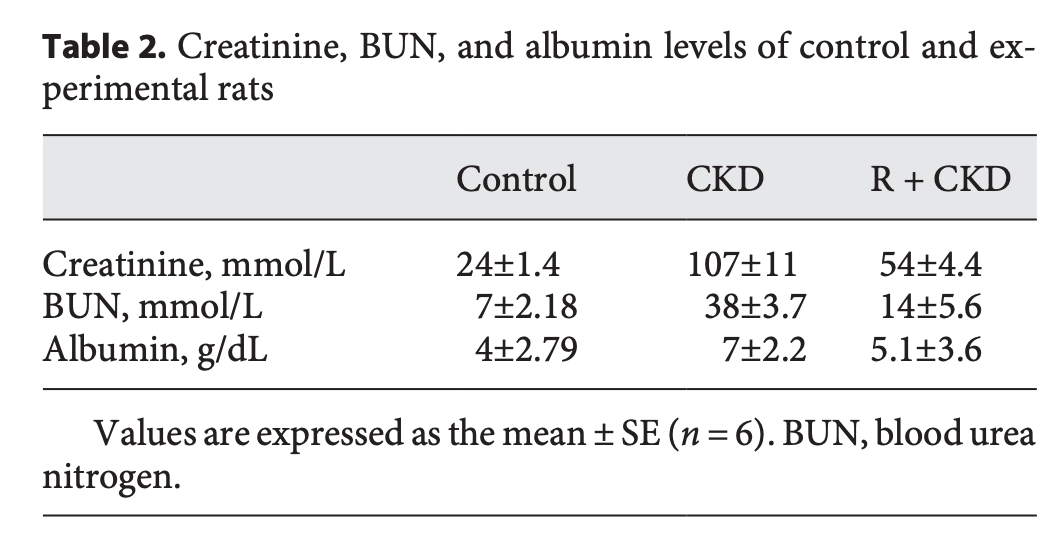
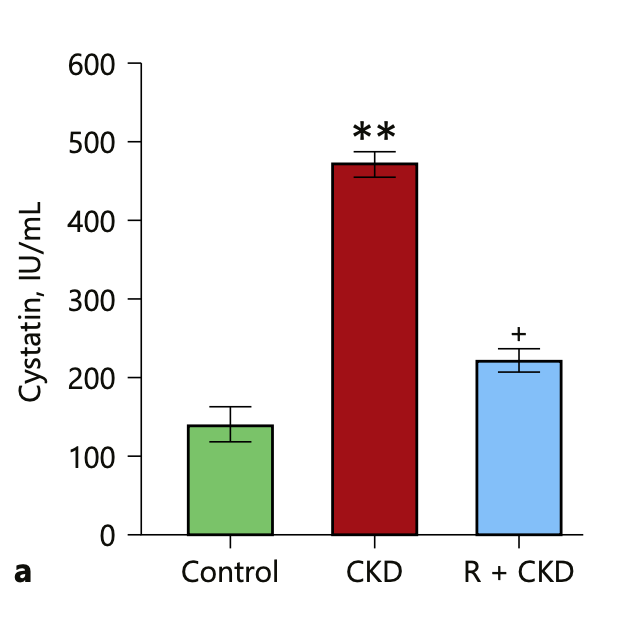
Attenuation of mTOR Signaling Is the Major Response Element in the Rescue Pathway of Chronic Kidney Disease in Rats
(They didn’t do a Control + Rapamycin only)
The current investigation was undertaken to study the role of mTOR-mediated signaling in CKD using Wistar male rats and adenine-induced CKD as an experimental model. The results suggest that mTOR inhibition significantly attenuated the induction of fibrosis, with restored serum creatinine and blood urea nitrogen levels. Activation of mTOR is the major responsive element with activation of miRNAs as an elementary role in the progression of kidney disease. Hence, targeting mTOR would be a possible strategy of treatment for CKD. Rats injected 1mg/kg for 5 days. The serum levels of creatinine, BUN, and albumin in CKD were significantly increased compared to the controls (Table 2). Rapamycin pretreatment exhibited reduced levels of these blood analytes in the CKD animals, but they were not equivalent to the control animals"
I did another comprehensive blood and urine test on July 4th. The problematic biomarkers are much improved, even though others are slightly worse (probably because I’ve been driving a lot through Europe: worse sleep, and I feel the negative effects of pollution through congestion, nasal irritation and sneezing). The biological age as judged by the Levine spreadsheet is higher (worse).