The minimal level we see in the literature where organ rejection in combination with other agents, is avoided is a sirolimus level of 3 ng/mL. Monotherapy needs to be 8-12 ng/mL as a trough (lowest level).
I think it is reasonable to think that threshold of 3 ng/mL and above is providing a therapeutic inhibition of mTORC1, but fails to some extent below that. So my approach has been to have weekly dosing patients get a 20-24 hr level of ~6 ng/mL. That usually works out well - doing a level at 48 hours after usually has a level <3 by a bit.
Single doses have a T1/2 more in the range of 24-36 hrs, it is only daily dosing that has the longer T1/2 of 63 hrs.
For folks doing dosing for neuroprotection - we sometimes push this up and go for a level of 9 or so, and then dose q14 days.
Again, lots of assumptions - and I’m just telling you how I usually do things with my patients in this space.
What I’ve been finding is someone who is 120-150 lbs usually does well with 7-8 mg to get a sensible weekly dose, and then our 150-190 lbs usually 10 mg, and above that usually 12 mg. That would be what I’m observing from data coming back from my patients and myself.
There is some variability in levels, but most are coming in to a reasonable range I’m happy with for weekly dosing with this.
I’m not certain I’m an expert yet - but I get to see a lot of levels. My last was 5 mg with GFJ 8 oz 3 hrs prior, then 4 oz with. I know my metabolism is around 30 hrs for T1/2. I had a 20 hour level of 9.5, so essentially 1.7 or so more half lives to get below 3 ng/mL. So 51 hrs from that level, anticipate not being therapeutic, so total time from dose to non-therapeutic is 71 hours give or take. I goal for ~30% of the time above this threshold, so I’m pretty happy with a dosing interval for myself with this of 10 days.
This is simply that way I’ve chosen to put some structure on this, until we have better evidence of pros-cons of rapamycin, and dosing.
#1 Elimination half-life, getting a 20-24 hr level, then another one in 48 hours gives a good understanding, and there are certainly individual variations to a modest extent. We can get a good estimate of T1/2 with having these 2 values. If you look on ePocrates, for example, they give T1/2 62h or 113h with impaired liver function. They also used to list single dose half life of 35 hrs.
I’ve not used everolimus, no good reason, apart from cost in the U.S. generic is a lot more than sirolimus. Certainly the shorter half life could require higher or repetitive dosing, depending on goals, and I don’t have experience with that, and would be unclear on the advantage of going to everolimus. I’m sure once can accomplish the same thing with that, I’d just need to map it out with levels, IF one buys into the theory that a serum level above a certain threshold is a sensible thing to achieve and maintain.
I’m at 170 lbs, 4 mg with GFJ every 14 days, with levels still a little high at 100 hrs in the 4.5 ng/mL range. So I often end up going to 21 days between doses. I will probably drop to 3 mg with GFJ the next time I test.
For patients doing this weekly, I test at 50 hours post dose and goal for ~3.0 ng/mL. There is variation between tests and overall, I have enough data to know this approach is safe, I cannot confirm efficacy as this is a challenge in a single medical practice rather than a long term research environment.
Average dosing without GFJ for weekly dosing in my patients comes to 0.1 mg/kg/dose. The issue is there is a lot of variation around this, with some individuals needing as high at 0.3 mg/kg/dose to be at our desired blood level and others being almost as low a 0.05 mg/kg/dose.
So testing a level is sensible. Taking it the same way every time (I usually advise with 1 oz of nuts or 15-30 mL of EVOO) is important for consistency.
Unless you weigh 30 kgs, I’d suspect your level will be low by how I dose my patients. You might have a few hours of mTORC1 inhibition if you are average weight, but I’d guess on redistribution you’d quickly be below 3 ng/mL.
Why do you use GFJ instead of just increasing the dose? I briefly used GFJ to extend my sirolimus supply, but was concerned that the effective dose wasn’t reliable.
I can conserve my supply, and it has been reliable and consistent on my testing. There has been no more variation in results that with people taking it without GFJ. It’s important you do it the same each time, regardless of whether your use GFJ or not. Generally with some fatty food (1 oz of nuts/1 tbspn of EVOO) if not with GFJ, and with GFJ, we usually do 8 oz 2-8 hours before, then 4 oz with the rapamycin. With monitoring levels every 3 months, we see the values and they’ve been pretty consistent, at least as much as with people taking it without GFJ.
That’s just my experience, including in a number of patients. There may be folks who this doesn’t work well for, but with monitoring levels you can see if there is consistency and the desired result.
By consistent, do you mean that values measured after intake of the same standard dose of rapamycin with GFJ in the same person don’t differ much between different tests (e.g. levels 48 hours after a dose is close to the same from dose to dose)? That would mean that the variation in CYP3A4 inhibitory compound ingestion from the different GFJ batches is either not high, or if high the dose of those compounds is usually far enough above the treshold for inhibition to result in a strong inhibition regardless of the batch. Am I understanding it correctly?
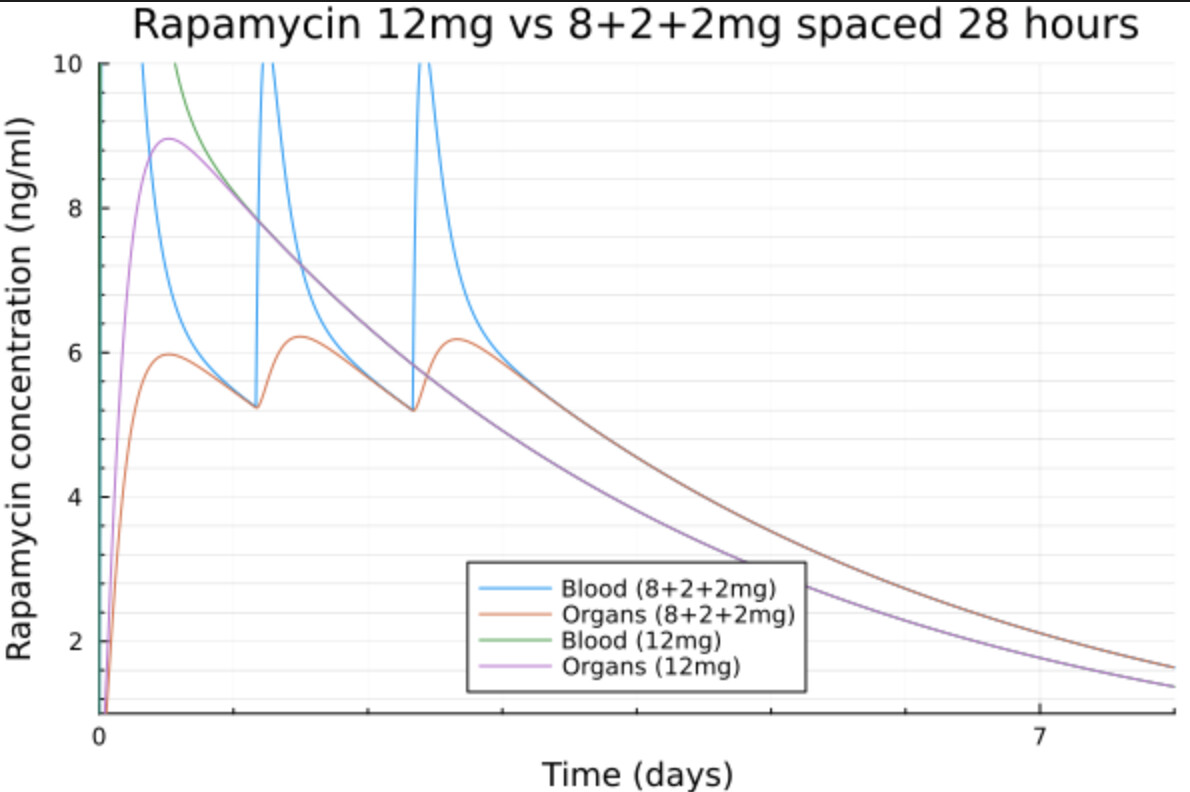
Looks low to me. I’m using 12mg every few weeks in a split dosing protocol to avoid having a peak level too high.
I use 8mg + 2mg + 2mg spaced 24 to 28h. That gives me a max level of 6ng/ml and 6 days above the 3ng/ml threshold.
When I take a high dose, my hepatic glucose production goes through the roof for almost 2 weeks. This could be done to the high dose rapa messing up with the pancreas beta cells producing insulin, making the liver insulin resistant or both. By splitting the dose, I get a similar or slightly higher AUC without that high peak and my glucose is less impacted.
By doing that I stay 4 days above 4ng/ml and 6 days above 3ng/ml.
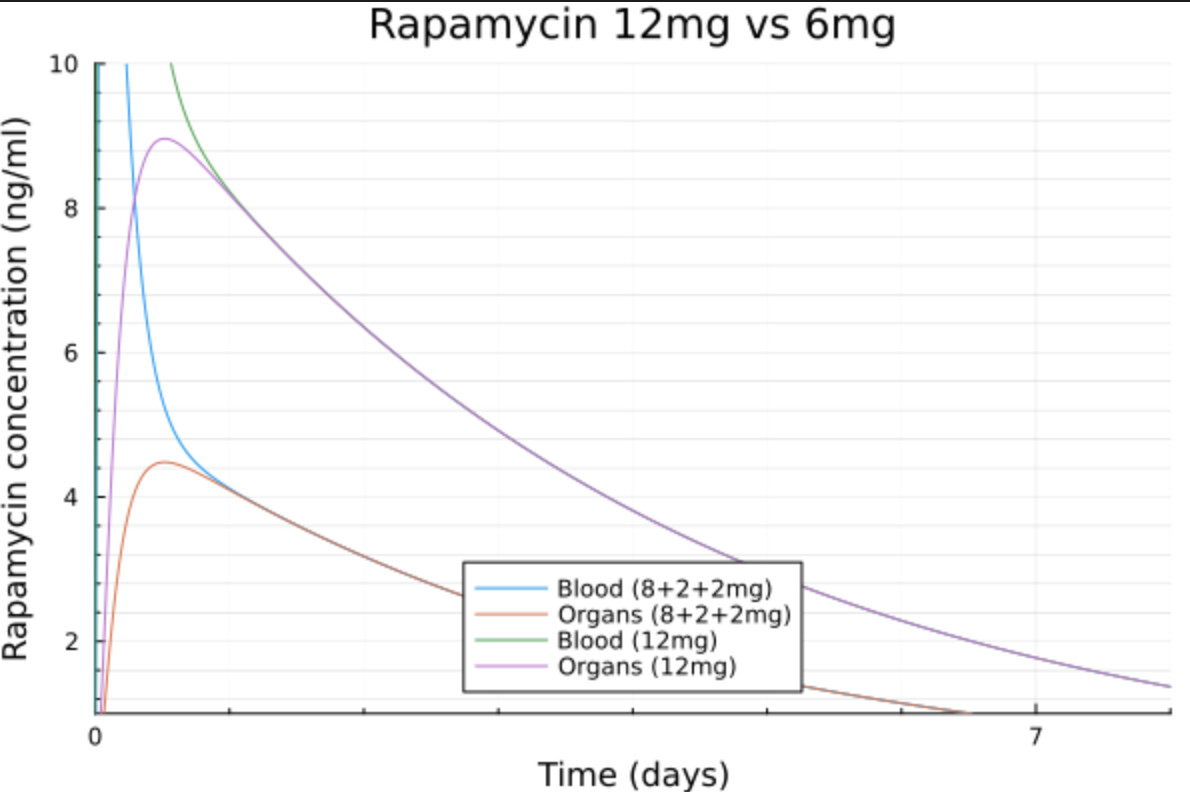
Compared to that, the popular 6mg dose goes only slightly above 4ng/ml and 3 days above 3ng/ml.
So the split dose gives me a much bigger AUC without the side effects I get with a high peak.
Obviously all that is purely speculative.
Whats the usual multiplier for GFJ? x2? x3?
And very important - what is your advice for monitoring the levels? At which timestamps from the starting point? I remember you suggested that 30% of time between doses should be below 3ng/ml. What is the desired levels then at desired times?
Ofcourse it would be great to achieve this information with minimal amount of tests…Price matters)
And, yes, I have to think about how to get desired numbers with smaller doses. Rapamycin is very rare and not easy to find here…Thats why I try to use GFJ. 2mg + GFJ, hope to get equal to 4-5mg. AI counted that if i’m ordinary “consumer”, so I have around 50-62h of t1/2, it will give me around 30% (25 % to 35%) of trough below 3ng\ml. Im around 97kg.
One thing people should look at is rapamycin levels (and symptoms) at 4 weeks vs 1 week, when dosing weekly. The long half life of this compound means that complete washout occurs after 10 to 14 days. So at 7 days, you would still have 12 to 15% of the previous dose on your bloodstream in theory.
A complete washout is not necessary, but if you stsrt getting symptoms of m-TOR2 inhibition after some time on the same dose, then it’s time to look at decreasing it.
Doctor, I just accidentally found your youtube channel))) And saw several very interesting videos) https://www.youtube.com/@DrApoE4
Subscribed! May I ask you offtopic question? For how long is it ok to take doxycycline to help omega-3 to get through BBB? My case is I’m 45, so, is it wise to start 20mg doxy now for decades, to support my AD-prevention? Any downsides or additional benefits? Maybe you can even answer in a separate topic? Because its a very important information…
So I’ll try and answer a few of the questions - I’m quite time poor these days. Doxycycline is a speculative therapy, and in humans we have enough information to say it seems to protect the BBB. Then comes the theory, on this probably helping have normal Omega 3 transport; which we have logic, but not proof, and nor is it likely that we will have proof on this without someone doing a pretty expensive study and for example labelling fish oil and seeing difference in translocation into the brain with a month of doxycycline vs. none in ApoE4’s.
It’s a relatively benign treatment, but as with anything I speculate about, chat with your physician, as some of the items won’t end up working out, and others will. The big issue is safety and cost when looking at what to consider actually pursuing.
In regard to @qBx123Yk suggestion in regard to getting 4 week levels after I’m presuming a single dose … I can tell you I’ve had patients who have accidentally done this after taking what would be a weekly dose that proved at 50 hours to have a level ~3 ng/mL. Every time I have this … the level even at 8 or 9 days has been <1 ng/mL. Single dose pharmacokinetics seem to result in a shorter half life would be my observation.
Now on the question of the typical multiplier w/ GFJ in my testing, it looks like the average is a 3 fold increase. But make sure it is the same brand of GFJ each time and that it isn’t GF Drink - that has little GFJ … we’ve seen this also.
We don’t suggest that 30% of the time between doses should be <3 ng/mL we suggest 70% of the time should be <3 ng/mL. Only 30% of the time above 3 ng/mL. I’ve not pursued more aggressive dosing, so I don’t know the safety of going beyond this. Individual members of this group often do things for themselves, that I’d not do for patients, as safety has to come first. I have enough data to know that what I’m doing is safe. I do not know that what I’m doing is effective as that is a very complex question to answer with Rapamycin. I can tell you that as compared to the fixed dosing that has been typical … e.g. such as everyone gets 6 mg/week … my patients are on more than this … so I am being more aggressive in dosing than many of the mass produced plans that aren’t targeting to levels.
@cl-user Makes an excellent point … go for high dosing, it’ll be around long enough to inhibit mTORC2 … and then we have adverse lipid and metabolic effects.