Hi Everyone! New to the group, but have been excited to see all the info and feedback from everyone. Recently received my sirolimus and my plan is to start at 5mg/wk. I just got an enhanced lipid done to get a baseline and am a little concerned with my APOb and LDL #'s which I’m not sure if I should be at this point or if I should attempt to bring in line prior to starting. Any feedback or input would be greatly appreciated. My info below:
Male / Age 39 / 190lbs / 6ft / cardio daily
Lipid Panel:
LDL 121
TG 170
HDL 70
APOb 103
Could be one off but wanted to get a baseline. Thanks
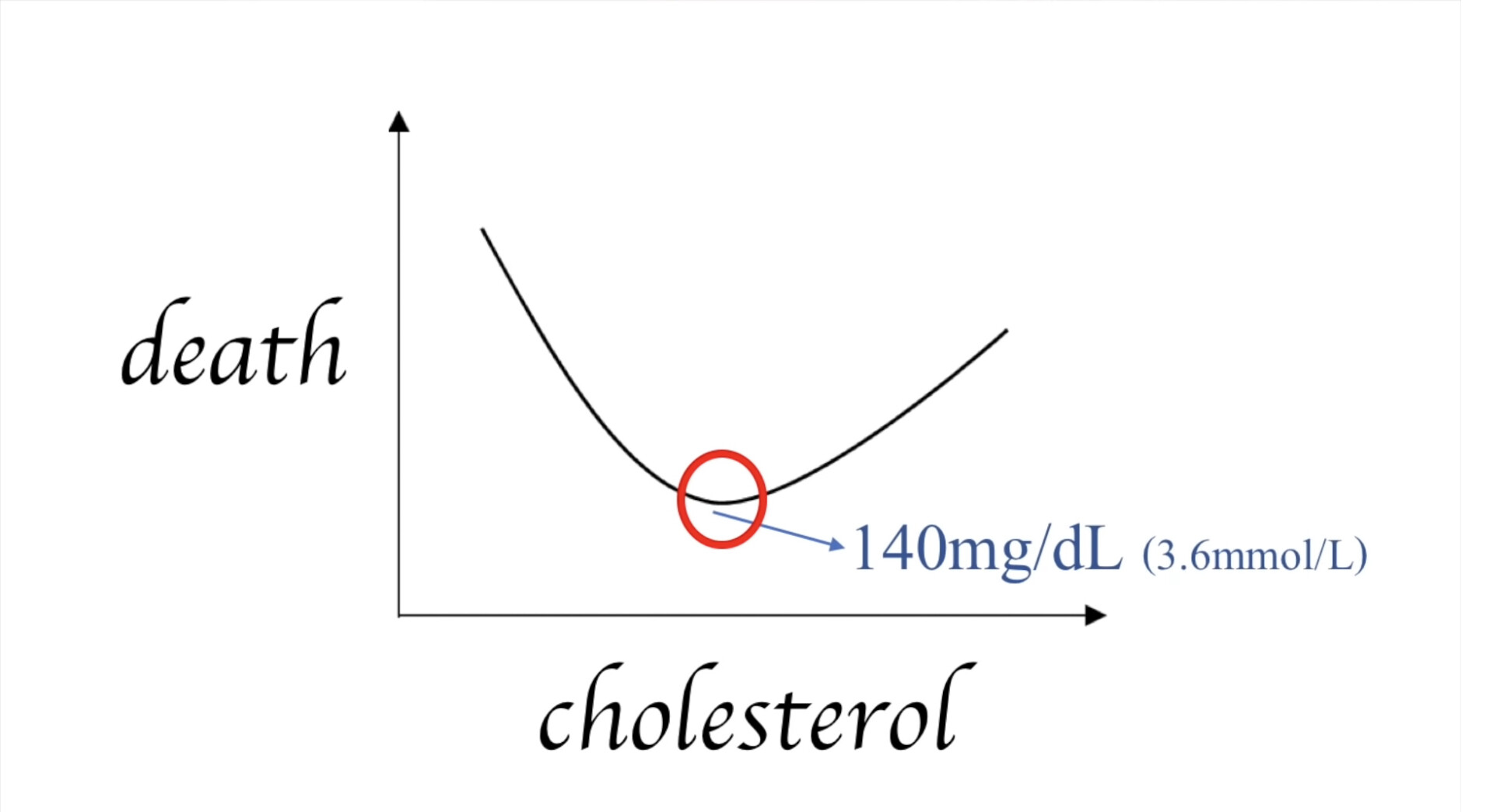
Opinions will be all over the place here. Lustgarten says all cause mortality is lowest for ldl=140. So I think yours is perfect. HDL is good too. ApoB isn’t terrible. It looks to me like you should lower TG, and the best way is to eat less carbs or take acarbose with them.
If you don’t go crazy with the Rapa it shouldn’t mess things up much, but I bet it makes things worse. You’re pretty young, so I think you should be more cautious. I have good luck going every 2 weeks. As I age I may increase the frequency. I’m 62.
Yeah the people with lowest LDL have cancer, liver disease, absorption/gut problems, filled with parasites, and a host of other things that isn’t controlled for. That’s why all cause mortality is lower for a higher LDL. It’s because of disease that is lowering LDL and at the same time increasing all cause mortality.
Would lustgarten also choose to be overweight, have high blood glucose (diabetes), and high blood pressure? Since low weight, low glucose, and low blood pressure make it look good…
Mendelian randomization suggest an LDL of that will have about a 70% less likelihood of living to 90th percentile.
My LDL and Triglycerides shot up 50% after 3 months on rapa. Your experience may be different but this is not an uncommon result. The rule of the site is generally not to tell other people what to do but my personal approach would be to bring lipids inline prior to starting. I am trying niacin and citrus bergamot to achieve this. Hope this is helpful.
Of course, it seems dosage dependent. After going to 5mg/week, with the exception of the LDL, I have been able to get my lipids into the normal, if not ideal, range. I have been trying to mitigate this by taking some additional supplements. If I do not get the LDL back into the normal range, I will lower my rapamycin dose.
You might also want to consider titrating your dose up. I believe that most people in this site do that. It might be prudent to see how your body reacts to a smaller does then work up. I started at 2mg and got quite a bit of acne then moved up to 4mg then 6mg and haven’t had any since.
I started with very high doses and worked my way down. I have been taking rapamycin for~ 20 months now. Starting in early November 2021, I have remained on various doses for ~ 3 months at a time. I change doses after lab tests. For me, at least higher doses equal worse results.
I just got my blood panel results and my ApoB was 138. I was quite concerned until I found the video above suggesting 140 is ok. My takeaway isn’t “phew - all good!”, rather it’s clear I need to learn more about all this.
There were other red flags - especially high Immature Grans (0.3) which is particularly concerning because it suggests possible infection (Bad - I have a large metal implant replacing half my femur plus a hinge for a knee. Infection is the largest concern, potentially requiring a new implant) or a marrow problem (Bad, because the reason for that implant was Chondrosarcoma, a cancer of the internal structure of bone). I also have borderline anemia (unrelated to iron or B12), which has been a mystery to doctors for decades and is probably “just me” but possibly also related to everything else.
Adding this extraneous info because I’m trying to keep these various moving factors in context with each other.