Pantethine is a form of b5 that is not rate limited. My problem with it is that it is so good at reducing the negative effects of alcohol that i drink more and i start out as a relatively heavy drinker
FWIW: From personal experience just taking low-dose naltrexone(LDN) will cut down your desire to drink wine. Definitely blunts the good experience ![]()
1 Like
Another thread here said Dr. Green was taking 20 mg every two weeks, not weekly.
Let’s verify this.
Anyone know the reference?
It would be interesting to know what Pantethine alone will do to your numbers. Based on the article you linked and the one I found below, it can lower LDL-C by 20%, but only lowers ApoB by 4 mg/dl. Of course, the ranges we’re talking about are different; these were people who already had fairly high LDL-C of 150 mg/dl after a 4-week low saturated fat diet before starting the Pantethine. A statin might be the only option for someone trying to cut ApoB in half, from 60-70 mg/dl to get down into the 30-40 mg/dl range.
Radiata, I’ve been using Pantethine for more than 5 years. It lowers my LDL-C about 12% at a dose of two 450 mg capsules daily (morning and evening with meals). Your second reference notes the 900 mg daily dose somewhere I believe and the reason I take it with meals is because the supplement label recommends it. I use the Jarrow brand. I may now consider experimenting with only one 450 mg pill and take it before any food to see if it has a better effect than my current method, but that just means more blood testing … so … maybe I’ll put that on hold for a while since I already know what I get with my current method.
1 Like
B5 is a CoEnzyme A precursor and Panethine is non rate limited. The disadvantage of this is that blood clotting may not proceed as quickly. However, otherwise it is quite helpful. I take it to accelerate the conversion of Acetaldehyde into Acetate.
“lipid-lowering effects of pantethine are most impressive when its toxicity (virtually none) is compared with drugs.”
1 Like
After my last blood tests, I discontinued taking a 40mg dose of Lipitor daily. I am taking 600mg of Pantethine in the mornings. I will be having my blood tests again approx. once a month. If the Pantethine alone doesn’t keep my lipids as low as I want them, I will try adding spirulina. Spirulina hasn’t been studied that much for lipid-lowering effects in humans it seems to be effective in the studies that have been done.
Spirulina is an anti-inflammatory that also reduces cholesterol and blood glucose levels.
“While there are several
other supplements being evaluated for lipid
lowering and weight loss effects, benefits
from supplementation of spirulina are not
limited to the above benefits but also extends
to its antiviral, anticancer, antioxidant, antidiabetic, anti-inflammatory, hepatoprotective, cardioprotective and immunity boosting
properties.”
“Spirulina is considered to be one of the most healing
and prophylactic ingredients of nutrition in the 21st century [2,3]
due to its nutrient profile, lack of toxicity and therapeutic effects”
A systematic review and meta-analysis of the impact of Spirulina
supplementation on plasma lipid concentrations
re: LPA Genotype test.
Does anyone understand what the result "LPA c 5673A>g Geno Bid/T” means with respect to Lp(a)?
Thoughts appreciated.
Looks like it may mean that you could have the gene for high Lp(a) levels or a higher risk of CVD due to the gene. Might be easier just to get an Lp(a) test done through Marek or some other lab testing service to see if you have it. Did you get this genotype test done specifically for LPA, or was it just included with other genetic testing?
Looks like Tocotrienol might be a good option as well. The same review states a larger effect for Pantethine, with reductions taking place at greater than 4 months of supplementation. That might be the issue with the study I previously found–they stopped the study after only about 3 months of supplementation and didn’t see a large decrease in ApoB. The usual caveat is that these studies probably included people with high lipids to begin with, so its tough to say whether or not we could get the same % reductions starting with relatively low lipids.
Tocotrienols
Tocotrienols are a family of unsaturated forms of vitamin E termed alpha, beta, gamma, and delta.5 The gamma and delta tocotrienols lower TC by up to 17%, LDL by 24%, Apo B by 15%, and lipoprotein(a) by 17%, with minimal changes in HDL or Apo A1 in 50% of patients at doses of 200 mg per day given at night with food.5,85–87 The gamma/delta from of tocotrienols inhibits cholesterol synthesis by suppression of HMG-CoA reductase activity by two post-transcriptional actions.5,85–87 These include increased controlled degradation of the reductase protein and decreased efficiency of translation of HMG-CoA reductase mRNA. These effects are mediated by sterol binding of the reductase enzyme to the endoplasmic reticulum membrane proteins call INSIGS.86 The tocotrienols have natural farnesylated analogues of tocopherols, which give them their effects on HMG-CoA reductase.86 In addition, the LDL receptor is augmented and they exhibit anti-oxidant activity. The tocotrienol dose is important as increased dosing will induce its own metabolism and reduce effectiveness, whereas lower doses are not as effective.5 Also, concomitant intake (<12 hour) of alpha tocopherol reduces tocotrienol absorption. Increased intake of alpha tocopherol >20% of total tocopherols may interfere with the lipid-lowering effect.5,85
Tocotrienols are metabolized by successive beta oxidation then catalyzed by the CYP P450 enzymes 3A4 and CYP 4F2.5 The combination of a statin with gamma/delta tocotrienols futher reduces LDL cholesterol by 10%.85 The tocotrienols block the adaptive response of upregulation of HMG-CoA reductase secondary to competitive inhibition by the statins.5,85 Carotid artery stenosis regression has been reported in about 30% of patients given tocotrienols over 18 months. They also slow progression of generalized atherosclerosis.5,87 The recommended dose is 200 mg of gamma delta tocotrienol at night with food.
Pantethine
Pantethine is the disulfide derivative of pantothenic acid and is metabolized to cystamine-SH, which is the active form in treating dyslipidemia.5,88–92 More than 28 clinical trials have shown consistent and significant improvement in serum lipids. TC is decreased by 15%, LDL by 20%, Apo B by 27.6%, and TG by 36.5% over 4 to 9 months. HDL and Apo A1 are increased by 8%.5,88–92 The effects on lipids are slow, with peak effects at 4 months, but may take up to 6 to 9 months.5,88–92 In addition, pantethine reduces lipid peroxidation of LDL, lipid deposition, intimal thickening, and fatty streak formation in the aorta and coronary arteries.5,88–92 Pantethine inhibits cholesterol synthesis and acclerates fatty acid metabolism in the mitochondria by inhibiting hepatic acetyl-CoA carboxylase; increases CoA in the cytoplasm, which stimulates the oxidation of acetate at the expense of fatty acid and cholesterol synthesis; and increases Krebs cycle activity.5,88–92 In addition, cholesterol esterase activity increases and HMG-CoA reductase activity decreases.5,88–92 There is 50% inhibition of fatty acid synthesis and 80% inhibition of cholesterol synthesis.5 The recommended effective dose is 300 mg 3 times per day or 450 mg twice per day with or without food.5,88–92
https://onlinelibrary.wiley.com/doi/10.1111/j.1751-7176.2011.00576.x
What range of LDL-c are you in? Ie., what was the starting value?
Have you ever had ApoB measured specifically? It can be a pain, given that ApoB isn’t on a standard lipid panel.
There has been a direct correlation between my lipids and ApoB. Unless someone is the exception most people who have low LDLc will have normal or lower ApoB. That is why it is not included in most lipid tests. The insurance doesn’t want to pay for it and my doctor says it’s unnecessary. So, occasionally I get my own. It’s relatively cheap. Ulta Labs charges

1 Like
Yes, this is true in most cases. My friend who is a cardiologist works ATM on a project to validate a formula to approximate apoB for local population from a standard lipid profile. He said it is showing 95% accuracy. I tried my results and measured apoB was within single digit of calculated.
1 Like
You said you were taking the compound formula first. How much of the Compound were you taking? The Compound isn’t as affective as the generic formula thus a higher dosage of the compound is required. But if you were on 14 MG of the Compound and then switched to 14 MG of Sirolimus then you more then doubled the amount you were taking. Im on 15 MG of Compound formula and thats equvalent to about 6 MG of Sirolimus. The avg person on Rapamycin is 6mg per week. This stuff isn’t candy, trying to overdose isn’t recommended.
Radiata, My LDL-C used to be in the low 130 - 135 range with diet alone, but is now 115 with the addition of Pantethine. I don’t have any records of Apo B before I started Pantethine, but my current Apo B is 80. Pantethine is not a miracle for me, but it along with avoiding saturated fats and eating cold-water fatty fish daily keeps me in a reasonable range without need for prescription medicine.
Another thing that may affect some people is low thyroid hormone. When mine is low my blood glucose levels and LDL-C levels go up. An inexpensive TSH (Thyroid Stimulating Hormone) test can tell you if there is a problem there.
1 Like
I have an LDL of 81 and I thought that was pretty good until I saw the video last night by Dr. Stanfield who is taking a statin to get his 80 down to the 60-70 range. He’s taking 5 mg of Rosuvastatin. I may be joining him. 60-70 is my new target.
I am going to do the same in a few weeks.
After I retired, having gained approx 40 excess pounds in the last four years of my job because I was relegated to writing white paper proposals for company I was working for, I went back to the gym, went on keto, etc, etc and worked hard to lose weight and get all of my blood markers within normal bounds.
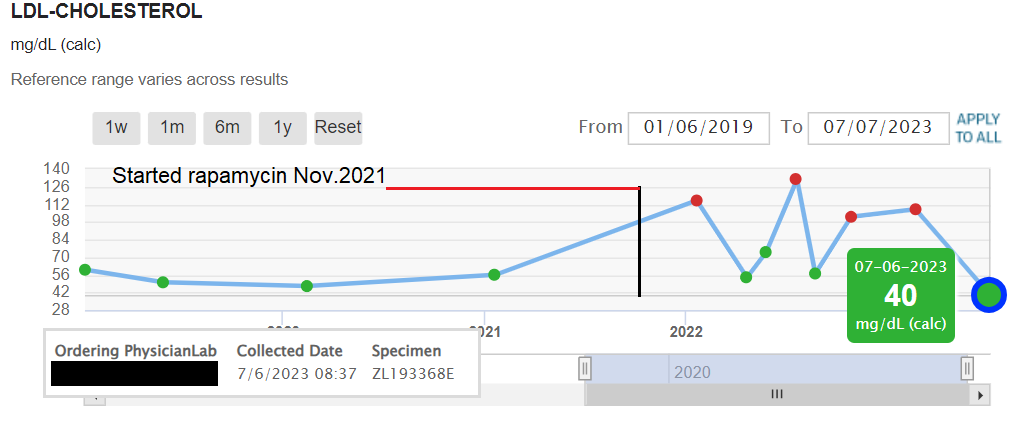
So, yes, I freaked out when my lipids shot above the normal ranges after starting rapamycin.
I do not know exactly why they were all over the place except I that was trying various interventions, diets and rapamycin dosage.
My current interventions are 40mg of Lipitor, 600mg of Pantethine, 18/6 TRF feeding, going to the gym and watching my diet a little more closely. I just stopped taking the 40mg of Lipitor and will see if the Pantethine will keep my LDL-c in the lower half of the graph.
I am only now getting the age reduction results I got from the Levine spreadsheet and Aging.ai calculators. Maybe I have inherited genes that allow me to get my LDL-c so low.?
4 Likes
Desert and all, I’m the dumbest one in the room here. I’m at best a parrot re what we heard on stage at Denver Low carb/metabolic conf.
- Get a calcium scan, if zero then ignore even elevated Apo-B. Just move on.
- During covid, those with elevated LDL had lower symptoms and higher recovery rate.
- Given this; we stuff ourselves with grass fed butter, anything with fat thats grass fed.
- We ignore our LDL, even consider it a blessing to have >>100 LDL
4a) we got our whole body calcium score done at one of those newer EBC electron beam systems. Both of us where zero everywhere. - Rapa for me has helped me loose weight. IE the theory of rapa helps lower the reset-weight as you loose. Your new “normal” drops with your actual weight lose. For me… I now weigh the same as I was in highschool. Another inch on my waist vs high school which means my muscle mass is lower. ;( Which is another reason why we follow the many Drs like Gabrielle Lyons saying eat a diet of 1.6g of protein per 2.2# body weight or for me 138 g protein which for hamburger is about 0.9 # per day. I can barely get that all down. High protein for minimizing sarcopenia, brain degredation… Rapa for simulating fasting etc. Just me, just my take on the big picture that we see. I read here many different views which is great.
summary (parroting 3 yrs of low carb/metabolic confs) higher LDL when calcium score is zero / low is good. This is all I have on this LDL topic.
We follow Attia and buy / read all his books. I agree hes not in the same camp as the keto/low carb Cardio Drs on stage at the confs re LDL and especially Apo-B. Our view: When your age is >>70 things turn (per just our views) that high LDL is an asset… Wishing all well, Curt

2 Likes