Probably dropping it from my stack too. Evidence of cardiovascular benefits is not sufficiently strong to outweigh even weak evidence of potential cognitive risks
3 Likes
That’s my thinking about a lot of drugs and supplements. So what that some drug is supposed to be protective against whatever, say, CVD - if I already take other stuff that’s protective and clinically shown to be safe, why add something that may come with risks or unknowns? Adding more is a “hat on a hat”. Not worth it. And if you keep adding, your stack will keep growing, increasing the odds of unforeseen negative interactions. Keep your stack to minimum of proven stuff where you’ve explored interactions. That’s why it takes me so long to add a drug to my stack - I scour the literature for interactions with the rest of my stack. Sometimes less is more. I’m a huge believer in polypharmacy, but also cognizant of the dangers.
5 Likes
There is like one study that it’s bad for Alzheimer’s and several that say it’s good. It probably just doesn’t have any effect at all for that. I think people need to relax before doing something silly and removing it from your stacks and thus increasing your risk of cardiovascular issues by doing so. If you can’t tolerate the sides, then I get it. But to worry it’ll give you dementia? Give me a break.
3 Likes
More than one study suggesting concern or lack of benefit in this thread re: Alzheimer’s and dementia:
Brennan & Tinworth (2025) - Molecular Neurobiology
Genetic data shows lifelong PDE5 inhibition increases the risk of Alzheimer’s and Lewy body dementia.[1]
• ETLAS-2 Trial (Olmestig et al., 2025) - Cereb Circ Cogn Behav
Three months of daily tadalafil yielded no cognitive benefit and resulted in slower reaction times.[2]
• Sanders Review (2020) - Journal of Alzheimer’s Disease Reports
High-dose PDE5 inhibition depletes cAMP, blocking amyloid clearance and promoting brain toxicity.[3]
Link: Sildenafil for the Treatment of Alzheimer’s Disease: A Systematic Review - PMC
There are also studies showing a cardiovascular benefit:
Wang et al. (2024) - Mendelian Randomization & Real-World Study
Genetic and real-world data show PDE5 inhibitors reduce the risk of coronary heart disease and MI.
• Soulaidopoulos et al. (2024) - Systematic Review and Meta-Analysis
A meta-analysis of 1.2 million patients found PDE5 inhibitors reduce MACE and overall mortality.
• Andersson et al. (2021) - Swedish Nationwide Registry
Nationwide data shows PDE5 inhibitors lower death, MI, and heart failure risks vs. alprostadil.
• Jehle et al. (2024) - The American Journal of Medicine
Analysis of 50 million men linked PDE5 inhibitors to lower risks of mortality, stroke, and MI.
Link: Benefits of Tadalafil and Sildenafil on Mortality, Cardiovascular Disease, and Dementia - PubMed
3 Likes
As is always the case with MR studies people should look at the choice of genetic mutation proxies.
Here they use 3, associated with systolic/diastolic blood pressure and PDE5A levels.
The first 2 are dubious to me but they think there is a relation with PDE5 even though it’s a proxy of proxy.
Here is what they get
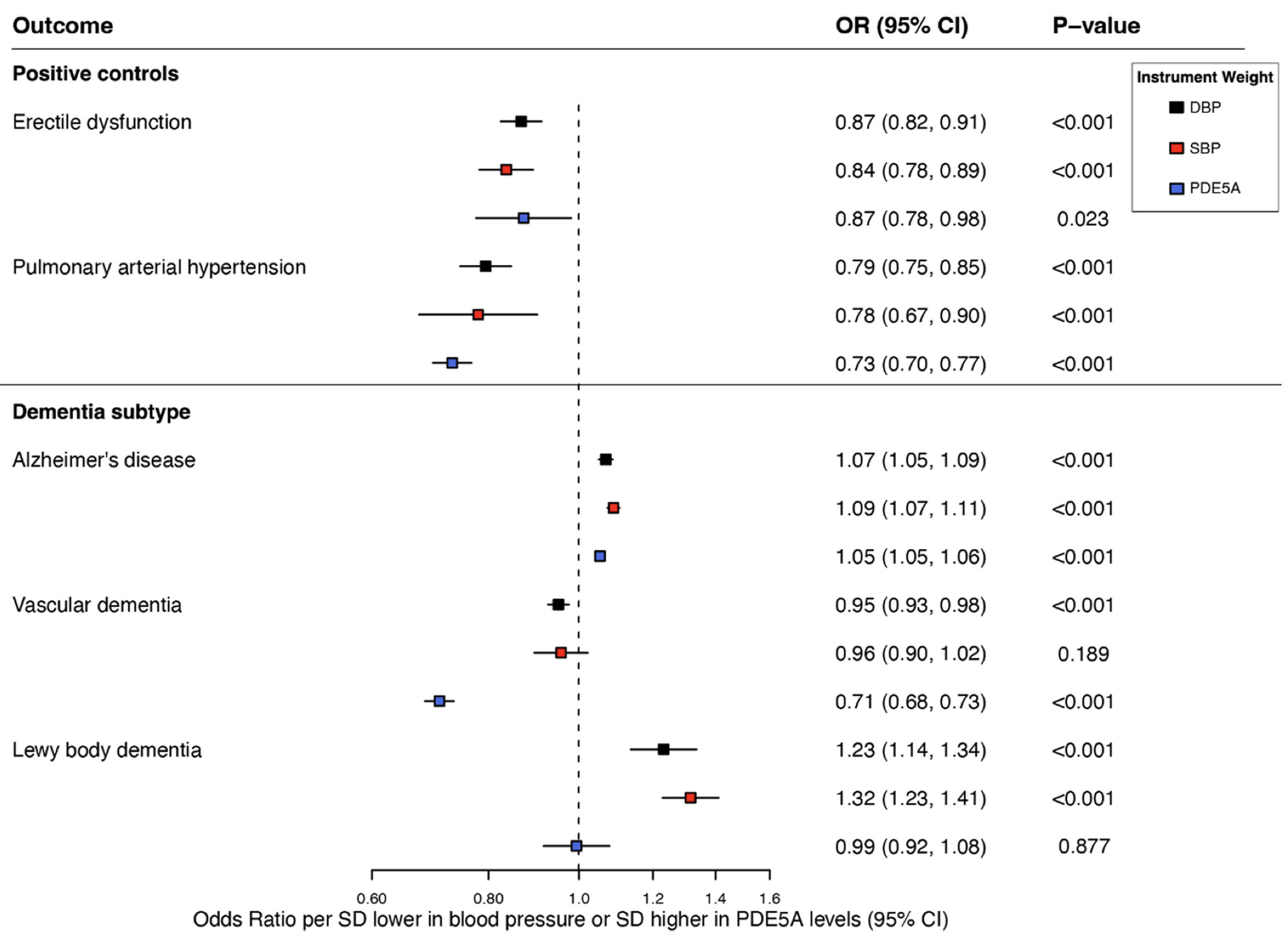
PDE5A levels have
- a lower OR (1.05) for Alzheimer than SBP and DBP.
- a much lower OR (0.71) for vascular dementia.
- No effect at all on Lewy body dementia.
BTW in 85 yo people who have dementia, there are more people with vascular dementia (46.9%) than Alzheimer (43.5%)
Looks more nuanced and positive for PDE5 inhibitors.
BTW a big problem with those MR studies is that the inhibition starts at birth and we know that a lot of longevity interventions are detrimental before middle age.
For instance mTOR inhibition at birth is obviously not good.
As my risk of vascular dementia and MACE is very high while my risk of Alzheimer is normal (APOE3/3), I’ll keep my tadalafil at 10mg/day.
7 Likes
Could you give me some examples? From what I understand, most anti-aging compounds need to be taken early in life; intervening in middle or old age can actually have the opposite effect.
That’s a very iffy statement. I’m not sure about “many”. If you are worried about mTOR and early development… maybe not? After all we have a similar situation with IGF-1 suppression or knockouts from birth, and in mice it results in dwarfism and an exceptionally long lifespan (there’s some equivocal results in Laron syndrome for people). Generally smaller members of the species tend to be more longevous (see: dogs). In fact delaying maturation in development is generally lifespan promoting, as sexual maturity pushes aging to a faster trajectory (see also pets and early neutering). CR started earlier, including before sexual maturity (in mice and rats) results in an even longer lifespan. I find it easy to imagine rapa administered starting very early in development on a cyclical basis, to allow some intermittent mTOR activation and suppression netting out to lifespan extension. Remember, dampening mTOR is not the same as elimination, because complete elimination is not a life extending intervention at any age. This is speculation of course, but I don’t think there’s a ton of life extension interventions that are deleterious at an earlier stage of development and should be strictly limited to application in old age. And I strongly doubt rapamycin is one (at least we need some proof, as it’s not self evident, I don’t think). YMMV.
1 Like
New video where Brad discusses Tadalafil towards the end (and encourages eating Arugula for NO)

I. Executive Summary
The reviewed transcript outlines the physiological imperative of mitigating the age-related decline of nitric oxide (NO), a critical signaling molecule for endothelial, cognitive, and musculoskeletal health. The central thesis critiques the commercial supplement industry for marketing ineffective or severely underdosed NO boosters. Specifically, the speaker dismantles the utility of L-arginine and L-citrulline supplements, noting their failure to produce reliable, clinically significant reductions in blood pressure or enhancements in athletic performance. Furthermore, the analysis challenges the clinical efficacy of commercial beetroot powders, citing independent testing that reveals sub-therapeutic nitrate levels in the vast majority of consumer products.
Instead of relying on exogenous supplementation, the transcript advocates for a whole-foods approach to exploit the enterosalivary nitrate-nitrite-NO pathway. While liquid beetroot juice is acknowledged as an effective, clinically validated intervention for hypertension, its high oxalate content poses a calculated risk for nephrolithiasis and inhibited nutrient absorption. The speaker’s primary actionable recommendation is the consumption of arugula (rocket), which possesses a superior nitrate density (~4,800 mg/kg) and a highly favorable low-oxalate profile, offering a zero-risk, high-yield dietary intervention.
Additionally, the transcript explores the pharmacological amplification of the NO pathway via tadalafil, a phosphodiesterase type 5 (PDE5) inhibitor. The speaker references recent large-scale observational data, including UK Biobank cohorts, that associate PDE5 inhibitors with substantial reductions in all-cause mortality, cardiovascular events, and dementia. However, the transcript accurately identifies a severe translational gap: the profound risk of healthy user bias. Because men prescribed tadalafil for erectile dysfunction often possess better baseline health and healthcare engagement, causality cannot be established. The analysis correctly concludes that until randomized controlled trials (RCTs) confirm preventative efficacy, off-label prescription of PDE5 inhibitors for longevity remains speculative. Ultimately, the optimal protocol prioritizes targeted dietary nitrate ingestion and exercise over predatory commercial supplements and premature pharmaceutical interventions.
II. Insight Bullets
- Nitric oxide (NO) is an unstable, short-lived gas essential for vasodilation; its age-related decline is a primary driver of cardiovascular and multi-systemic dysfunction.
- Direct ingestion of NO is impossible; therapeutic strategies must target endogenous production pathways or signal amplification.
- Prescription NO donors (e.g., nitroglycerin, isosorbide mononitrate) bypass natural production, rapidly inducing physiological tolerance and losing long-term efficacy.
- L-arginine supplements increase blood arginine levels but fail to reliably increase systemic NO due to extensive first-pass metabolism by hepatic arginases.
- L-citrulline acts as an arginine precursor and elevates blood arginine more effectively than direct L-arginine supplementation.
- Despite superior pharmacokinetics, L-citrulline yields clinically underwhelming results; meta-analyses show only marginal diastolic blood pressure reductions at high doses (≥6g/day).
- The enterosalivary pathway converts dietary inorganic nitrate (NO3-) to nitrite (NO2-) via facultative anaerobic bacteria on the tongue.
- Swallowed nitrite is further reduced to NO in the acidic gastric environment or via systemic nitrite reductases, entirely bypassing the eNOS pathway.
- Clinical trials demonstrate that ~400mg of dietary nitrate (via liquid beetroot juice) can reduce systolic blood pressure by approximately 8 mmHg in specific hypertensive populations.
- Independent product testing reveals that most commercial beetroot powder pills contain sub-therapeutic nitrate levels (as low as 4.3mg), far below the ~300mg active threshold required for physiological effect.
- Beets contain high levels of soluble oxalates, which can inhibit mineral bioavailability and precipitate calcium oxalate kidney stones in susceptible individuals.
- Arugula yields approximately 4,800 mg of nitrate per kg, offering a superior, low-oxalate alternative to beets for dietary NO enhancement.
- Tadalafil operates differently from nitrate donors by inhibiting the PDE5 enzyme, thereby preventing the degradation of cGMP and amplifying endogenous NO signaling.
- Recent observational data (including UK Biobank cohorts) associate PDE5 inhibitor use with a 28-34% reduction in all-cause mortality and significant drops in cardiovascular risk.
- Healthy user bias severely confounds observational PDE5 inhibitor data; treated cohorts often possess better baseline cardiovascular function and lifestyle habits than untreated counterparts.
- Current clinical guidelines do not endorse tadalafil for preventative cardiovascular care, highlighting a critical translational gap requiring Level B (RCT) evidence.
- Co-administration of PDE5 inhibitors and nitrate medications is strictly contraindicated due to the risk of profound, life-threatening hypotension.
III. Adversarial Claims & Evidence Table
| Claim from Video | Speaker’s Evidence | Scientific Reality (Current Data) | Evidence Grade | Verdict |
|---|---|---|---|---|
| L-citrulline slightly reduces blood pressure at doses ≥6g/day. | 2019 Meta-analysis. | Verified. A 2022 meta-analysis confirms marginally significant reduction in diastolic BP at doses ≥6g/day, but non-significant overall effects on systolic BP in middle-aged/elderly populations. | Level A | Plausible |
| Beetroot juice (~400mg nitrate) significantly reduces BP. | 2014 study on hypertensive patients. | Debated. While older studies show benefit, a recent 2024 RCT found that 4 weeks of beetroot juice affected nitrate metabolism but did not improve vascular function or BP in hypertensive older adults. | Level B | Speculative (Context/Population Dependent) |
| Most commercial beetroot powders lack sufficient nitrates (<300mg). | ConsumerLab testing. | Verified. Independent analytical studies show a 50-fold range in NO3- content among supplements; only 5 of 24 tested products contained the ≥5 mmol NO3- required for clinical effect. | Level C (Analytical) | Strong Support |
| Tadalafil use is associated with a 28-34% reduction in mortality. | Observational studies; 2024 UK Biobank study. | Verified observation, unverified causation. 2024 UK Biobank analyses note PDE5 inhibitors (like Sildenafil) are associated with increased lifespan, but explicitly warn of healthy user bias and the need for RCTs. | Level C | Plausible (High Confounding Risk) |
| Arugula is higher in nitrates and lower in oxalates than beets. | Unnamed data source. | Verified. Agricultural analyses confirm arugula contains up to 480 mg nitrate per 100g, far exceeding beets, with negligible bioavailable oxalates. | Level C (Analytical) | Strong Support |
IV. Actionable Protocol (Prioritized)
High Confidence Tier
- Dietary Nitrate via Arugula: Consume ~100g of fresh arugula daily to achieve the ~300-400mg therapeutic threshold of inorganic nitrate. This leverages the enterosalivary pathway without the oxalate burden of beets.
- Microbiome Preservation: Avoid the use of broad-spectrum antibacterial mouthwashes (e.g., chlorhexidine). These obliterate the oral facultative anaerobic bacteria required to convert dietary nitrate (NO3-) to nitrite (NO2-), effectively neutralizing the cardiovascular benefits of leafy greens.
- Exercise-Induced Shear Stress: Utilize zone 2 and high-intensity interval training to increase endothelial shear stress, the primary mechanical trigger for endogenous eNOS upregulation.
Experimental Tier
- L-Citrulline Supplementation: 6-8g of L-citrulline malate taken 60 minutes pre-exercise. While clinical outcomes for chronic blood pressure management are marginal, it is a safe precursor for acute endothelial support and carries a high safety margin.
- Standardized Liquid Beetroot Juice: For acute pre-training vasodilation, utilize liquid beetroot juice only if independent testing confirms ≥300mg (approx. 5 mmol) of nitrate per serving.
Red Flag Zone
- Commercial Nitric Oxide “Pills”: Avoid beetroot powder capsules and low-dose L-arginine supplements. The data strictly indicates these are sub-therapeutic and a waste of capital.
- Tadalafil for Primary Prevention: Do not initiate PDE5 inhibitors solely for longevity or cardiovascular prophylaxis outside of established clinical indications (e.g., ED, PAH). Safety data and RCTs for primary prevention are currently absent.
- Contraindication Warning: Never combine PDE5 inhibitors with exogenous nitrate donors (prescription or high-dose dietary) due to the risk of fatal hypotensive crisis.
V. Technical Mechanism Breakdown
The eNOS Pathway (Endogenous Synthesis)
Under normal physiological conditions, NO is synthesized in the endothelium by the enzyme endothelial nitric oxide synthase (eNOS). eNOS catalyzes the oxidation of the amino acid L-arginine to produce NO and L-citrulline. Oral L-arginine supplementation is highly inefficient due to rapid degradation by intestinal and hepatic arginases (the “first-pass” effect). L-citrulline bypasses this hepatic extraction, entering the systemic circulation where it is converted to L-arginine in the kidneys, making it a superior, albeit clinically modest, substrate donor.
The Enterosalivary Nitrate-Nitrite-NO Axis (Exogenous Synthesis)
Dietary inorganic nitrate (NO3-) from leafy greens (arugula) circumvents the eNOS pathway entirely. Upon ingestion, NO3- is rapidly absorbed in the upper gastrointestinal tract and actively concentrated in the salivary glands (up to 20-fold higher than plasma levels). It is secreted into the oral cavity where commensal facultative anaerobic bacteria reduce NO3- to nitrite (NO2-). Once swallowed, NO2- is further reduced to NO in the acidic lumen of the stomach, or absorbed into systemic circulation where it is reduced to NO by deoxyhemoglobin and other nitrite reductases, particularly under conditions of hypoxia or low pH.
The cGMP/PDE5 Axis (Signal Amplification)
Once NO is produced (via eNOS or the enterosalivary pathway), it diffuses into adjacent vascular smooth muscle cells and binds to the heme moiety of soluble guanylyl cyclase (sGC). This activates the conversion of guanosine triphosphate (GTP) into the second messenger cyclic guanosine monophosphate (cGMP). Elevated cGMP activates Protein Kinase G (PKG), which lowers intracellular calcium levels, resulting in smooth muscle relaxation and vasodilation. Phosphodiesterase type 5 (PDE5) is the primary enzyme that hydrolyzes and destroys cGMP. PDE5 inhibitors like tadalafil do not create NO; they competitively bind to PDE5, preventing the degradation of cGMP, thereby massively amplifying and prolonging the endogenous NO signal.
Oxalate Toxicity Profile
Beetroot contains high concentrations of soluble oxalates (ethanedioate). In the GI tract, oxalates chelate divalent cations (primarily calcium and magnesium), inhibiting their bioavailability. Systemic absorption of excess oxalate leads to renal excretion, where it can precipitate with urinary calcium to form insoluble calcium oxalate calculi (nephrolithiasis). Arugula provides the necessary NO3- substrate without this toxicological burden.
1 Like
I am struggling to understand why they have chosen SBP and DBP as proxies. PDE5A biology is much broader than BP regulation (cerebral blood flow, synaptic plasticity, neurovascular coupling,…) therefore it is very likely that these proxies are very? incomplete.
I think they showed in their model only that genetically lower blood pressure is associated with higher Alzheimer’s and Lewy body dementia risk. Whether this has anything to do with PDE5A inhibition is unclear.
2 Likes
I think you have to take the results in the larger context. If we assume the worst, and it’s a HR 1.07 for Alzheimers, that is a 7% added risk above a certain baseline. Even the worst finding from the Oxford MR study was Lewy body dementia with HR 1.32. If your individual baseline is pretty low, that 32% may still not be very significant.
You can also offset that potential risk against the proven benefits (pulmonary hypertension, benign prostate hypertrophy etc) and some plausible other benefits (UK biobank, all-cause mortality etc).
Lastly, to be honest, it’s one hell of a lifestyle drug. Even if you don’t have erectile dysfunction, they still improve the quality, consistency and “staying power”. Your partner will be pretty happy, and so will your ego. Plus, you get sick pumps in the gym which I personally find incredibly satisfying haha
6 Likes
This study has been peer-reviewed. It shows that genetically proxied PDE5 inhibition increases the relative risk of Alzheimer’s disease by 5% to 9%. Personally, I think this is an acceptable risk. What are your thoughts?
1 Like
I was interested in those drugs for neuroprotection. The evidence was already weak (mostly longitudinal studies with a lot of confounders) but with the MR showing increased risk of dementia: it’s a no for me. So I assume your question is: if you’re interested in those drugs for heart health, is the increased dementia risk worth it? I guess that’s a personal choice based on family history / genetics. If you have a family history of heart disease but no dementia then maybe. But even in that case, if your apoB + BP + glucose are already optimized and under control with lifestyle + drugs => can tadalafil really move the needle? By how much? If so is that worth the 5-9% dementia risk increase?
1 Like
Just reading the paper again: “Lewy body dementia (OR 1.32, 95% CI 1.23-1.41)”
I withdraw what I said above: sildenafil and tadalafil can go to the trash ![]() I don’t want LBD…
I don’t want LBD…
4 Likes
Did the paper show about same risk for Tadalafil as Sildenafil? The reason
I ask is because my side effects are night and day apart (for me) even though they are same category drugs. As an example, I get blurred vision, insomnia, and weak muscle aches with Cialis, and none with Viagra. With Viagra I only get a light flush and no other sides (btw, my doses are 6.6mg cialis, and 25mg viagra and haven’t tried other dosing).
IMO 5-9% risk is a lot. I usually have no problem experimenting with substances that have risk factor of ideally up to 1%, but at times up to 3%. Anything over 5% and I have to think more than twice before I try. Obviously, I’m talking about medium to severe side effects and not minor ones i.e. risk of dementia, risk of heart disease, diabetes etc and not a light headache as example…
3 Likes
sustained serum level as likely to yield highest benefit
DrFraser, I hope that is the case because it implies that tadalafil with it’s long half-life would be just as good as sildenafil with only one daily dose instead of sildenafil’s 20 mg TID. But, would a 5 mg daily dose of tadalafil be strong enough to match that 20 mg dose of sildenafil … I wonder?
I agree that these should be treated as unproven and potentially adverse until more evidence comes through.
But I may be more hopeful than others and less convinced by the MR studies.
The methodology seems flawed for IDing the PDe5 inhibition genes - all the MR studies use blood pressure variants near the PDE5A locus as instruments for “PDE5 inhibition.” . So they’re not really MR studies for PDE5 inhibition per se.
The major issue though is using circulating PDE5A protein levels to select. This from Claude:
“The Framingham observation — that higher plasma PDE5A predicts AD — is almost certainly a case of reactive upregulation: neurons and vascular smooth muscle cells under neurodegenerative stress upregulate PDE5A expression as a compensatory response to impaired cGMP signalling. The elevated protein is a biomarker of early disease, not a cause of it”
So by selecting using a marker neurodegentive stress - they probably completely invalidated the study.
This higIn this highly heterogeneous, retrospective observational study, among all PDE5 inhibitors, only sildenafil use was found to be weakly associated with a reduced risk of AD. However, this association did not reach statistical significance in men (HR: 0.58, 95% CI: 0.31–1.09) and was significant only in women.
1 Like
Well however small it is, at least it is a benefit LOL
But this drug comes with plenty of risks. For instance, someone just posted above about it increasing the risk of retinal detachment. If you don’t actually have ED, the payoff is just way too low to justify the risks.
2 Likes