Perfectly said. My thoughts exactly.
2 Likes
Just to be clear, there still haven’t been studies showing Taladalil does all these wonderful things as well, right? We are just speculating and hoping it does?
3 Likes
You’re right of course, we don’t know if it is interchangeable with sildenafil, but tadalafil is the choice of Matt Kaeberlein.
I started with sildenafil and then switched to tadalafil because it has a longer half-life and you only have to take it once daily. I have noticed no side effects so far. It possibly lowered my systolic BP by a couple of points. Both are amazingly cheap from India and I now have a lifetime supply of both. TMI: They both cause nighttime erections that are so hard I have difficulty peeing and I am forced to wait a while until the erection subsides before I can pee without a great deal of force.
Both are PDE5 inhibitors
“Sildenafil, on the other hand, is also a PDE5 inhibitor, but its chemical structure differs from tadalafil. Its chemical formula is C₂₂H₃₀N₆O₄S, and it belongs to the same class of drugs as tadalafil.”
C₂₂H₁₉N₃O₄ Tadafil
C₂₂H₃₀N₆O₄S Sildeniflil
12 Likes
I’ve been taking cialis most days for years, so it would suck if it turns out only Viagra had the benefits. My guess is Tadalafil also has the same benefits though. I’m hopeful.
4 Likes
Is there a Costco near you? The cost of generic viagra and cialis are very reasonable there.
1 Like
Conflicting evidence on PDE5i: No association between initiation of phosphodiesterase-5 inhibitors and risk of incident Alzheimer’s disease and related dementia: results from the Drug Repurposing for Effective Alzheimer’s Medicines study 2022
A recent Israeli study also found no protective effect for tadalafil vs alpha-blockers in BPH: Phosphodiesterase-5 Inhibitors and Dementia Risk: A Real-World Study 2024
The issue with PDE5 inhibitors is the lack of a good comparator and potential confounders (someone who gets prescribed viagra has a more active social and sexual life, which is associated with healthspan): Phosphodiesterase-5 Inhibitors and Dementia Risk: Confounding by Indication in Real-World Studies 2024
It might not be a class property but a specificity of sildenafil: Phosphodiesterase-5 inhibitors use and the risk of alzheimer’s disease: a systematic review and meta-analysis 2024: “Particularly, sildenafil usage showed a significant risk reduction (HR: 0.46, 95% CI: 0.31–0.70, p < 0.001), while findings for tadalafil and vardenafil were not significant.”
A recent study also found a protective effect (Phosphodiesterase Type 5 Inhibitors in Men With Erectile Dysfunction and the Risk of Alzheimer Disease: A Cohort Study 2024) but they note: “Last, because of the limitations of our database, we cannot rule out the effect of unmeasured confounding. We were unable to account for levels of physical and sexual activity, which may confer a level of benefit in AD risk and be predictive for PDE5I exposure.”
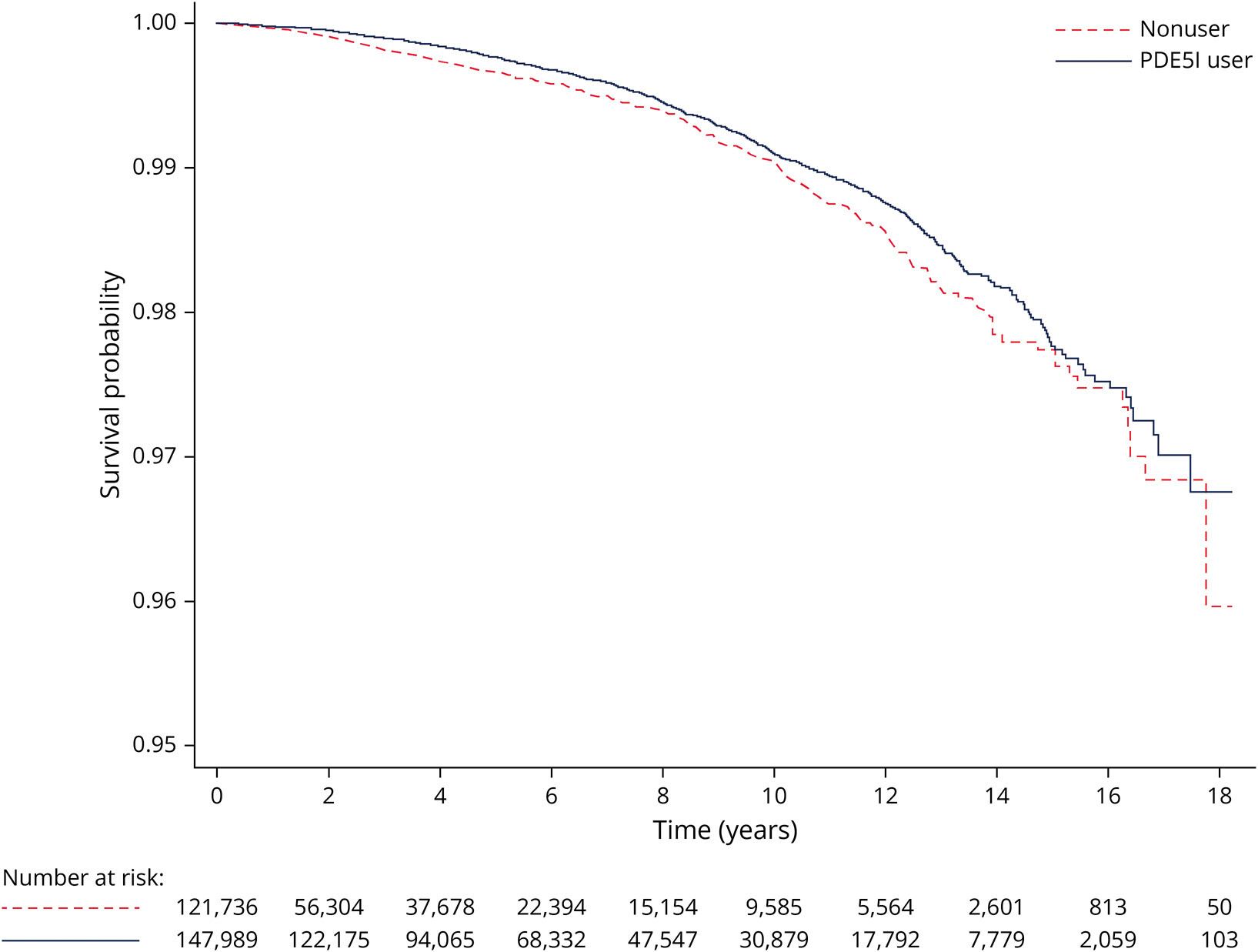
In this study, over 18 years (!), I would expect the difference between the two curves to become wider and wider, but it’s not the case:
Here, as well, the potential protective effect only applies to sildenafil:

As they note: “Evidence from pharmacokinetic studies have shown that the PDE5Is, sildenafil and tadalafil, both cross the blood–brain barrier, with sildenafil demonstrating greater permeability.”
(Of note, the ITP chose to test sildenafil and not tadalafil…)
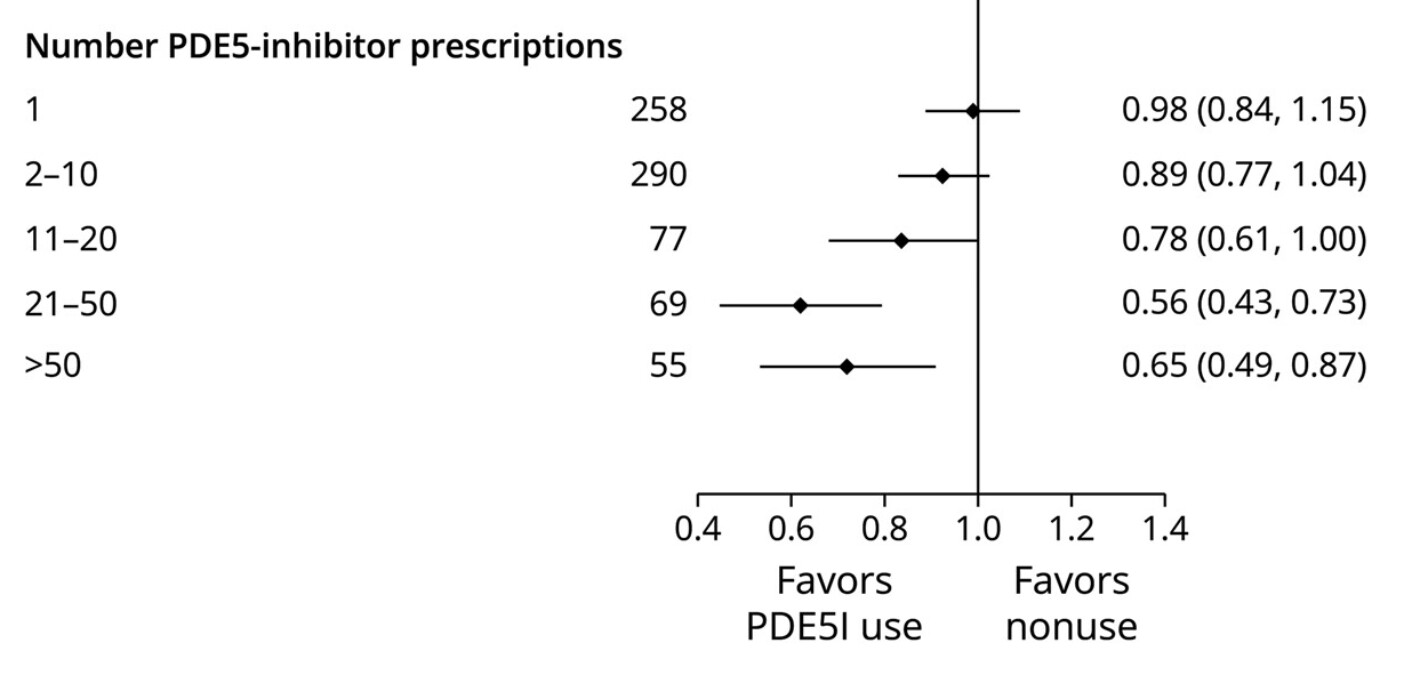
I would also expect regular users (>50) to have even less AD risk, but it doesn’t seem to be the case:
And surprisingly, it’s only protective in people >70yo?! If the protection was real, I would expect that the sooner you start, the better, right?:

They also don’t find any benefit “Among individuals without hypertension or diabetes”. ![]()
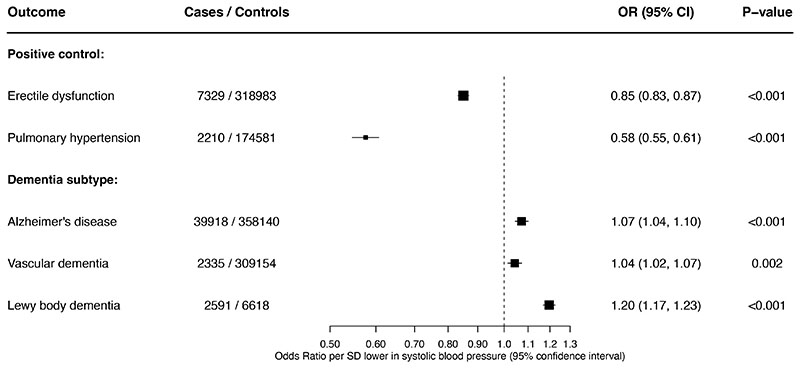
Then we have this Mendelian randomization preprint (![]() ) by a researcher from Oxford University: Genetically proxied PDE5 inhibition and risk of dementia: a drug target Mendelian randomisation study 2024
) by a researcher from Oxford University: Genetically proxied PDE5 inhibition and risk of dementia: a drug target Mendelian randomisation study 2024
In contrast to evidence from observational studies, our findings indicate that inhibition of PDE5 is associated with a higher risk of dementia and an unfavourable neurocognitive profile. This risk should be further investigated prior to clinical trials of pharmacological PDE5 inhibition for the treatment and prevention of dementia.
My conclusion from all the above:
- Tadalafil is not neuroprotective
- Sildenafil: still an open question, but probably not.
- If the MR preprint is correct, tadalafil and sildenafil might even be neurotoxic.
Thoughts @DrFraser?
16 Likes
That Mendelian randomization thing looks worrisome. Not conclusive, but IMO one needs to wait for a really convincing refutation of confounding before taking the other observational stuff seriously. Especially since we know that psychosocial factors are so predictive of longevity.
2 Likes
Wouldn’t you think that most observational studies would likely show poor results as those patients who need Viagra are likely higher risk for dementia?
These studies looked at patients diagnosed with ED or BPH.
First I don’t know whether ED or BPH are associated with a higher risk of dementia.
Second, if they have a higher risk that’s even better for association studies: you would be more likely to see the positive effect in a high risk population. In the same way that hypertension increases the risk of AD and PD but telmisartan users have half the rate of AD and PD vs non users. Same for diabetes and SGLT2i like dapagliflozin cutting the risk of AD and PD by two among this high risk population.
So absence of any protection in longitudinal studies + toxicity in MR preprint + the lack of protection in animal models = not neuroprotective and don’t use these drugs unless you have ED (and if you have BPH use terazosin or alfuzosin instead).
1 Like
There still seem to be cardiac benefits, for example comparing men who have ED, tadalafil (vs. none) led to much lower cardiac mortality. That review was published in Clinical Cardiology Feb 2024. There are multiple others. But this is depressing on the neurocognition component.
8 Likes
Do insurance plans generally cover tadalafil? I discovered my insurance doesn’t. Where do you buy it then? It seems to be quite cheap with a GoodRx coupon. Has anyone tried it? Is anyone taking it for neuroprotection purposes? If yes, at what dose and for how long? Is it helpful? Intuitively, it should be helpful as you have more blood flowing through your vessels.
2 Likes
So with a GoodRx or SingleCare coupon, 90 x 5 mg Tadalafil at CVS is $26.44. Surprisingly 90 x 20 mg is only $33.73.
The dose I’ve been Rx’ing is just 5 mg daily for vascular and until today for neurocognition - as I think this one is going to fall out as not effective - or at least, I don’t think I have enough evidence right now to make an assessment that this should be a core part of neurocognitive protection. @adssx has dashed my hopes that this was a likely beneficial drug in that area.
Some patients will choose the 20 mg and split the pills. The manufacturer says not to, but I’m not seeing a specific reason not to - unless someone knows a good reason on this one?
Pt’s with ED who don’t fully function without a bigger dose of tadalafil and add to the 5 mg dose, but max usually is 20 mg in 24 hours.
5 Likes
Instead of splitting the tadalafil 20mg pills, would taking the 20mg pills every three to four days, because of the relatively long half-life (17.5 hours), be a viable option?
The reason I ask is because I likely have a lifetime supply of the 20 mg tablets. ![]()
6 Likes
This is one of the more disappointing findings I’ve seen here. I thought Tadalafil was a lock to be great for a variety of reasons.
9 Likes
It looks to me as though the only concern on splitting them is that there may be unequal distribution of the drug through the tablet, and you could get a bit more or less than you think you are getting. I’d maybe look at breaking one in half and taking 10 mg every second day, would yield a much smoother level.
5 Likes
Is there any evidence that an equal distribution is required?
Or to put it another way: Is there any evidence that an unequal distribution would be less effective? We have evidence that drugs such as rapamycin are effective in unequal distributions.
That’s a fair question.
So side effects of any medication tend to be worse with higher dosing. Efficacy is worse with lower dosing (unless you believe in homeopathy then the reverse is true).
With doing 20 mg every 4 days, day 1 20 mg goes down to 10 mg effectively by 18 hours, then by 36 hours we are at 5 mg active, then at 54 hours down to 2.5 mg… etc.
So you will be getting a huge variation in side effects at the beginning (if any) but then efficacy loss later on.
There is obviously no outcome data, but we know different doses have different efficacy and side effects.
I tend to run all my long term medications in a way to keep a fairly
smooth level - but that is just me and how I was trained.
7 Likes
I don’t know if there is a proven association, but ED is often seen in patients with DM, CAD, PAD all of which I could see be a risk for dementia.
In association studies your comparing those on the drug for ED with those not on the drug because they don’t need it. So you may be comparing unhealthy with healthy. My guess is the unhealthy will have greater chance of dementia.
2 Likes
Before we only save our Cialis for “special occasions”, let’s not forget it appears to have good cardiovascular benefits
(Mouse study)
Tadalafil Prevents Acute Heart Failure with Reduced Ejection Fraction in Mice - PMC.
8 Likes