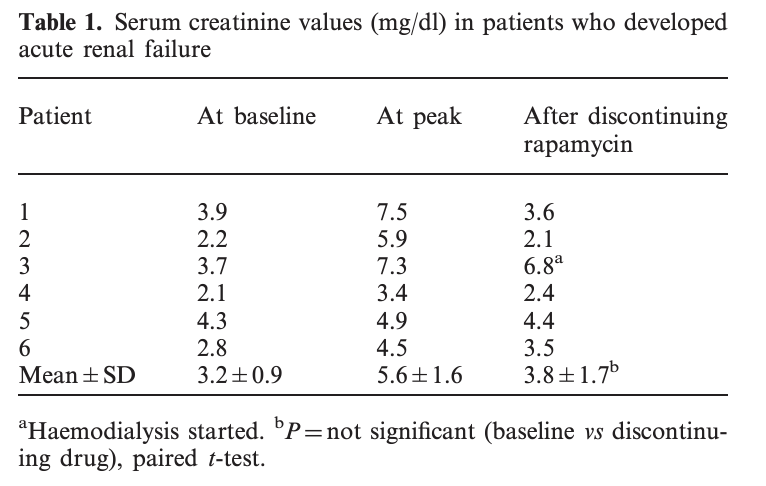
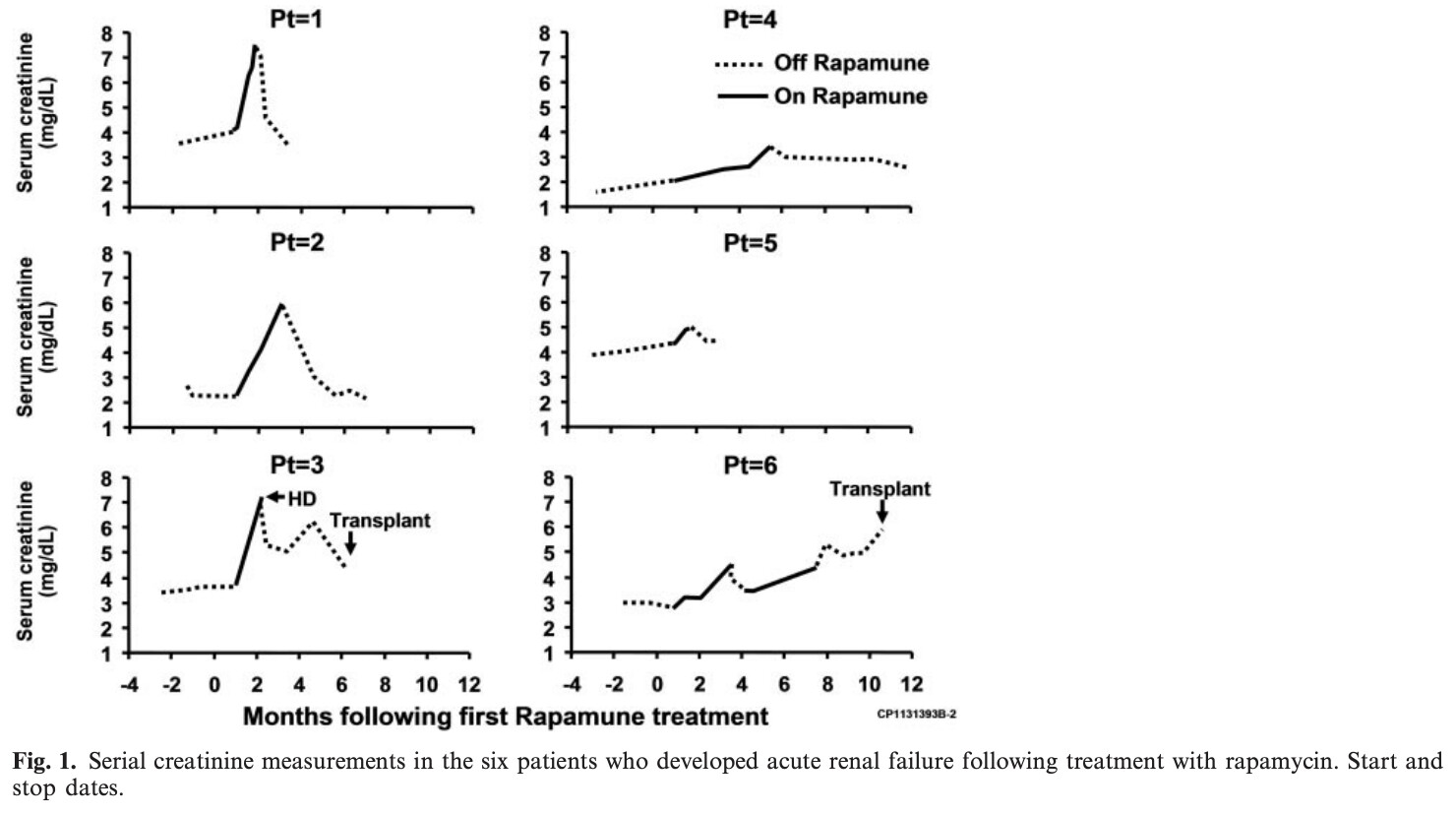
"In four patients, discontinuation of the drug resulted in improvement of renal
function close to baseline levels. One patient required
haemodialysis and had no subsequent recovery of renal
function. In another patient, renal function recovered
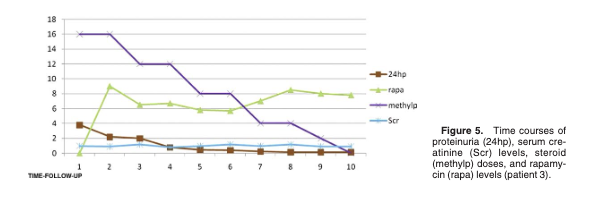
after discontinuation of the drug and then rapamycin
was resumed at a lower dose when creatinine returned
to baseline. This resulted in a second acute increase in
serum creatinine that failed to return to baseline when
the medication was discontinued. "
The study focuses on a specific population, but I’m curious about the risk for elderly people who may have undiagnosed mild chronic glomerulopathies.
Do you check kidney biomarkers (e.g., urine albumin-creatinine ratio, serum creatinine, or cystatin C)? Have you observed any changes?
Glomerulonephritis is one of at least 15 different types of kidney disease. My CKD has never been specified, but I think it resulted from an acute kidney injury, triggered by high BP. In any case, after more than a year of using rapamycin, I have detected no difference, good or bad, on my kidney function. I do a monthly check of creatinine, which continues to decline, along with a corresponding rise in GFR. These markers have been slowly improving for years. The gods have been good to me.
The study quoted has ZERO implications on otherwise healthy subjects based on the studies’ subject selection and rapamycin 35 mg/week high dosing… in other words its results are non-applicable to general population without renal disease and using much lower rapamycin doses.
I can tell you from my experience that any patient with CRF has to be very careful with any drug administration and dosing.
Yes, but the study mentions proteinuria as a key factor. Elderly people often have proteinuria, which can be a side effect of diabetes as I understand.
I have been taking moderately high doses of Rapamycin (10-14 mg eq.) on a weekly schedule for roughly 2 years and my creatinine and eGFR numbers are close to perfection. I have noticed only minor changes in my kidney function numbers which amount to statistical noise IMHO. N=1
TABLE 1: ADVERSE REACTIONS OCCURRING AT A FREQUENCY OF ≥20% IN AT LEAST ONE OF THE RAPAMUNE TREATMENT GROUPS IN A STUDY OF PROPHYLAXIS OF ORGAN REJECTION FOLLOWING RENAL TRANSPLANTATION (%) AT ≥ 12 MONTHS POST-TRANSPLANTATION (STUDY 2)*|Adverse Reaction|–––Rapamune Oral Solution–––||
|2 mg/day
(n = 218)|5 mg/day
(n = 208)|Placebo
(n = 124)|
|*
Patients received cyclosporine and corticosteroids.|
|Peripheral edema|54|58|48|
|Hypertriglyceridemia|45|57|23|
|Hypertension|45|49|48|
|Hypercholesterolemia|43|46|23| |Creatinine increased|39|40|38|
|Constipation|36|38|31|
|Abdominal pain|29|36|30|
|Diarrhea|25|35|27|
|Headache|34|34|31|
|Fever|23|34|35|
|Urinary tract infection|26|33|26|
|Anemia|23|33|21|
|Nausea|25|31|29|
|Arthralgia|25|31|18|
|Thrombocytopenia|14|30|9|
|Pain|33|29|25|
|Acne|22|22|19|
|Rash|10|20|6|
|Edema|20|18|15|
Pregnancy may pose a risk of CKD progression for people with established CKD. In addition, some recommended medications to slow or prevent CKD progression are teratogenic (such as ACEi/ARBs or mammalian target of rapamycin inhibitors) and discontinuation during pregnancy should be considered.
I wonder if this is a typo because rapa isn’t mentioned anywhere else in the report and I don’t think mTOR inhibitors are “recommended medications to slow or prevent CKD progression”.
Rapamycin, an mTOR inhibitor, does not have a direct, consistent effect on albumin levels in the blood. However, its impact can vary depending on the context:
In Kidney Transplant Patients: Rapamycin has been associated with lower serum albumin levels in some studies, possibly due to its effects on protein metabolism or inflammation.
In Cancer Therapy: When used as part of nanoparticle albumin-bound formulations (e.g., nab-rapamycin), it does not appear to significantly alter albumin levels
General Use: Rapamycin’s effects on albumin are not well-documented in healthy individuals, and any changes are likely to be secondary to its broader effects on metabolism and immune function.
This sounds like typical AI waffle word games to me.
Circulating albumin is a very crude measurement in general. It’s affected by liver output, kidney filtration, tissue fluid and edema, and it’s a general marker of inflammation.
The best data I am aware of, the PEARL trial, showed no changes in albumin in those healthy subjects.
I can talk only about personal experience with taking Rapa for 15 years after kidney transplant. AI gave pretty accurate info about decreased albumin in transplant patients associated with Rapa. Mine is always on a lower side and I have to try hard to keep it within norm.