My cystatin C Journey
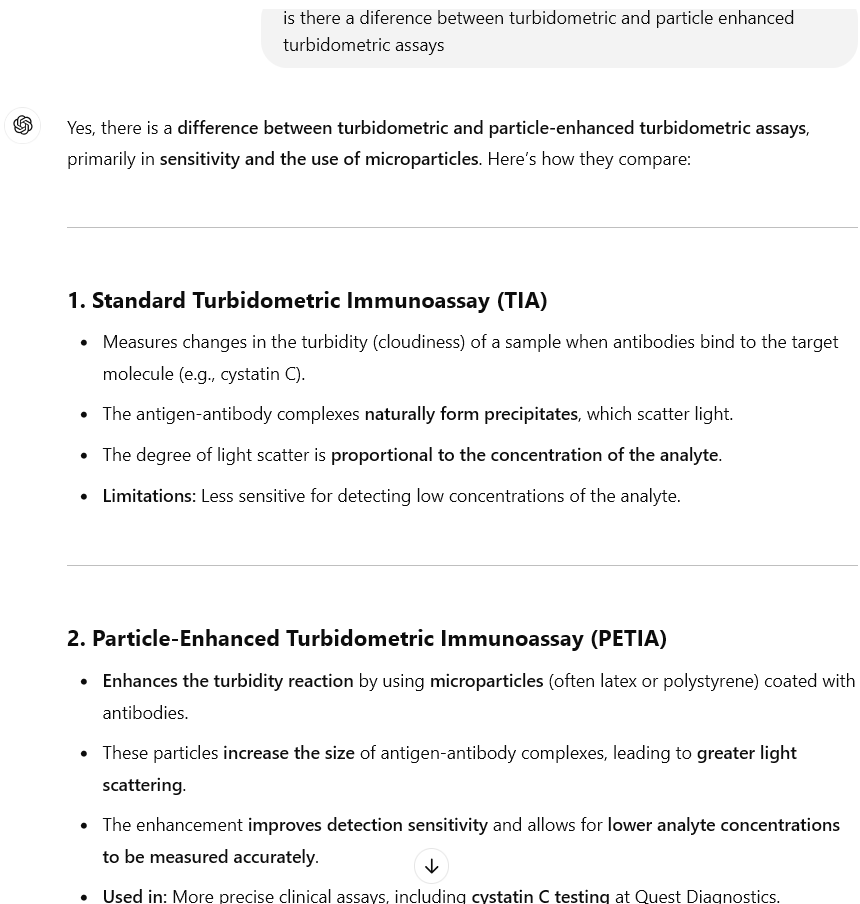
In June of 2023, and January 2024, I did two tests at LabCorp. The results that came back looked quite good, especially since ceatinine-based EGFR showed 25-30 units less.
I tested again last September, and the results showed a seemingly significant 8-9 point decline.
Not thrilled paying $80+ a pop, but then somebody pointed out you can get $40 (really $60) tests done via Jason Health and Quest, who can pass up such a bargain, so I got another at the end of December.
The EGFR result came back 12 points lower than September. I’d lost about 20 points in a year and a half.
WTAF. Yet one more time, stop most all meds and see if that arrests the decline.
I did three more tests (at least I found a way to get them done at $25 per), two weeks apart, all at LabCorp. Egfrs from those three: 72, then 82, then 102. Apparently my kidney function returned to the status of an eighteen-year-old’s, just by stopping meds.
One odd thing about that last (102) EGFR. Whereas all the preceding tests had been sent to a lab in North Carolina for processing, this one was processed here in San Diego. A new capability apparently.
Just for s&g, tested again, two days after the 102, at Quest. Came back 27 points lower.
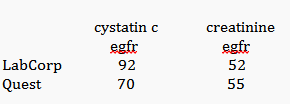
All summed up below.
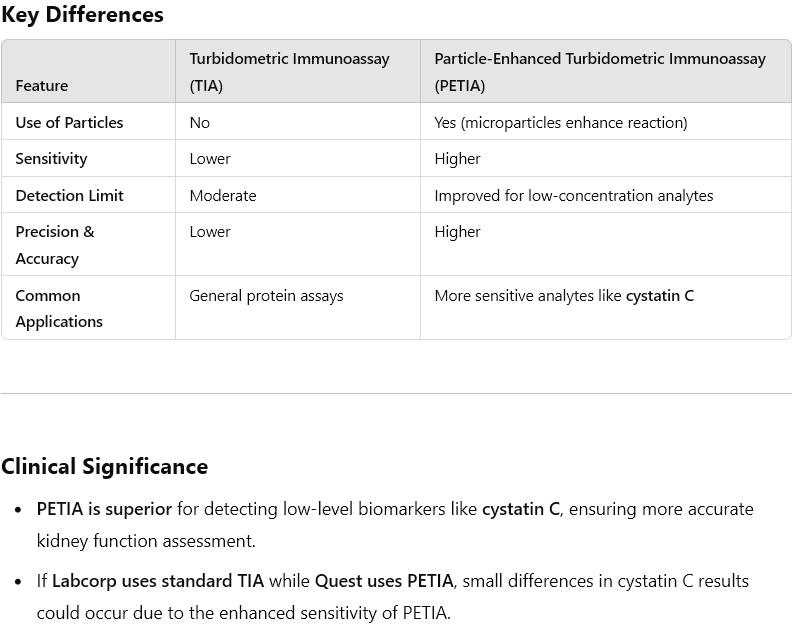
How do the LabCorp and Quest methodologies differ?
LabCorp’s test description says it uses a turbidometric assay, Quest says it uses a ‘particle-enhanced’ TIA.
Maybe the above explains why the Quest results are ‘somewhat’ lower than LabCorp’s. Nothing explains the 102 reading except some malfunction.
Next time I test, I will do cysC at a colocated site, with both blood draws occurring within about an hour. I have read that cysC is affected by hydration status (as is creatinine) so will make sure to be well-hydrated.