In the Rapamycin Longevity Series I interview the world’s leading Rapamycin and mTOR researcher Joan Mannick. She is currently CEO at Tornado Therapeutics where their goal is to develop the next generation of mTOR inhibitors which is better than Rapamycin. Without her research and passion in the Rapamycin field we would not be where we are today.
These are the three key takeaways I take with me.
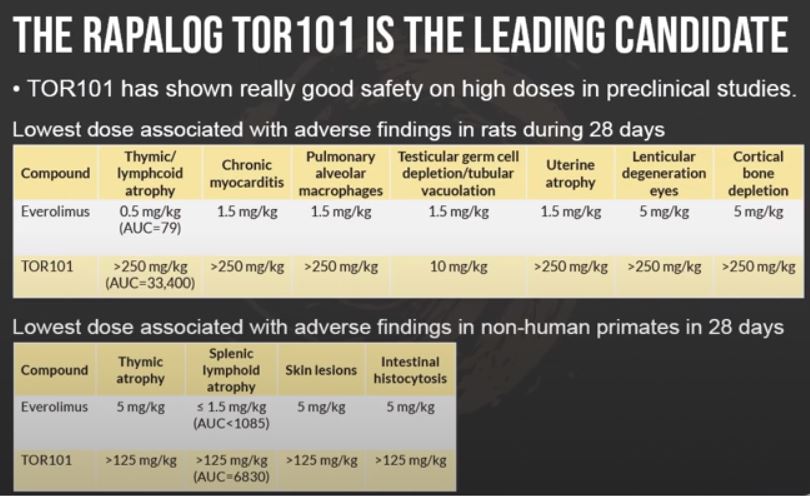
The data around turning down mTOR to younger levels looks very interesting when it comes to improving the aged immune system. So I feel quite confident after this interview that we probably around 2030 will have an mTOR inhibitor that is approved for improving the immune system in elderly. The leading mTOR inhibitor TOR101 which Joan is currently working on seems also very unique in its safety profile when it comes to very high doses. This opens up many other interesting areas to look at also.
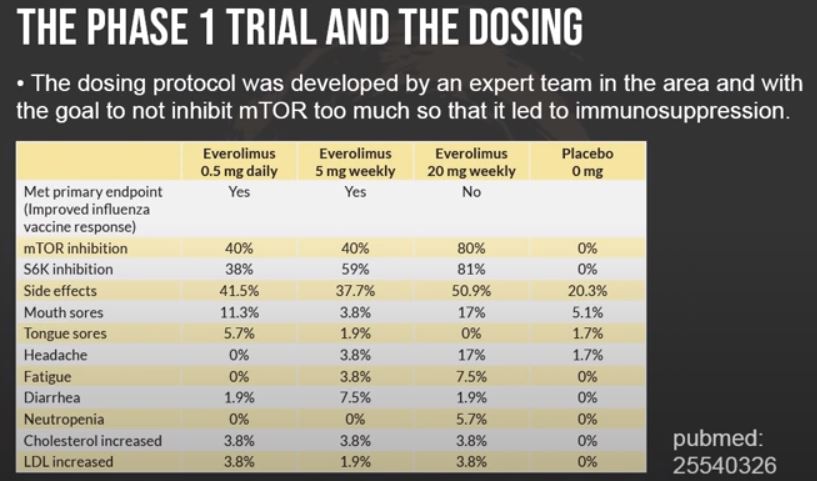
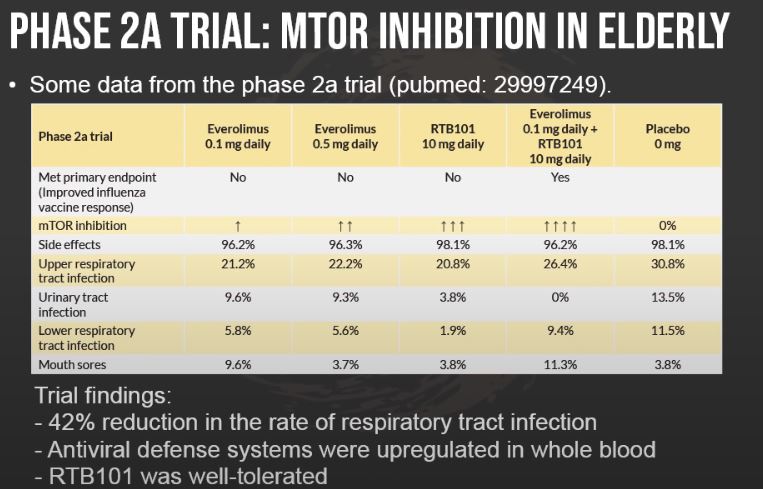
One other very interesting thing that she lifted up in the podcast was about the mTOR inhibition levels of different doses of the rapalog Everolimus. In the phase 1 trial the doses 0.5 mg/daily and 5 mg/weekly inhibited mTOR around 40% and these two doses had the best effect. The dose 20 mg/weekly which inhibited mTOR around 80% had a too high mTOR inhibition. I think it was also very interesting to hear her view on how to potentially detect early signs of too much mTOR inhibition. One thing is to look at if lipids and glucose levels in the blood start to increase. This may be an indication of mTORC2 inhibition.
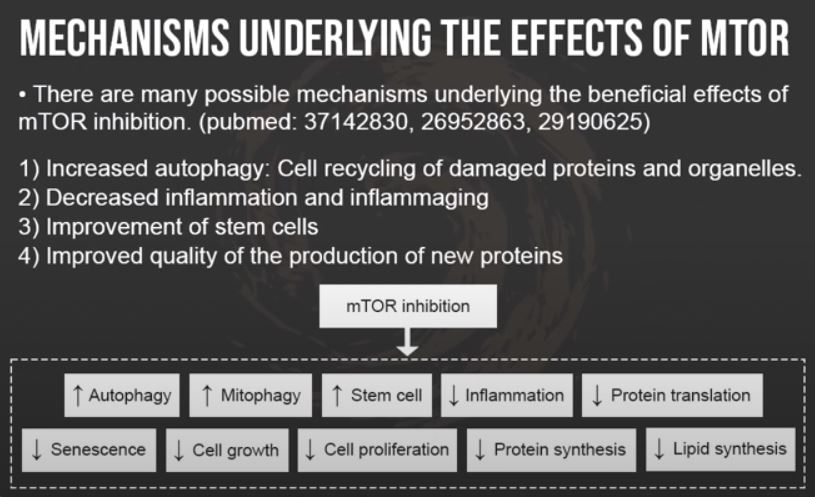
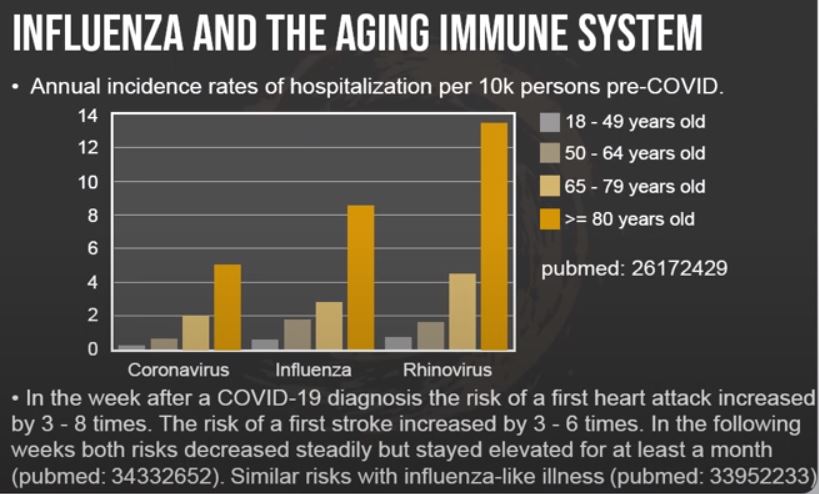
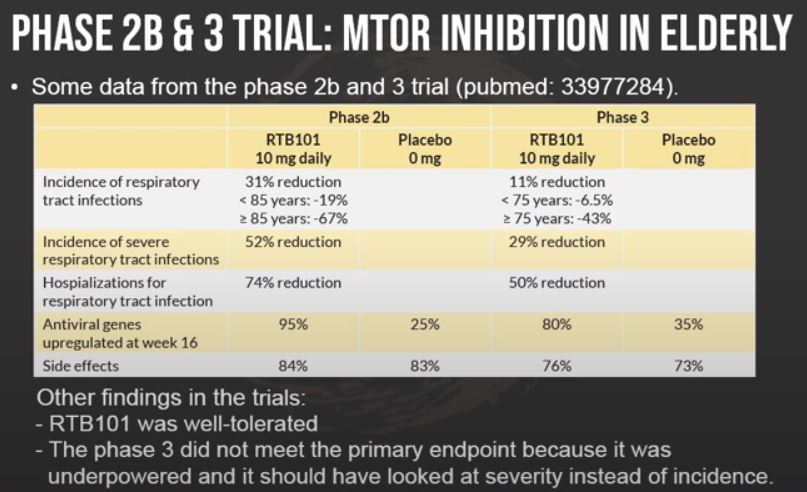
It was interesting when Joan looked at what genes were upregulated when elderly took a mTOR inhibitor. It was not things like a big increase in autophagy or improved mitochondrial function. The biggest effect was seen in upregulation of different antiviral genes. This reminds me also of Laura Niedenhofers very interesting research where she has found that an aged immune system may drive aging and senescence (pubmed: 33981041). This makes me start to wonder if one reason why mTOR inhibitors work so well in multiple species is because it keeps the immune system in a more healthy state.
Timestamps from the episode
01:59 Longevity interest and research 03:40 How Joan’s longevity career started 06:24 What is mTOR and what makes it unique 08:55 Mechanisms underlying the effects of mTOR 10:56 How translatable is the effects of mTOR to humans 12:43 mTOR inhibition and it’s upstream pathways 14:02 What is Rapamycin and how it was discovered 15:21 The weak points of Rapamycin 16:35 mTOR contains of mTORC1 and mTORC2 17:28 What is a rapalog 18:31 Detect early signs of mTORC2 inhibition 19:40 Tornado Therapeutics and it’s portfolio of rapalogs 23:13 Joan proposed a courage trial to the board 27:07 Animal data show Rapamycin may improve the immune system 28:09 Designing the dosing protocol for phase 1 trial 29:26 The phase 1 trial and it’s results 32:50 Aged immune system may drive aging 35:12 A good immune system may prevent cancer 36:05 Influenza and the aging immune system 38:29 The phase 2a trial and mTOR inhibition in elderly 39:32 The phase 2b and 3 trial 40:28 Antiviral genes are upregulated 42:26 Catalytic mTOR inhibitor RTB101 43:05 The phase 3 trial did not meet the primary endpoint 46:02 Pilot trial to decrease the severity 46:59 Dose protocol of Everolimus and RTB101 49:37 Safety profile between Everolimus and RTB101 52:10 Vaccines and/or mTOR inhibitor 54:51 Dosing protocol to improve the antiviral response 56:44 Taking a break or continue taking mTOR inhibitor during a common cold 57:49 Immune system biomarkers 59:24 Sarcopenia and mTOR inhibition 1:01:50 Leading candidate in Tornado Therapeutics portfolio 1:03:19 Safety profile of the rapalog TOR101 1:06:13 Next step for TOR101 1:08:25 Rhinovirus trial with TOR101 1:08:56 When will a mTOR inhibitor be FDA approved for longevity 1:10:28 Lifespan studies with TOR101 1:11:49 Joan’s own personal approach to mTOR inhibitors 1:13:33 Most promising longevity interventions 1:15:30 Autophagy and mTOR inhibitors 1:16:40 Big challenges in the longevity field 1:19:20 What the field really needs 1:20:48 Contact information
With the caveat that I do my best to never try and guess the motivation of someone, and take them at face value - I do think think that someone like her is in a difficult position with that question.
It would be difficult for her to say “no comment” (though personally, I think that would be perfectly acceptable). In a way we would assume a “no comment” answer means she’s taking it.
If she says “yes”, then it would be easy to see that as a tacit endorsement. She could use all the disclaimers she wants, but the fact that she takes it would help sway people to take this drug, on the margin and a reasonable person could feel uncomfortable influencing people to take this kind of off-label treatment. She is obviously highly credible and has a high level of “authority” with regards to this drug.
I have an old Land Rover, which I love. When people ask me if they should get one, I don’t hesitate to say “no”. The car is a PITA, but I don’t care because I like it. The person who buys one will buy one anyway, even thought I’ve told him not to. That’s the kind of person who should own one.
And maybe that’s the kind of person who should be experimenting with this drug. Someone who understands the risks and potential benefits (to the extent we know them), without an endorsement from her.
I agree with you. She does have level of credibility to uphold higher than the average. I have seen some of the experts change their messaging from feeling it is not worth the risk based on current data to they have personally reconsidered, but do not feel the masses should follow. She did an excellent job in providing a counter point to someone at a conference in Saudi on why Rapamcyin shows a lot of hope. Personally, I would feel better if someone of her stature said they are taking due to her expertise:).
I recall listening to an interview with Matt Kaeberlein where he said he wasn’t taking it…though he does talk about isolated event where he was having trouble with his shoulder which was inhibiting him going to to throw the ball around with his son and he did take rapamycin/sirolimus for a period and it was helpful.
In a later interview, I think he said that he does take it, but don’t hold me to that (I don’t recall the exact interview).
I did t listen to the interview, but read Krister’s summary and slides. Did Joan Mannick discuss Rapamycin dosing? I saw the dosing for Everolimus, but not Rapamycin.
@David & @egec She is not taking any mTOR inhibitor yet but she is open to take it when more data comes. In this time clip you can find a summary of what she want to see before she starts taking it.
Regarding Matt Kaeberlein he is not taking Rapamycin yet again but he will take it again. In this time clip he shares why.
Are we sure that is correct? From an order of magnitude (log type of level) perhaps, but I thought Peter Attia spoke with one of the top scientists and they said it was like 60% or something.
Haven’t read it carefully, but this new paper may suggest ~50%?
For anyone considering Evero or switching from Rapa or basing your Rapa from scratch off of the Evero clinical trials I think you may want to look into the ratios a bit more.
The C/d ratio of sirolimus was 4.42, whereas the everolimus ratio was 2.23, resulting in a sirolimus: everolimus ratio of 1.98. Secondarily, after converting between mTORi, 93% of patients who reported intolerance(s) to one agent had a resolution of that intolerance. In our patient population, everolimus appeared better tolerated than sirolimus, with significantly more patients having no reported intolerances and significantly fewer patients experiencing edema. Other lab values were similar between patients receiving sirolimus and everolimus, except for an increased hemoglobin level in those receiving everolimus.
Conclusions:
The conversion ratio of 1:2 observed in our population suggests OHT recipients may require an increased dose of EVL compared with SRL to maintain the same goal trough levels. A conversion between mTORi appeared to improve tolerability and did not lead to clinically significant worsening of any measured lab value.
I think you’d want to assume “similar” or 2x and test your blood levels if you were going to switch. Dose is close but as we’ve seen with sirolimus it is pretty individually dependent. I wonder if one can test everolimus levels at Lab Corp like sirolimus? Since it is likely liquid chromatography tandem mass spec it should be an easy switch if they are willing to read it out. . Probably not nearly as common of a test though.
Great podcast/interview, thanks so much.
I have a question regarding her statement re lipids/triglycerides. She said or implied that a useful way to determine the best dose for an individual is to monitor lipids and if they increase the dose is too high.
Since finding the ‘right’ dose is sort of the holy grail, this is huge information but I have not heard it presented this way before. Yes, well aware of the potential risk of rapa increasing lipids but not heard that this may be a/the way to guide dosing.
Have others heard this? Thoughts?
Second question: what exactly is the goal of levels? If taking 6mg q wk what is being looked for in a trough level, what is its clinical value. I understand the importance of levels in transplant pts but how would they be used with low dose use?
Note sure how much I buy that. Perhaps looks at the different ITP success stories and see if lipids/triglycerides and did she also say glucose (?) went up in the mice even when they had good longevity benefits? You can also compare between the lower dose rapa successes and the higher dose successes.
Thanks for the clarification! From previous comments she seems to be more interested in a short acting rapalog that can mimic mTOR inhibition similar to when we are younger and it naturally mTOR is turned off when we are fasting during sleep. Everolimus better? Dosing before bed to achieve peak levels while asleep / fasting?
Neo, the steak basically is to repair muscles with high protein after my workout. I do workout and steak every other day. At my age I feel there is a need for recovery and actually working out every day might be bad for me. I see no issue with muscle loss or anything by just working out every other day. Which has been my schedule for about six years now.
So I generally workout from about 6 pm until 7:30 pm at night. Then, at home, I grill a steak around 9pm. I don’t do my rapamycin until probably about 11 pm or midnight.
I figured by then most of the steak protein benefit… has happened, and shouldn’t be as effective on the rapamycin. I go lighter on protein the next day.
Yes I think @Krister_Kauppi is correct here. Everolimus is basically same molecule as rapamycin, this is discussed in Peter Attia podscast #272 between David Sabatini and Matt Kaeberlein. And they both consider conversion 1:1 as mTOR inhibitor.
I agree that they seem similar from their mechanistic effects. But I’m not convinced of that simple 1:1 conversion ratio - and would look into it more if I was basing decision off of the conversation factor.
Here is another paper
mTOR Inhibitors Everolimus and Sirolimus Are Not Peas From a Pod
The half-life of sirolimus (60 h) is approximately twice that of everolimus (28 h). In addition, everolimus is both more soluble and bioavailable and has a 2.1-fold weaker binding affinity for FKBP12 than sirolimus
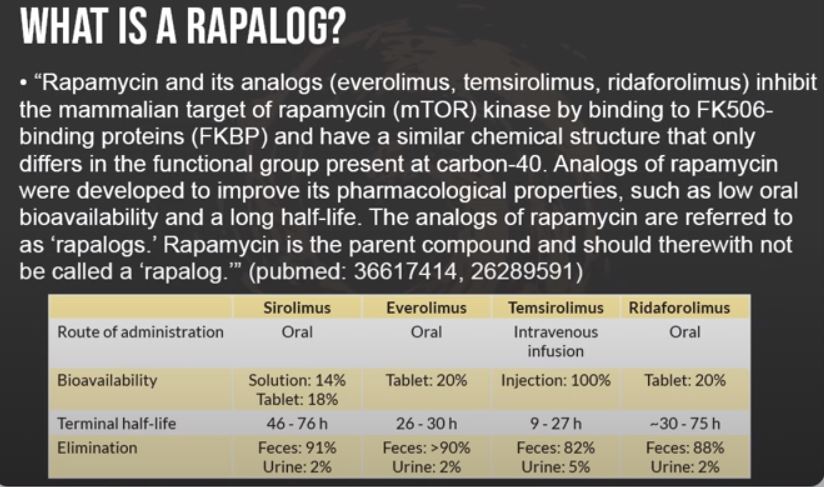
Rapamycin inhibits the mTOR kinase by binding to FK506-binding proteins (FKBP), and its analogs have a similar chemical structure that only differs in the functional group present at carbon-40 (shown in Fig. 1) [10]. Rapamycin’s analogs such as everolimus, temsirolimus, and ridaforolimus are therefore direct analogs. They were developed to improve the pharmacological properties of rapamycin; low oral bioavailability (tablet: 14%, solution: 18%) and a long half-life (46–78 h) [11‒13]. Everolimus has higher bioavailability (tablet: 20%) and a shorter half-life (15–35 h) than rapamycin [12, 14]. Ridaforolimus has a higher bioavailability (tablet: 20%) [15, 16]. Temsirolimus is a derivative of everolimus formulated for weekly intravenous administration and, therewith, has 100% bioavailability [17].