Yes, I’ve thought that might be the case as well. My current approach is to keep my estradiol at a level just above the menopausal range (I’m a bit stumped on how how to phrase this politely) so I’m able to function adequately in my marriage which is to a slightly younger man. To my knowledge I don’t need high levels of reproductive hormones for anything.
2 Likes
A couple of quick things on HRT - taken topically using FDA approved patches - monitoring levels is not needed - monitor by symptoms, so long as in the 0.025 to 0.1 mg/day range (most end up ~0.05). Make sure to be on micronized progesterone at night irrespective of whether one has a uterus as it is a great GABA agonist and normalizes sleep for most.
Do not use oral estrogens - topical only.
+/- add 10% of a male dose of testosterone.
That is a quick primer to my approach in this area - naturally lots of nuances, indications, contraindications … etc.
Labs of hormone levels aren’t needed UNLESS there are problems that aren’t obviously in need of fixing (exception would be if on testosterone I’d check occasionally). There reason is that we know the dose that is safe and effective with these preparations, and simply talking with the person generally lets us know if we are on a decent dose for them in regards to estradiol (skin, hair, sense of well being, for example) and progesterone (sleep quality, among others)
5 Likes
Thank you sir! By some stroke of dumb luck or divine intervention this is my exact hormone regimen! Your input is always greatly appreciated and valued.
1 Like
Thank you for the information, may ask what is the reason for not using oral estrogen? Apologies if I missed something.
1 Like
Absolutely good question. Oral estrogens undergo first pass metabolism inducing clotting factors in the liver. Thus increased thrombosis (PE/DVT) and stroke. We should be using bioidentical on the estrogens now, so Estradiol - but I still see some physicians prescribing it orally - and they are increasing their patient’s risk of these complications for no conceivable reason when patches are available and eliminate this risk.
I also have patients come to me who have had prior DVT or PE and their doctor tells them they can’t have estrogens. This is incorrect - there is no increased risk of these issues with topical estradiol.
Hopefully that answers this one - let me know if any other questions.
2 Likes
Yes, that explains it. And is it normal to start the patches when you are still getting period @50 years range of 21- 60 days. Or just wait and see whether Rapa helps with them continuing.
1 Like
What you said!!!
I had a clot once many years ago and recently asked about oral estradiol vs the gel I’m using, and the doc said not with your history.
1 Like
Peri-menopause is a complicated time on how to best manage the transition. There is some testing an planning needed. In general, we don’t want you having years of chaos with the transition, but need to sort out some stepwise sensible interventions to smooth the up and down of this time.
Seeing an expert is usually helpful in getting a plan together.
If one is of the understanding that optimizing hormones for life is probably the best approach for longevity - letting years of up and down happen along with metabolic and mental health effects may not be the best plan.
There is a risk/benefit with every intervention - or lack thereof.
Most of the time, individualized approaches are best, as one size doesn’t fit all.
2 Likes
TMI ALERT:
Well, once again, it’s either cancer, or I’m a genetic freak, or rapamycin delays menopause.
That is all. Carry on….
3 Likes
Puberty, menopause and aging are AFAICS part of development. You can slow them down and speed them up.
1 Like
We’re all about TMI here, the more information the better. Its anonymous sharing, so don’t be shy. We’re a medically-oriented site, so we go into more detail than the typical “consumer” site.
3 Likes
I’m dying over the graphic you used in that link ![]() !!!
!!!
Yes, after that link, breaking news about my cycle seems like a big yawn.
1 Like
Its in men’s interest to understand more about menopause as it is part of development and aging.
1 Like
Would you mind sharing more details? My wife and I are interested in knowing how long your cycle has been done, how long you’ve been taking rapamycin, what dose, how often?
Edit: I apologize. I reread your comment and realized that what you are saying is that you still have your monthly cycle, not that you regained it. Is that correct? Thanks!
1 Like
Freeze embryos instead and select them using genetic screening choosing which polygenic and monogenic traits you want to increase or decrease. Can become pregnant post menopause.
1 Like
Hmmm… cost of rapamycin at 5mg/week is about $20/month for 5 years (say); total cost = $1200
vs. cost of embryo freezing…
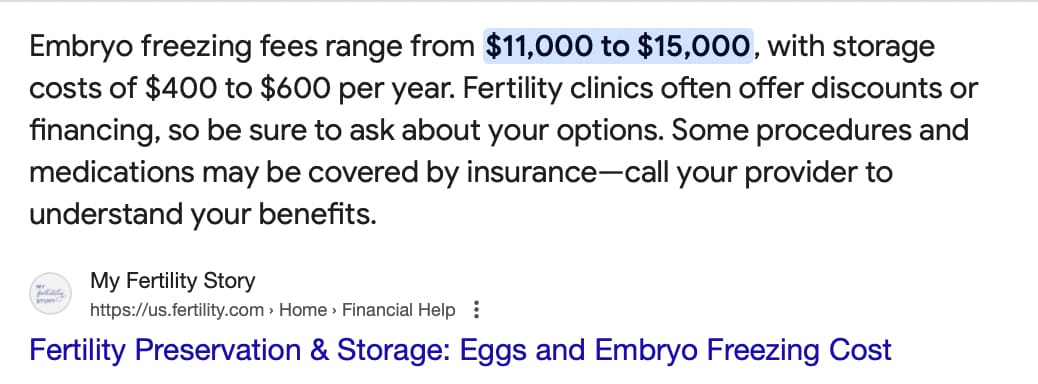
Isn’t having children already expensive?
You didn’t add the genetic screening, if you add the benefits from that it’s many orders of magnitude greater $$$ compared to rapa if you like to think that way.
The difference in income from lower risk for different diseases & higher intelligence or educational attainment.
I’m happy to share. And you were right the first time, it came back, sort of.
I had been late to enter menopause, but I had not been regular for a year or two prior. According to Oura, my last cycle had been 6/18/23. I was 57 at the time.
Then, as I posted on 6/1/24, at 58, I got my cycle again. Menopause is after you don’t have a cycle for 12 months, so I had officially been in menopause for a week. It was not a full cycle and then only a little bit less the next month, and then nothing at all happened again. I will note that my cycle had never been more than 3-4 days.
I did have a pelvic ultrasound to rule out anything scary.
Then, as you saw, I got it again the other day.
My history with rapa.
4/6/24 1mg first dose
4/27/24 3mg second dose
5/4/24 6mg third dose.
I then continued with 6mg weekly.
I took Sept off only because I had a rash and wasn’t sure if it was from the rapa.
Then, I continued on 6mg weekly
I’m normally between 104lbs-108lbs.
There is still a chance this was all going to happen without rapa, but at my old age, I imagine that is quite rare? Rapa has made a tremendous difference in how I feel, so I would not be surprised if it was causal.
1 Like
All extremely hypothetical for the foreseeable future… and do you have any idea of the pain and discomfort that women have to go through for egg or embryo harvesting (the regular shots, etc.)…
I would argue that the cost/benefit for rapamycin is much, much higher than for IVF or embryo implantation.
All the cost you’ve mentioned is for the hypothetical ability to have children. The actual success rates for IVF or frozen embryos is much lower than most people realize:
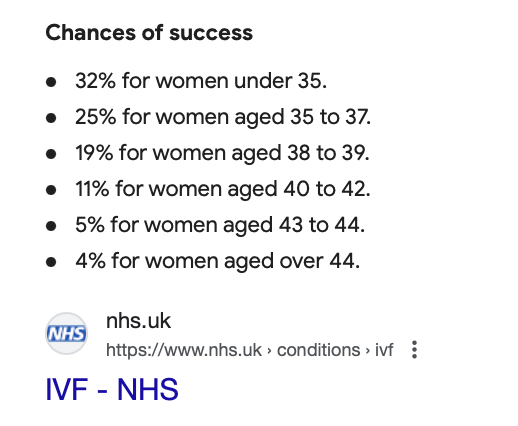
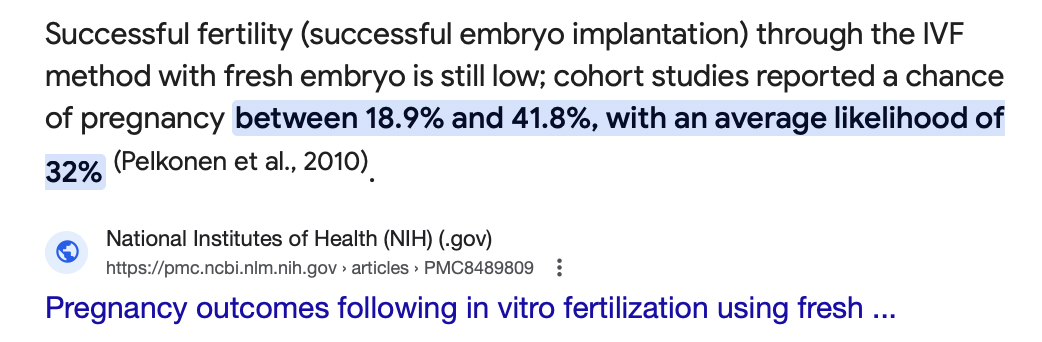
1 Like
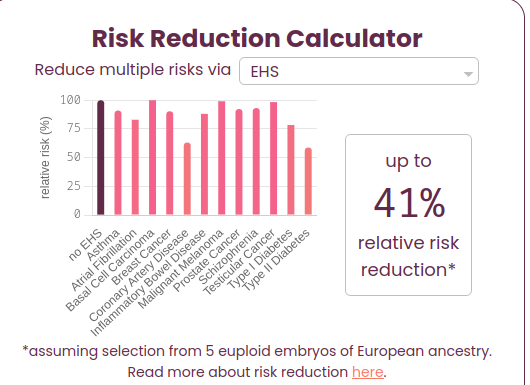
What’s hypothetical with embryo selection? There are multiple companies offering this right now, you can even get the raw data yourself and upload to different sites. For example you can choose to reduce risk of schizophrenia by 52% (schizophrenia == ~zero income):
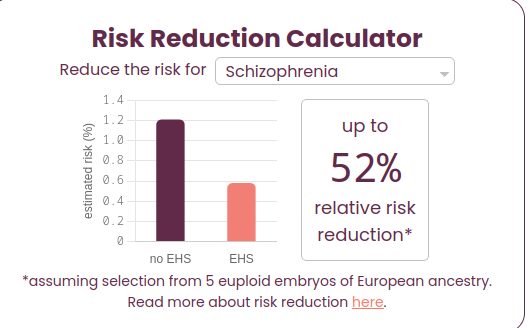
Or in total overall 41% relative reduction:
No, but look at the benefits above.
That’s a good point but:
(1) Does younger surrogate have higher chance of success and thus it will work eventually by switching surrogates if it doesn’t work for one, if so why can’t this be done?
(2) Can’t you combine rapamycin to either increase chance for IVF success after a period of taking it, or to delay the decrease in chance of IVF success?