Important documentary?

Fauci is a hero!

What evidence demonstrated that the vaccines didn’t reduce transmission?
Important documentary?
What evidence demonstrated that the vaccines didn’t reduce transmission?
Shingles vaccines seems to reduce the likelihood of dementia by between 17% and 25% depending on the study (there are 3 well-known studies). But no causal link has been established. These are large, observational studies and have garnered significant interest. They compelled me to get the vaccine despite concerns about reactivating Bell’s Palsy. My father died of Alzheimer’s and my mother died with dementia. So, I’m highly motivated to stack the deck however I can.
The vaccination itself caused an annoying 2 days (one for each shot) of feeling like crap. But ultimately worth the possible reduction in risk of dementia.
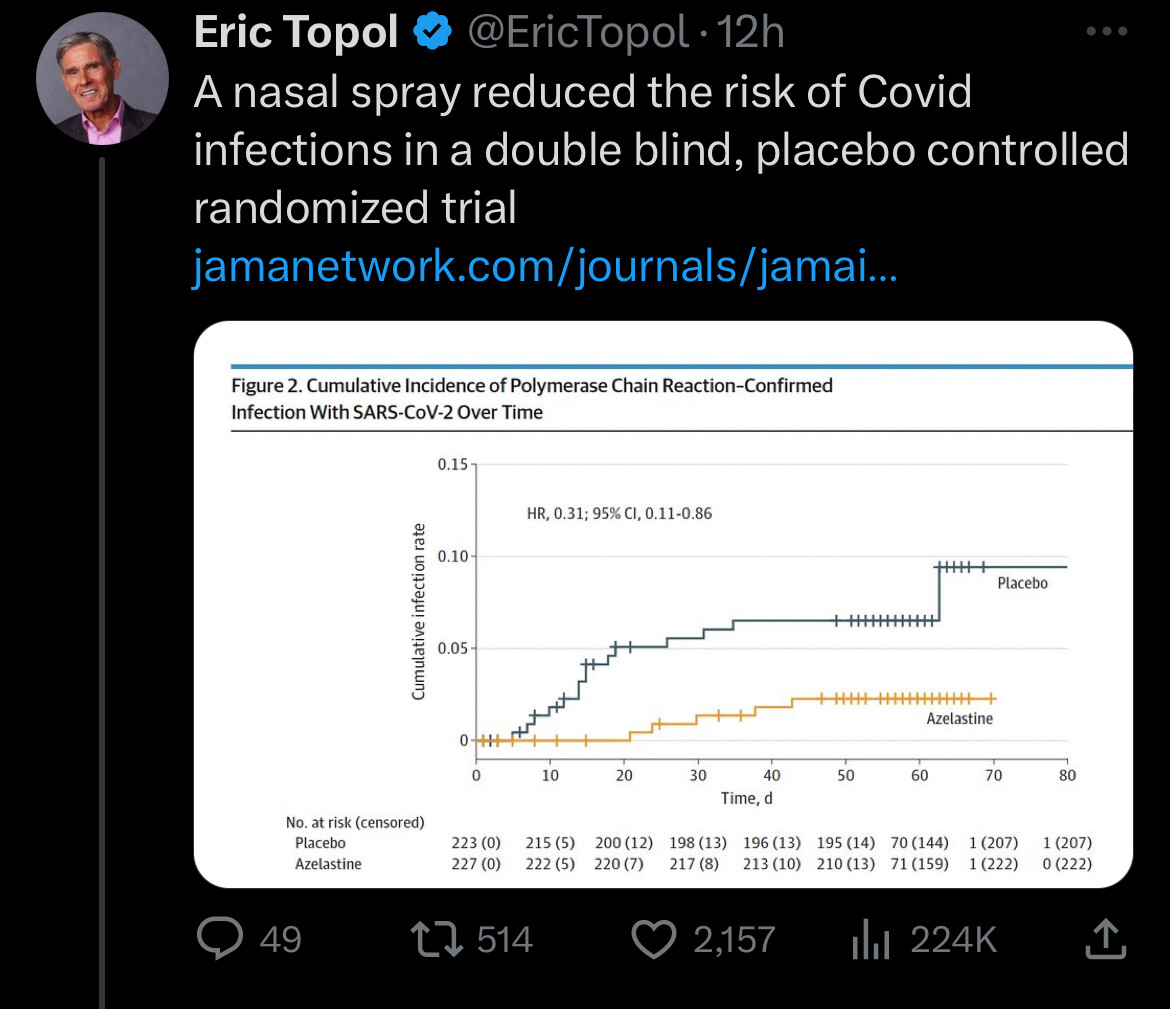
Thought some of you might be interested to see this:
Findings In this randomized placebo-controlled clinical trial that included 450 participants, the incidence of laboratory-confirmed SARS-CoV-2 infections was significantly lower with application of azelastine nasal spray compared with placebo treatment.
https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2838335
I have had and thrown away azelastine because I couldn’t deal with the taste.
I do have Olopatadine spray to use before bed on rare occasion if I’m a bit stuffy. I don’t know the pros and cons of using these things more often, or even if a non azelastine spray would even work.
Azelastine is about $6 USD for 120 doses here in Hong Kong. Since I get COVID every Spring, I’ll probably pick some up and start using it in February.
@DeStrider @Neo
I wonder what is special about this particular spray, or if some of the other histamine sprays work, like olopatadine or even enovid etc.
I say this only because I haaaate azelastine.
It doesn’t seem ‘any’ spray would do because the placebo group I assume had some sort of spray (maybe saline).
I use Profi nasal spray. It lasts 8 hours. Have been using it for 2 years and so far so good - no viral infections (knock on wood).
It’s hard to tell if it’s a class effect or something specific for Azelastine. But I can tell you from my experience is that if you can taste your azelastine, you are using the nasal spray improperly. Most people do. Here are the proper instructions: RYALTRIS® - Nasal Spray | How to Administer RYALTRIS®
The only changes I would add specifically for you are: tilt head forward more aggressively, do not inhale at all and actually blow out the excess - with that the spray should not end up running down in to your throat where your tongue will pick up the bitter taste.
Moreover, use Astepro OTC rather than generic azelastine it’s 50% stronger so only 1 spray/nostril needed and they added sorbitol to offset the bitter taste a bit.
It looks some of the anti-viral effect is class effect and some other may be specific for azelastine. I also prefer olapatadine but may have to get some Astepro instead.
The specific mechanism by which azelastine works against viral infections is not fully understood but is believed to involve a combination of anti-inflammatory actions, modulation of cellular receptors like ACE2 and integrins, inhibition of viral proteins, and effects on the nasal mucosa’s ability to block viral entry. Research suggests these broad effects contribute to its observed antiviral activity against viruses such as SARS-CoV-2, RSV, and influenza.
Potential Mechanisms
Evidence
Excellent follow up, thank you!
Do you happen to know if there any negative consequences of using astepro often (esp. when it’s not needed for a stuffy nose)?
I’m just wondering if I should use it any time I’m out and about because why not, or if I should be a little more particular about when I might use it, packed restaurant, etc.
Can’t wait to try your tips on not tasting it!!
I am always concerned with the anticholinergic effects on the brains of elderly adults.
So, I asked ChatGPT 5 in paid think mode.
Query:
“Do you think azelastine would have the same adverse cognitive effects on elderly people as other antihistamines, such as diphenhydramine, doxylamine succinate, etc.?”
Bottom line: Generally safe for elderly adults.
I won’t post the complete response. If you want to see it:
https://chatgpt.com/c/68b9e1fc-fb20-832a-b51a-11dcd6b86eff
Astepro is only 200 mcg (0.2 mg) per spray. Oral anti-histamines dosing can very between 10 mg to 180 mg, If you blow out excess instead of swallowing I estimate 60-80% will be expelled. I wouldn’t expect many systemic side effects with the low dose. The only side effect would be excessive nasal dryness if you nose is already dry (or have Sjorgen’s) , problem here in Arizona (probably not in Florida). I use my medicated spray after a saline nasal wash.
I also asked ChatGPT 5 for a theoretical dosing protocol for using azelastine nasal spray for possible prevention of SARS-CoV-2 infections.
Query: “What would be the theoretical dosing protocol using azelastine nasal spray for the possible prevention of SARS-CoV-2 infections?”
Reply FWIW:
Short version: if you want to copy the only randomized clinical trial to date, you’d use azelastine 0.1% nasal spray, 1 spray per nostril, three times daily (TID) for 56 days during the risk period. That’s exactly how it was given in a phase-2, double-blind RCT (450 adults) that cut PCR-confirmed COVID-19 from 6.7% (placebo) to 2.2% (OR 0.31).
If you only have OTC Astepro 0.15%
Each 0.1% spray delivers 137 mcg; each 0.15% spray delivers 205.5 mcg. The trial’s total daily amount (0.1% TID, 1 spray/nostril) ≈ 822 mcg/day. You can approximate that with 0.15% 1 spray/nostril BID (≈822 mcg/day).
Label limits for 0.15% (≥12 y): ≤4 sprays per nostril/day. (So BID plus an occasional “top-up” still stays within label.)
Seems a little tedious for me. I think I will skip it for now.
I’m baaaack…
The updated covid vax is now available here. It’s been almost a year since my last jab, so I’m ready.
Question, what is the ideal way to time this with my last dose of rapa?
My last dose was Saturday, 6 days ago. Is it fine to get my covid vax now or should I wait a little longer?
Also, how long afterwards would you wait to take your next dose of rapa
And… are there any supplements you would take or avoid the day of vax, or for a couple of days afterwards? I assume it’s business as usual.
Would part of the protective effect be diminished by not partially covering throat and mouth mucosa?
^^^ There are different types of vaccines, which may or may not be healthy (thats the argument)
I think the live attenuated/inactivated/subunit vaccines which people are mentioning that do have somewhat proven health affects like flu/shingles/ may be more natural to the body than mRNA, though I’m not an expert. So I will wait on the covid, but I do get other vaccines
I don’t know. Usually it’s the nasal passages where most of the actual infections occur… assuming one is not a mouth breather. But if she cannot tolerate the taste, at least she can cover the nasal mucosa.