OK. But I’m having a slightly anemic reaction to this study (ahem! apologies, couldn’t resist). To me the most relevant quote from the study was this:
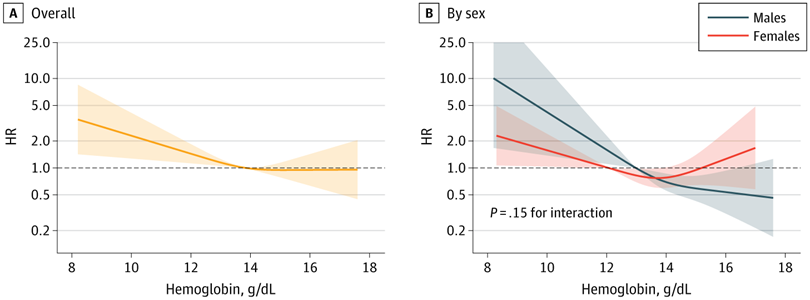
“Anemia was defined according to World Health Organization criteria.”
And what is that? It’s hemoglobin below 12.0 g/dL for women and 13.0 for men.
If someone has such numbers, this is notable. Hardly anyone does (on this list).
Meanwhile, the relationship between iron status and anemia is a huuuuuge can of worms, as seen in this thread. Many of us have what might be seen as below range iron levels, but absolutely don’t have anemia according to WHO criteria.
As an example my numbers from my most recent LabCorp test:
TIBC - 405 ug/dL (ref. 250-450)
UIBC - 330 ug/dL (ref. 111-343)
Iron - 75 ug/dL (ref. 38-169)
Iron Saturation - 19% (ref. 15-55)
Ferritin - 20 ng/mL (ref. 30-400) flagged as Low by LabCorp.
And in the same test, my hemoglobin was 15.4 g/dL (ref. 13.0-17.7).
So, I certainly seem to be on the low side of iron status, but pretty robust hemoglobin number far from WHO anemia. As I’ve reported I don’t experience any of the typical anemia symptoms and my energy levels are fine.
How useful is this connection (anemia/AD) to most of those of us on this list who struggle with their iron status? I don’t know.
Also, if you dig into this study, it becomes ever more equivocal, with a variety of factors (BMI included, nutrition status etc.) and after adjustments barely on the border of significance. Like I said: anemic.
The signal may be there, but we need much stronger results, especially those which might allow us to define optimal iron biomarkers (which was not even the focus of this study).