What are your thoughts on that it increases insulin levels (and in a continuous, not just post randial as in the normal insulin cycle).
I understand it can be valuable for weight (and if combined with good exercise for body composition), but am wondering if it perhaps it not good with contact GLP-1 modification for longevity?
No. PushHealth is via text only. I recommend getting oral Semaglutide from India. Just as effective if you take in a completely empty stomach with very litttle water for 30 minutes
I am not taking it currently. And, when I was it was only once a month (ish) in very low dose. I did check my insulin during that time and it didn’t increase.
I just ordered some Rybelsus (oral semaglutide 7mg and 14mg tablets), which hopefully should be here in a few weeks. Will be interesting to see if it cuts my appetite and has any effect on body fat loss given the lower potency vs injectable semaglutide. I’ll post my results here.
The trial ended last year. The results haven’t been published. But Novo Nordisk’s Annual Report 2023 says: “Phase 1 trial investigating the effects of the combination of semaglutide and SGLT2i inhibitor dapagliflozin in people with T2D was completed. The project was terminated.”
Phase 1 is normally for safety and pharmacokinetics. I think that companies are required to report serious and unexpected adverse reactions to the regulatory authorities immediately. So I assume that the project was not terminated due to safety reasons but for commercial reasons? Dapagliflozin was developed by Bristol-Myers Squibb in partnership with AstraZeneca. So maybe Novo Nordisk didn’t want to work with its competitors?
On the other hand, Novo Nordisk’s FLOW trial of semaglutide in people with T2D and CKD ended early due to efficacy in October 2023, and they’ve just reported “a statistically significant and superior reduction in kidney disease progression as well as cardiovascular and kidney death of 24% for people treated with semaglutide 1.0 mg compared to placebo”. Given that many people with T2D and CKD are already on SGLT2i (and they were not excluded from the trial), I assume that many in this trial were on semaglutide + SGLT2i. Unfortunately, “The detailed results from FLOW will be presented at a scientific conference in 2024.” As noted by a practician here: “Clinically I cannot wait to see what combination therapy with SGLT2 inhibitors and/or Kerendia will demonstrate.”
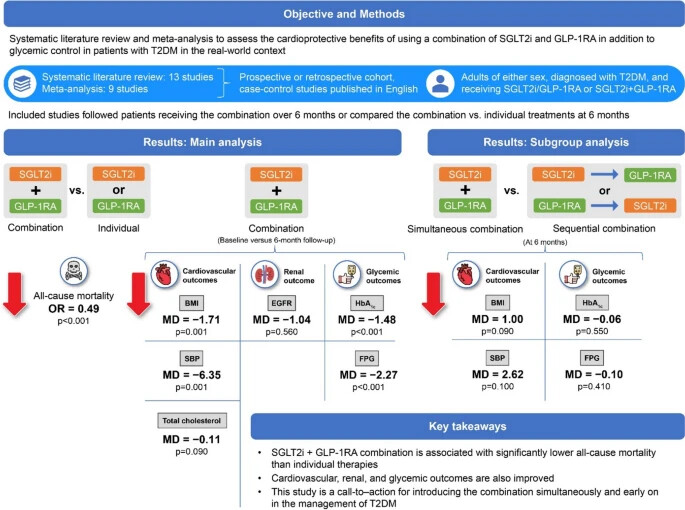
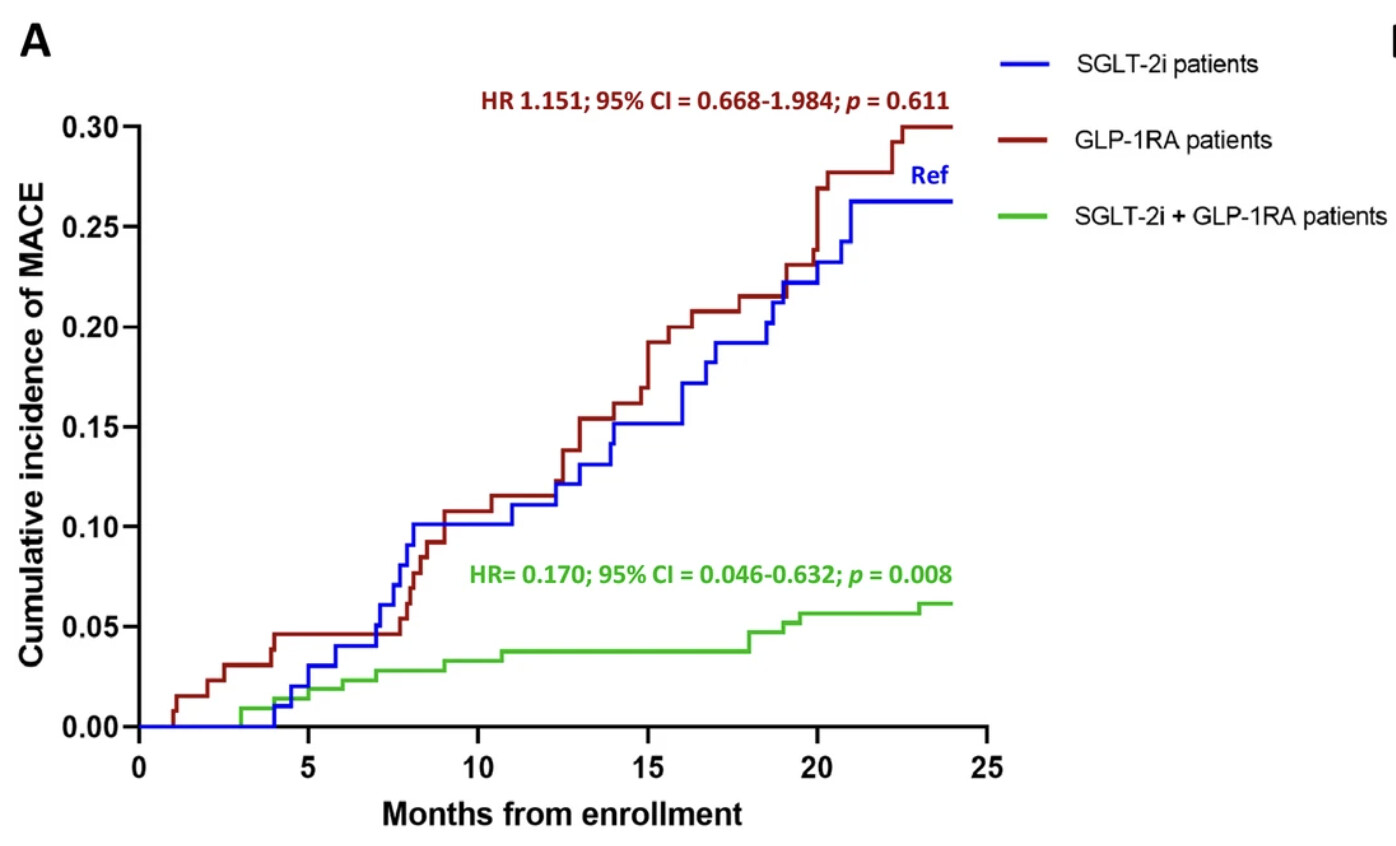
The combination of SGLT-2i and GLP-1RA is associated with a reduced incidence of cardiovascular events in patients with T2D and AMI compared with either drug used alone, with a significant effect also on peri-infarcted myocardial rescue in patients without a second event.
(Regarding the cancer risk, this India paper concluded: “Semaglutide use in RCTs and real-world studies was not associated with an increased risk of any types of cancer, and this conclusion is supported by a high grade of evidence.”, Semaglutide and cancer: A systematic review and meta-analysis 2023)
Is Attia wrong? (to be fair, he published his article in February 2023, while most of the above articles were published later in the same year)
Novo Nordisk is conducting trials on semaglutide for nonalcoholic fatty liver disease (NAFLD) in non-obese and non-diabetic people so we’ll soon know how good semaglutide is in this context.
I think that semaglutide + SGLT2 together can be very powerful, wrt health benefits
However, I currently use semaglutide but very intermittently (one 7mg tablet every three weeks). This is for multiple reasons:
I still observe subtle noticeable effects .
I did not want to develop tolerance by taking the high recommended dose
I feel fatigue and loss of motivation if I am on a higher or a more continuous dose — even here I try to make sure that I don’t take it immediately before a deadline for example.
With respect to SGLT2 + Semaglutide:
Combining them increased my fatigue / led to slight hypoglyceamic feeling, which is not only not fun, but also makes me want to go eat a bunch to feel better.
I now look to use SGLT2 during the trough of semaglutide, and trough of rapamycin (especially if I’m taking a larger 25mg dose of empagliflozin), and when I am having carby and sugary meals (happens mostly while traveling, where I lean into being a ‘foodie’)
I feel like I’m in a good zone with this protocol.
Another reason for my intermittent dosing is because I’m conserving my current stack lol.
I have acarbose every day before starchy meals.
And metformin occasionally with rapamycin.
Have you tried the lowest dose instead (oral semaglutide 3 mg)? And why don’t you abandon acarbose and metformin for just daily SGLT2i + semaglutide 3 mg?
Ah yeah I used to use 3mg. I might have continued but I don’t have access to it now.
I don’t see a reason to abandon acarbose.
Maybe low dose daily SGLT2i once I have access to enough. But I hesitate during peak semaglutide because of what I mentioned, and also around peak rapa, because I do want to minimize any potential UTI.
I’ve mostly used 25mg empagliflozin, which I’ve occassionally halved (e.g. if I’ve taken 25 consecutive days in a row). I’ve tried cana before, but mostly empa.
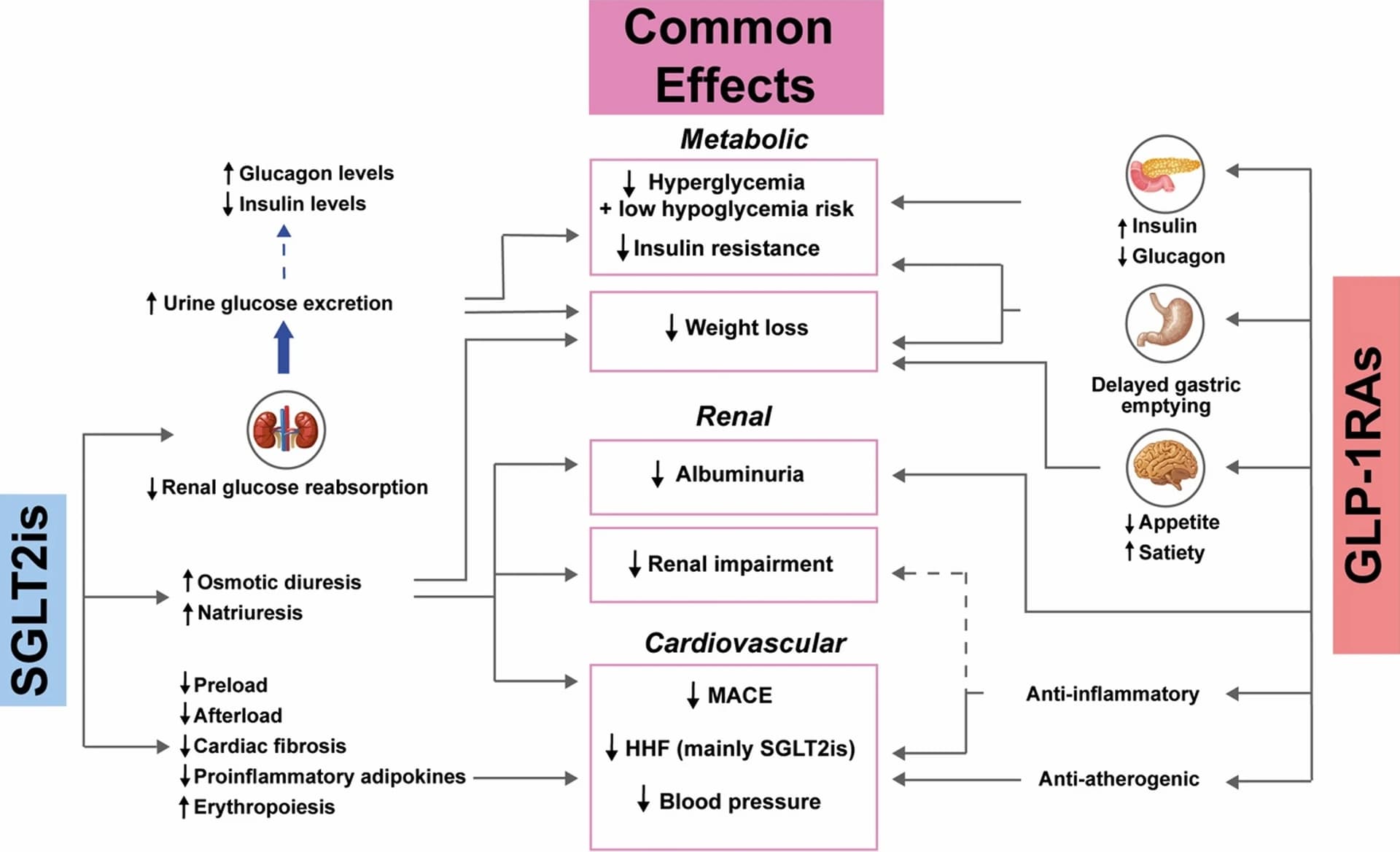
From your reading, do you know if it’s only reabsorption of glucose that is inhibited by SGLT2is or are there other compounds too? Albuminuria is suggested in the diagram, I see. I wish somebody also measured the amount of plastics and PFAS that are eliminated due to SGLT2is (if any).
I do wonder if their oppositive effects on insulin are synergestic or cancel out some effects (for e.g. on appetite supression).
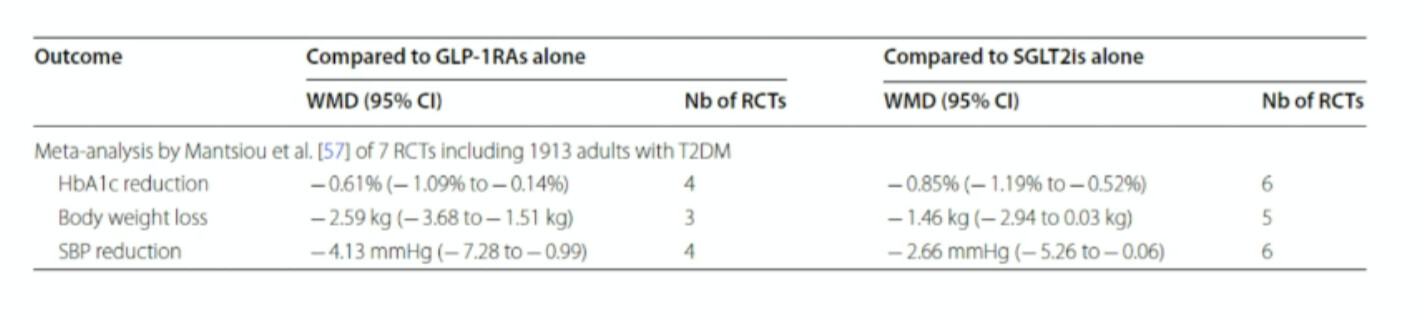
From what I read, effects are additive for weight loss, synergistic for blood pressure lowering, and complementary but non additive for Hb A1C reduction:
It’s interesting that they’re additive for several health benefits, but not for diabetes (based on HbA1C), given that they’re both originally diabetes medications!
Some experts have said that we may also look back on GLP-1 drugs as one of the greatest modern advancements in the treatment of chronic conditions. They’ve already shown promise for cardiovascular, liver and kidney disease, and some are now being tested on Alzheimer’s, sleep apnea, PCOS—even addictive behaviours, like gambling. That is ahugescope.
Are these drugs going to help all of these different conditions in a meaningful way? That’s unlikely. We don’t yet have enough data to say we should put this stuff in the drinking water, but there are encouraging signs of their benefits. Right now, we have excellent data for Type 2 diabetes, heart disease and obesity. We’re gonna get some excellent data for kidney disease in the next few months, then heart failure in the summer. We’ll have to wait a year or two for Parkinson’s and Alzheimer’s.
I lost 65 lbs of scale weight and gained 1kg of lean mass while on tirzepatide (Mounjaro). I got DEXA scans. If one gets adequate protein and lifts heavy weights at least 2x a week (I was doing 3-4, progressive overload), one does not have to lose muscle. There are many similar anecdotes online. Judging by the online forum participants, most people on these drugs are obese women who don’t lift weights. Of course they lose muscle. These are the people who are letting the drug do all the work for them (not even tracking calories and macros, etc.)
Btw, tirzepatide is generally regarded by those who have tried both to be vastly superior to semaglutide in terms of effectiveness and the side effect profile. Retatrutide is even better in some respects because one tends to have more energy (less fatigue) on it. Tirz usually begins working within a couple days of the initial injection, but with sema you have to slowly increase the dose because the side effects are otherwise often intolerable. Reta usually takes 2-4 weeks to kick in, but when it does, you simply have zero appetite. I wouldn’t waste time with semaglutide.
I think the fatigue comes from allowing caloric intake to drop too low. It’s easy to not eat enough and especially not eat enough carbs when you’re trying to prioritize hitting a protein target, because after protein and fat, you might not have a lot of room left in your energy budget for carbs. I suppose the keto people wouldn’t have this issue, but I don’t function well on a keto diet and needed some carbs.
I tracked calories in Cronometer, weighing and measuring everything, and tried to not let my deficit get too low.
The other thing was to exercise daily no matter what (well, sometimes Sunday off). I mostly just alternated cardio with weights, and I didn’t slack off in terms of intensity with either.
Now with retatrutide things are a little different because the glucagon receptor agonist activity seems to provide an energy boost (a common anecdote and my experience). Retatrutide feels better than tirzepatide, I think, partially because of this. You can eat more on reta but the pounds just fall off as if they’re getting torched in a metabolic furnace.