A white paper from the company that is a good overview. Then I’ve done a Gemini analysis of it.
2020-11-30-WhitePaperNovelBiomarkersChronicInflammation-2.pdf (459.7 KB)
Report: The “iAge” Inflammation Clock & CXCL9
Analysis of Edifice Health White Paper & Scientific Validation
Part 1: The Executive Summary
Title: The Inflammation Clock: AI Uncovers the Immune Signal “CXCL9” as a Driver of Cardiovascular Aging
Narrative:
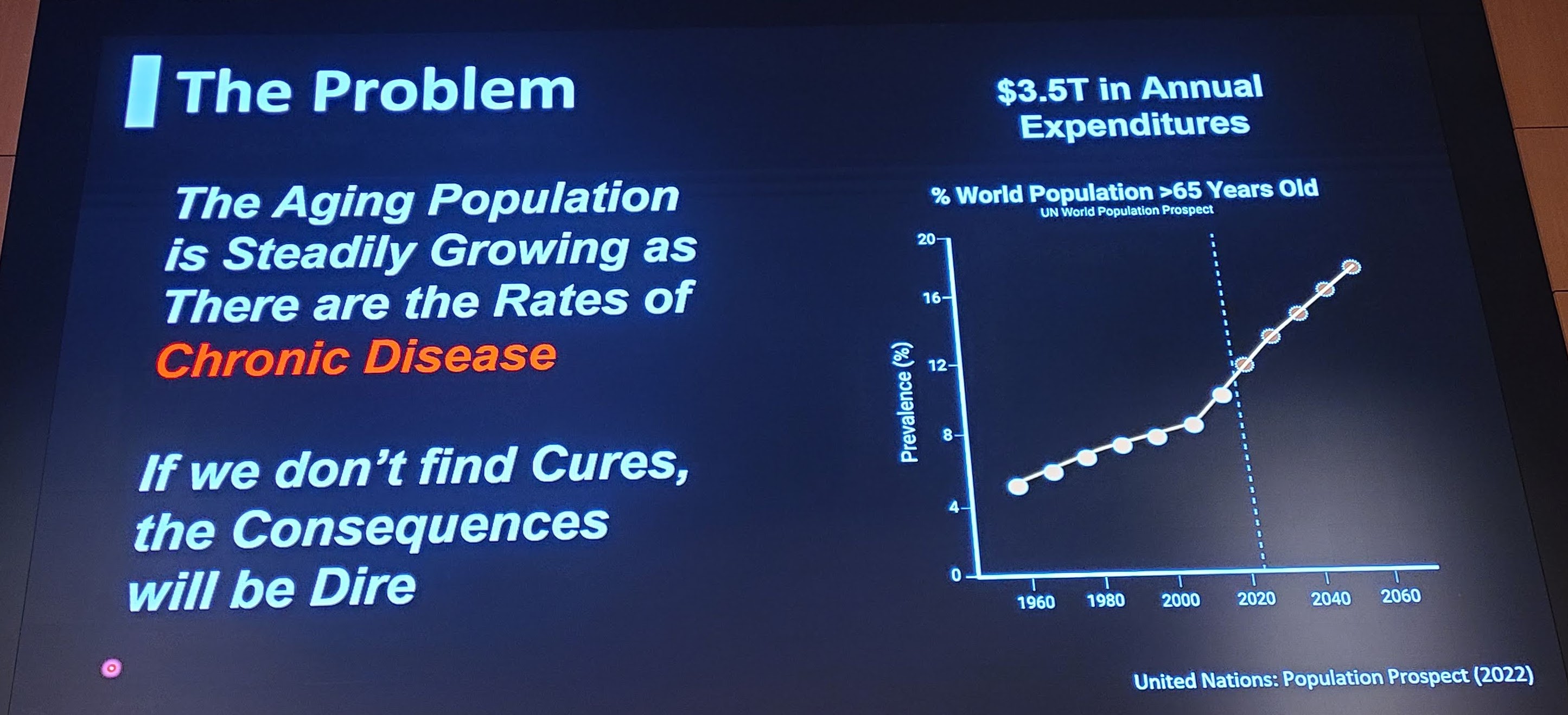
We have long known that chronic inflammation is the “smoldering fire” beneath the diseases of aging, but we have lacked a precise fuel gauge. Standard markers like C-Reactive Protein (CRP) are blunt instruments—good for detecting acute infection, but poor at quantifying the subtle, lifelong accumulation of immune damage known as “inflammaging.”
Researchers from the Stanford University School of Medicine (USA) have deployed deep learning on the “1000 Immunomes” dataset to construct a novel metric: iAge (Inflammatory Age). Unlike chronological age, iAge measures the cumulative burden of Systemic Chronic Inflammation (SCI). In the pivotal validation, this metric outperformed chronological age in predicting multimorbidity, frailty, and specifically, cardiovascular decline.
The “Big Idea” here is not just a new score, but the isolation of a specific molecular culprit: CXCL9. This chemokine was identified as the loudest signal in the inflammatory noise. The study suggests CXCL9 is not merely a bystander but an active driver of arterial stiffness and endothelial senescence. While the white paper frames this as a commercial breakthrough for Edifice Health, the underlying science—eventually published in Nature Aging—provides a compelling mechanism linking immune signaling directly to the loss of vascular elasticity. For the longevity enthusiast, this shifts the focus from “lowering inflammation” broadly to targeting specific chemokine pathways that rigidify our arteries.
Context & Impact:
-
Institution: Stanford University (USA) / Edifice Health.
-
Journal: The white paper cites Nature Medicine (Under Review), but the verified peer-reviewed publication appeared in Nature Aging (2021).
-
Impact Evaluation: The impact score of Nature Aging is 16.6 (2023), evaluated against a typical high-end range of 0–60+ (where Nature Medicine is ~58). Therefore, this is a High impact journal (specialized top-tier), though distinct from the Elite general medical status of Nature Medicine originally targeted in the white paper Nature Aging Impact (2024).
Part 2: The Biohacker Analysis
Study Design Specifications (Verified Source)
-
Source Paper: An inflammatory aging clock (iAge) tracks multimorbidity… (2021)
-
Type: Human Observational Cohort (Stanford 1000 Immunomes) + In Vitro Mechanism + Murine Validation.
-
Subjects:
-
Human: 1,001 individuals (aged 8–96 years).
-
Validation Cohort: 19 healthy older adults (Framingham Heart Study subset).
-
Animal: Young (2 mo) vs. Old (24 mo) C57BL/6 mice.
Mechanistic Deep Dive
The study moves beyond the “cytokine storm” concept to identify CXCL9 (a T-cell chemoattractant) as the master regulator of vascular aging.
-
Vascular Stiffness: CXCL9 suppresses endothelial cell function, preventing them from relaxing and repairing blood vessels. This directly promotes arterial stiffening—a primary driver of hypertension and heart failure in the elderly.
-
Reversibility: In mouse models and human cell cultures, silencing CXCL9 reversed the aging phenotype. It restored endothelial proliferation and reduced cellular senescence.
-
The “iAge” Metric: This is a composite score of ~50 cytokines. An individual can be “chronologically 50” but have an “iAge of 70,” predicting a significantly higher risk of frailty and multimorbidity.
Lifespan Data
-
Lifespan Analysis: No direct lifespan extension (mortality endpoint) was tested in the intervention arm of this study. The study established correlation with exceptional longevity (centenarians had lower iAge), but did not prove causation for lifespan extension in a treated cohort.
-
Translational Gap: The “silencing” of CXCL9 was achieved via genetic/molecular tools (shRNA) in the lab, not a commercially available pill.
Novelty & Critical Limitations
-
Novelty: The application of AI to immunometrics is genuine innovation. Most inflammation panels (IL-6, TNF-a) are too variable; iAge aggregates them to find a stable signal. Identifying CXCL9 as a causalagent (rather than just a marker) is the major scientific value-add.
-
Critical Limitations:
-
Commercial Bias: The white paper is a sales tool for Edifice Health.
-
Trial Termination: The Edifice Health clinical trial (NCT04983017) testing supplements to lower iAge was Terminated. This is a critical signal that the “solution” phase may have hit feasibility, safety, or business hurdles.
-
Complexity: CXCL9 is not part of standard LabCorp/Quest panels, making the metric inaccessible without the proprietary test.
Part 3: Claims & Verification
Claim 1: “Systemic Chronic Inflammation (SCI) is the root cause of age-related disease.”
Claim 2: “iAge predicts cardiovascular aging and multimorbidity better than chronological age.”
-
Verdict: Level C (Correlation).
-
Evidence: The Nature Aging paper supports this correlation in the Stanford cohort and validation sets. However, prospective data (predicting future events in a new group) is limited compared to established metrics like the GrimAge clock.
-
Source: An inflammatory aging clock (iAge)… (2021)
Claim 3: “Edifice Health interventions can lower iAge.”
-
Verdict: Level D/E (Unverified/Terminated).
-
Evidence: The specific clinical trial (NCT04983017) designed to prove this was terminated. While a separate study on Oats (Avena sativa) showed reduction in a related marker (Eotaxin-1), the broad claim of a “solution” remains clinically unproven in a completed Phase II/III trial.
-
Source: Study NCT04983017 Status: Terminated
Part 4: Actionable Intelligence
The Translational Protocol: Targeting CXCL9
Since the proprietary “iAge” supplement trial was terminated, we look to the literature for validated modifiers of the CXCL9/Eotaxin pathway.
1. Intervention: Whole Grain Oats (Beta-Glucan)
-
Mechanism: A specific study using the iAge metric found that oat consumption reduced Eotaxin-1, a chemokine closely linked to the iAge profile, independent of weight loss.
-
Protocol:
-
Dose: Equivalent to ~3–4g of beta-glucan daily (approx. 1 large bowl of steel-cut oats).
-
Feasibility: High. Readily available food source.
-
Cost: Negligible ($0.50/day).
-
Safety: GRAS (Generally Recognized As Safe). Contraindicated only for celiac disease (unless certified gluten-free).
2. Biomarker Verification Panel
If you cannot access the Edifice “iAge” test, use these proxies:
-
hs-CRP: The standard baseline (Target: < 0.5 mg/L).
-
Fibrinogen: A clotting factor that rises with vascular inflammation.
-
Omega-3 Index: Indirectly correlates with lower inflammatory load.
-
Advanced: CXCL9 levels are occasionally available in “Cytokine Panels” from specialty labs (e.g., Mayo Clinic Labs, EmpowerDX), but are expensive (~$300+).
3. Pharmacological Speculation (High Risk)
-
JAK Inhibitors (e.g., Ruxolitinib): These drugs block the JAK-STAT pathway, which downstream regulates CXCL9.
-
Safety Warning: Phase I/II Safety data shows significant risks (infection, thrombosis, malignancy). NOT recommended for biohacking/longevity due to poor risk/benefit ratio in healthy adults.
-
Status: Data Absent for longevity application.
Part 5: The Strategic FAQ
Q1: The white paper cites “Nature Medicine,” but the paper is in “Nature Aging.” Is this a red flag?
-
Answer: It suggests the paper was “cascaded.” It was likely submitted to Nature Medicine (IF ~58), rejected/transferred, and accepted by Nature Aging (IF ~16). The science is still top-tier, but the “Elite” impact claimed in the marketing draft was not fully realized.
Q2: The clinical trial for the iAge intervention was “Terminated.” Why?
-
Answer: ClinicalTrials.gov lists the status as terminated. This often happens due to recruitment failure, lack of funding, or early safety signals. Without a published explanation, we must treat the “commercial solution” (supplements) as unproven.
Q3: Can I measure iAge without Edifice Health?
-
Answer: No. The AI algorithm is proprietary. However, you can track the outcomes iAge predicts: arterial stiffness (via Pulse Wave Velocity) and frailty (Grip Strength).
Q4: Is CXCL9 modifiable by lifestyle?
-
Answer: Yes. The oat study suggests dietary fiber/polyphenols can modulate these specific chemokines. General anti-inflammatory protocols (Zone 2 cardio, sleep hygiene) likely lower it, though specific data is missing.
Q5: Does Rapamycin lower iAge/CXCL9?
-
Answer: [Hypothesis: Strong]. Rapamycin inhibits SASP (Senescence-Associated Secretory Phenotype). Since CXCL9 is a key component of the inflammatory feedback loop in senescent cells, Rapamycin should theoretically lower it, but human data specifically measuring iAge + Rapamycin is Data Absent.
Q6: Should I take “Immune Boosting” supplements based on this?
-
Answer: No. The paper argues against “boosting.” iAge shows that hyper-inflammation (too much immune activity) is the problem. You want “Immune Resilience” (calm baseline, rapid response), not chronic boosting.
Q7: How does iAge compare to Horvath/GrimAge clocks?
-
Answer: They measure different things. GrimAge (DNA Methylation) measures “hardware” aging (epigenetics). iAge measures “software” activity (current immune state). iAge is likely more volatile and responsive to short-term interventions (e.g., a week of bad sleep) than GrimAge.
Q8: What is the “translational gap” for the CXCL9 findings?
-
Answer: The reversal of aging in the study was done by silencing RNA in mice. We do not have a human-safe drug that selectively silences CXCL9.
Q9: Is the “Stanford 1000 Immunomes” dataset public?
-
Answer: Yes, parts of the data are available via ImmPort (SDY112 - verify access). It is a legitimate, high-quality academic asset.
Q10: What is the single best “Next Step” for me?
-
Answer: Since the commercial test is in flux (trial terminated), focus on the **Pulse Wave Velocity (PWV)**metric. The study links CXCL9 directly to arterial stiffness. Measuring your PWV (available in some smart scales/watches or clinics) is the functional readout of the damage iAge claims to predict.