Increasing Muscle Mass in the Elderly
“This study provides evidence that DHEA replacement has the beneficial effect of enhancing the increases in muscle mass and strength induced by heavy resistance exercise in elderly individuals.”
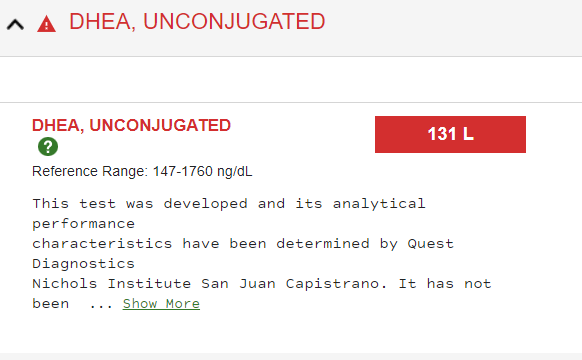
Because your body produces less and less DHEA as you age, I started DHEA supplementation and had a test after 4 months of taking 300mg daily. The results were disappointing, so I am going to increase my daily dose.
"DHEA is an important precursor hormone and is the most abundant circulating steroid present in the human body. Learn more about DHEA at You & Your Hormones, the public information website of the Society for Endocrinology.
Of course, we know we need some steroids to increase muscle mass. ![]()
This leads to the question of rapamycin dosing and mTORC1 inhibition. In the elderly keeping muscle mass is more important than in youth because it becomes increasingly harder to increase muscle mass as we age.
Now that I know that I am very DHEA deficient I am going to up my dose of DHEA and increase my heavy resistance training. So far I have been successful in slowing or stopping sarcopenia at least as far as not losing any strength. Taking rapamycin seems to help with it and also helps with weight reduction. It is very hard to measure muscle mass when you are losing weight. I have a “Smart Scale” that pretends to tell me my total muscle mass, but who knows? Taking bicep measurements is not that helpful while you are losing weight because you are losing some of the surrounding body fat.
I don’t know if an 82-year-old can gain muscle mass, but I am on a new quest to try.
https://journals.physiology.org/doi/full/10.1152/ajpendo.00100.2006