The current dosage used like 6mg/week or 12mg every other week are not optimal in term of time in target range as we generally (*) want to avoid the side effects associated with large doses but using smaller doses does not keep the level at a therapeutic level long enough.
(*) Some might disagree here
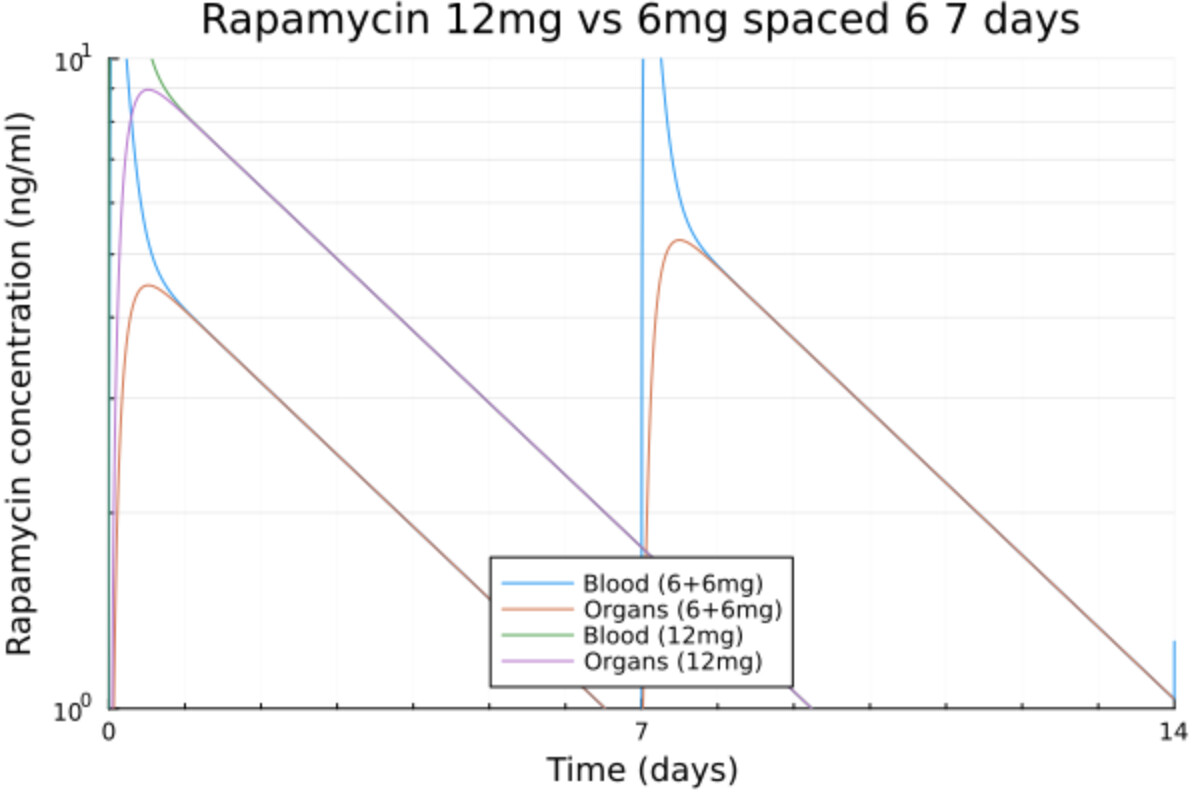
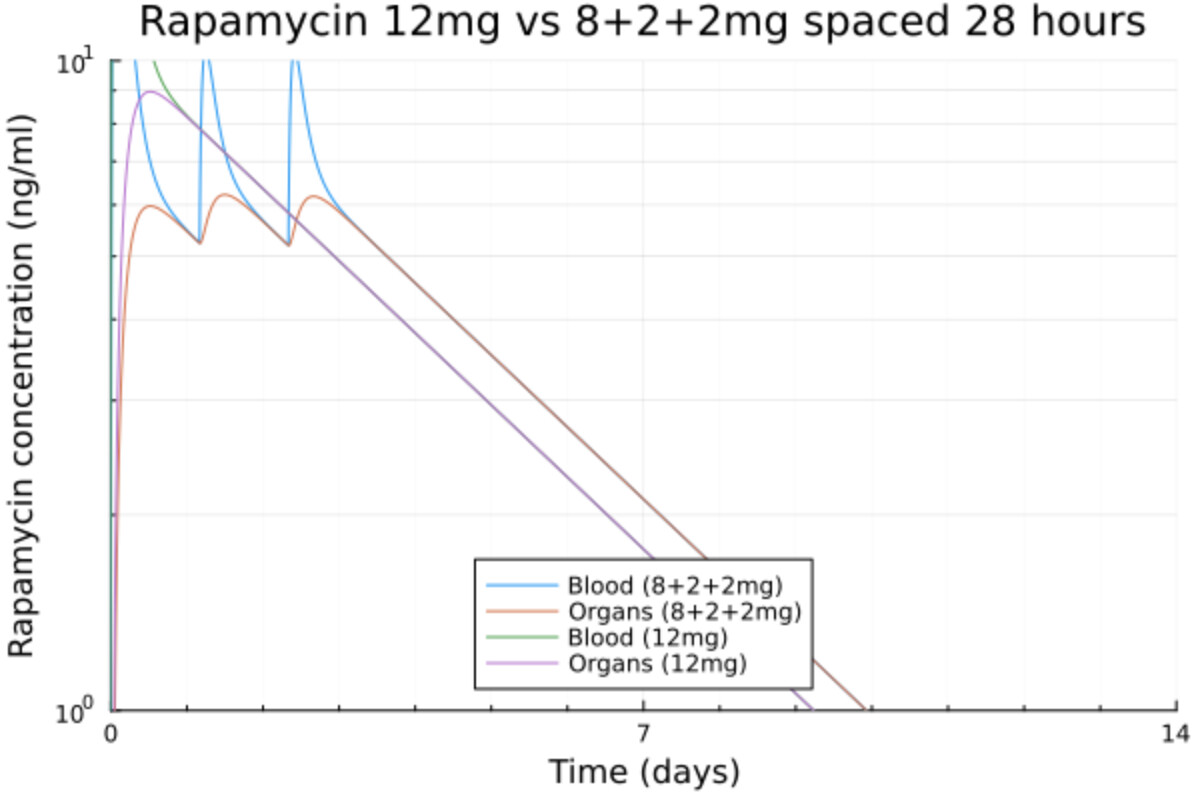
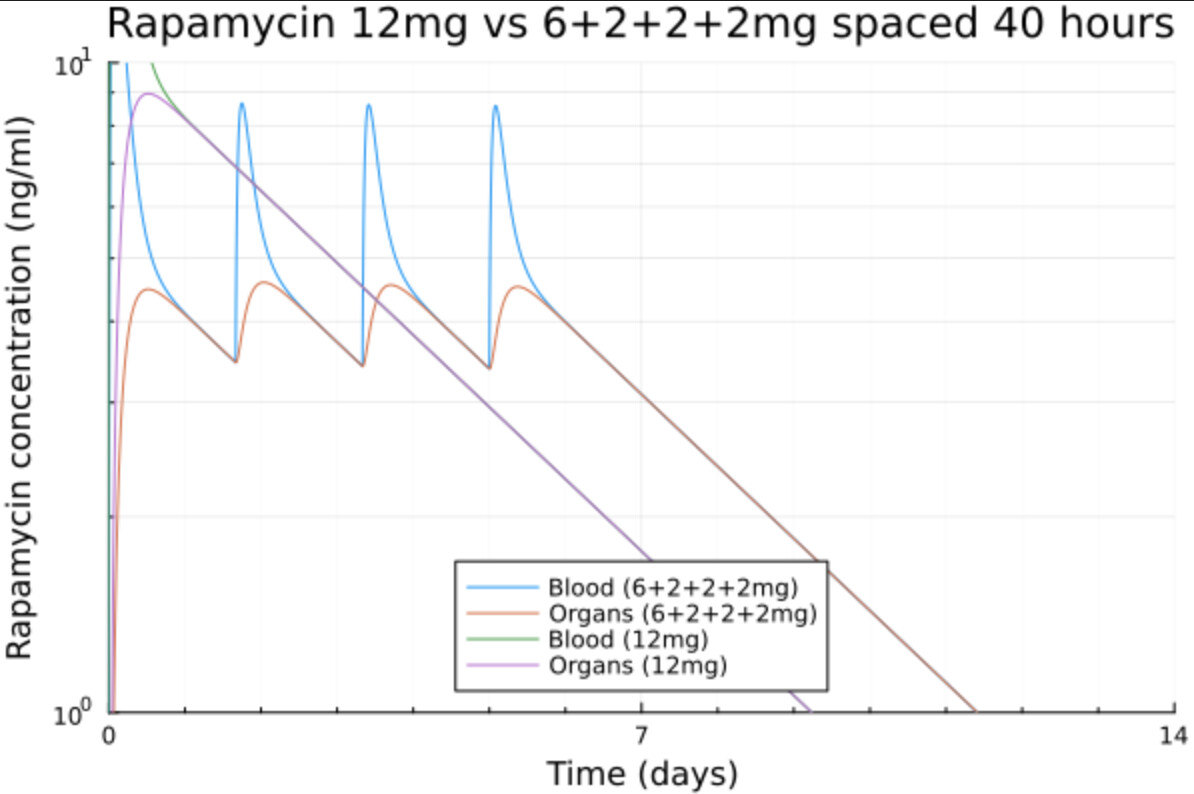
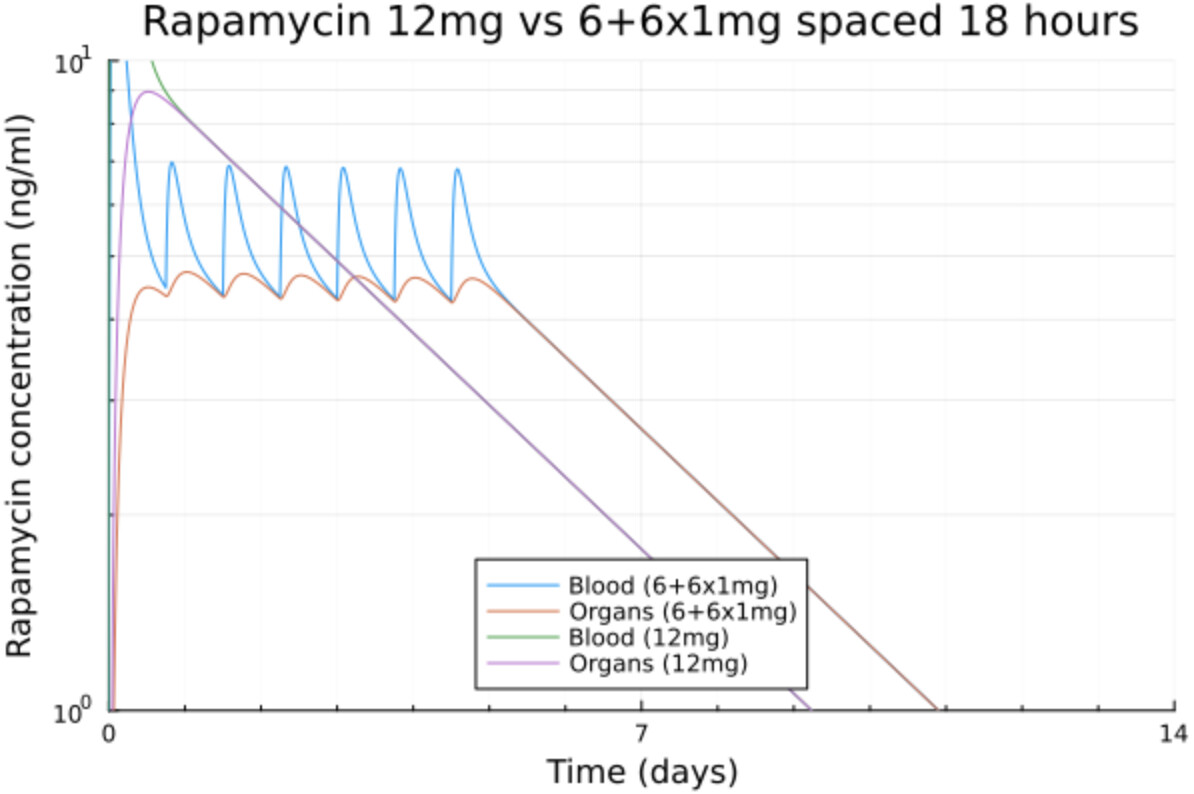
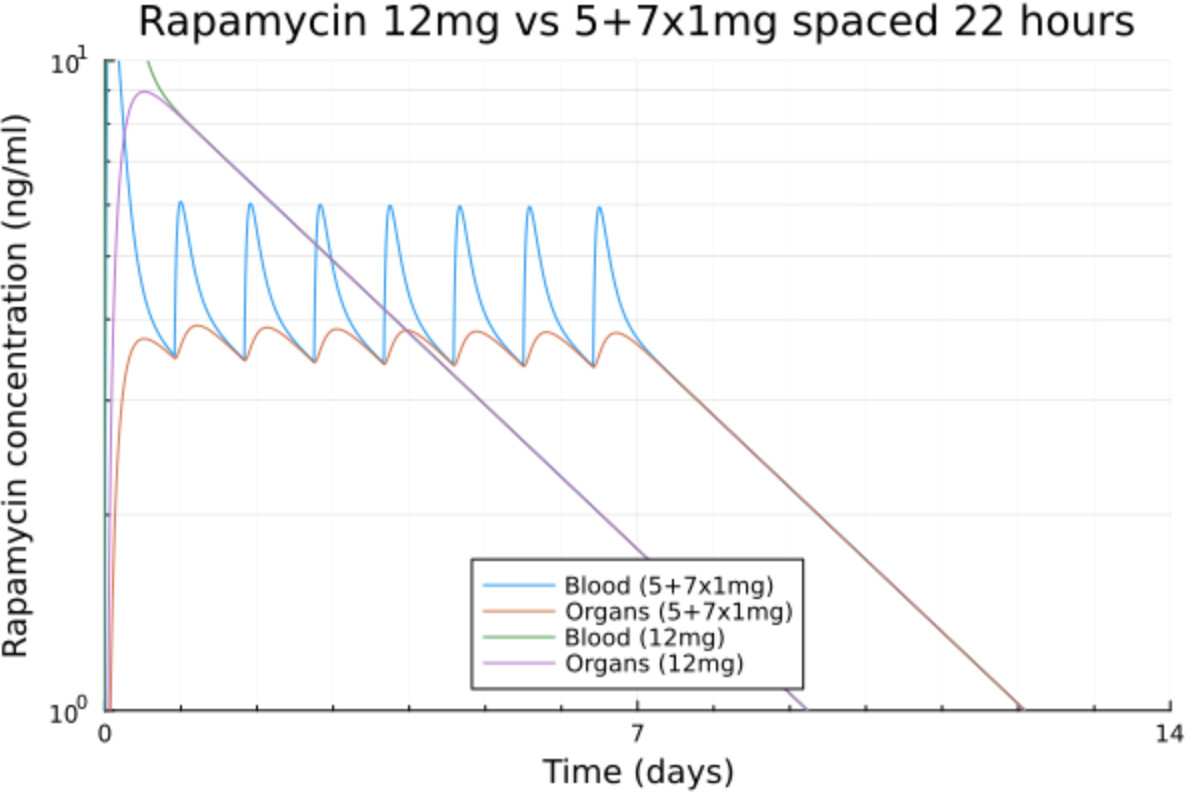
Here is what I get when playing with my rapamycin pharmacokinetics model fitted to my blood tests.
BTW my rapa half life is 65.1h and I have 2mg pills.
The time in range is now increased by 3 days with the same total dose.
Basically by splitting the dose into a starting dose to reach the desired level and then maintaining it by periodic small doses of 1 or 2 mg we can maintain that exact level for the time we want and we don’t get any high levels that can potentially cause issues.
The bigger issue to me is, do we know what the definition of “therapeutic level” for longevity is?, and do we know how “long enough” should be defined also? I mean “too long” is probably defined as when mTORC2 starts getting inhibited, but thats not something we can measure yet.
The problem is that we don’t know what the therapeutic levels are. In particular there is a question as to the extent to which selective mitophagy can be stimulated in stem cells that are quiescent in the stem cell niche. We don’t know if that works or not.
AIUI Optineurin linked selective mitophagy can happen in hypoxic environments. Hence there is a tool. Whether tool can be used or not is unclear.
As we know the data is sparse but taking 5 or 6 mg/week is likely the bare minimum for a meaningful effect. The problem is that the trough will rise over a few weeks and people might end up in some grey zone where the rapamycin effects are not totally on because the dose is low but not totally off because of the trough.
I spent a lot of time chatting with the LLMs but ChatGPT 5.1 and Gemini 3 (both in thinking mode) do not agree. ChatGPT thinks that the usual therapeutic range of 5~15 ng/ml is effective because it does suppress the immune system while Gemini thinks it should be over 15 or at the very least over 10 for longevity purposes as it’s pulsed and not chronic. Another argument of Gemini is higher doses will cross the BBB.
Both agree that the trough should be low and that because of the targeted max levels, a spacing of 7 days is probably not enough for that and that the trough should be below 0.5 for a few days at least.
In my N=1 we see that the trough is not low enough at 6/mg per week and that it’s going to accumulate hence the every 2 weeks protocol.
I don’t think accumulate is the right word here. It’s not like the levels rise endlessly. With once a week dosage, after a few weeks the amount (left in the system just before the next dose) after week i+1 is almost exactly the same as in week i.
The real question is (I believe) is how low the level needs to get in order to not inhibit mTORC2 and how often it needs to get that low (or conversely how long can it stay above a certain level without causing problems).