Thanks @RapAdmin for of this valuable info, very helpful and valuable!
Has anyone measured and seen how IGF-1 changes with rapa N=1?
Thanks @RapAdmin for of this valuable info, very helpful and valuable!
Has anyone measured and seen how IGF-1 changes with rapa N=1?
This really fits with things I’m trying to find and create strategies for - cancer and neurodegen as 2 of the bid 4 seems so much less under our control than cardiovascular and metabolic disease…
That’s what I’m thinking.
From LEF it seems that:
“IGF-1 appears constant over a 24-hour period, making it useful as a bio-marker to help assess blood levels of GH.”
And
”Fasting is not required for this test. Take all medications as prescribed.”
And from Marek it seems like it one the tests that (at least with some assays) can get wacko results if done while having somewhat recent vitamin B7 supplementation:
”Note: This test may exhibit interference when sample is collected from a person who is consuming a supplement with a high dose of biotin. Cease biotin supplementation at least 72 hours prior to blood draw.”
all about growth hormone:

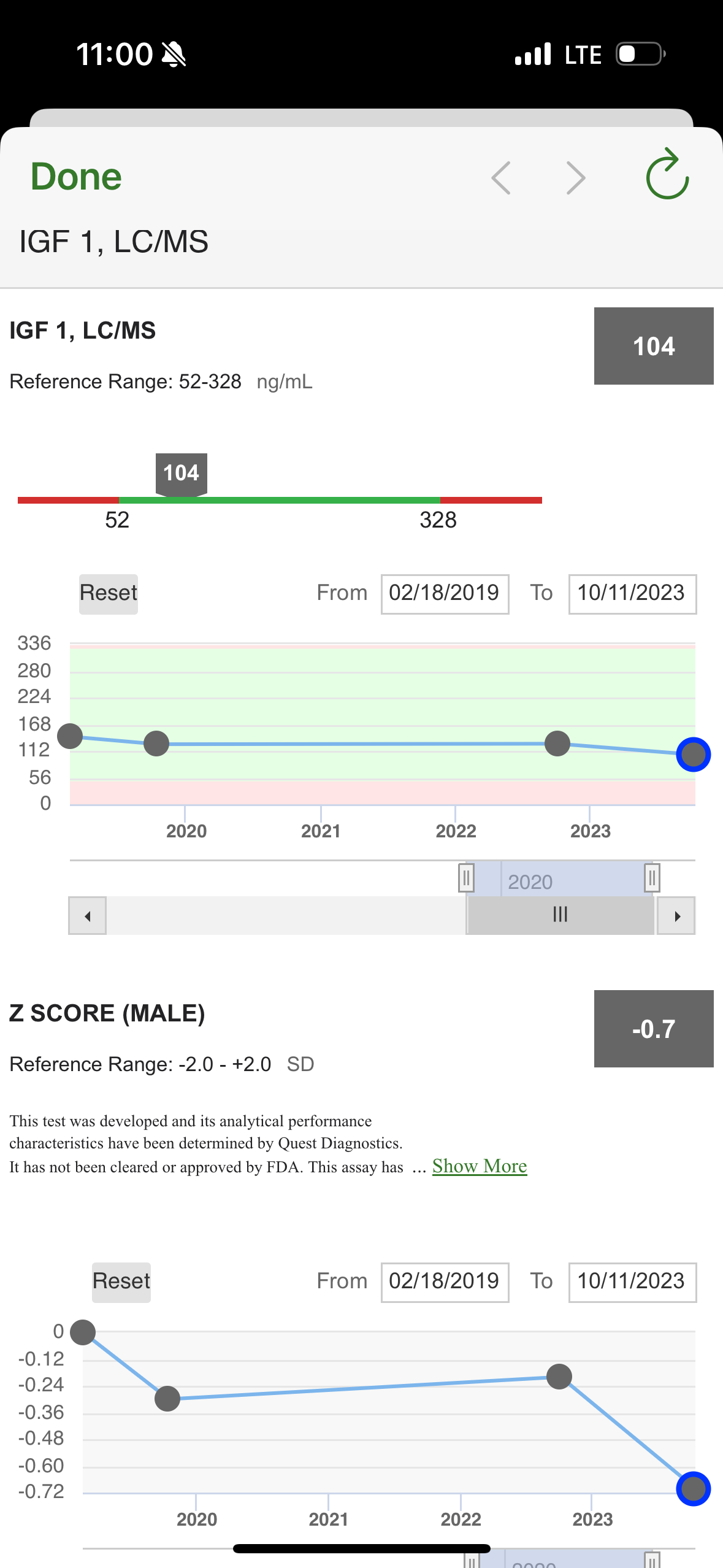
Here are my test results. Seems that as long as I keep working on muscle and resistance training as a foundation against osteoporosis and sarcopenia and I’m not worried about those then lower might be even better?
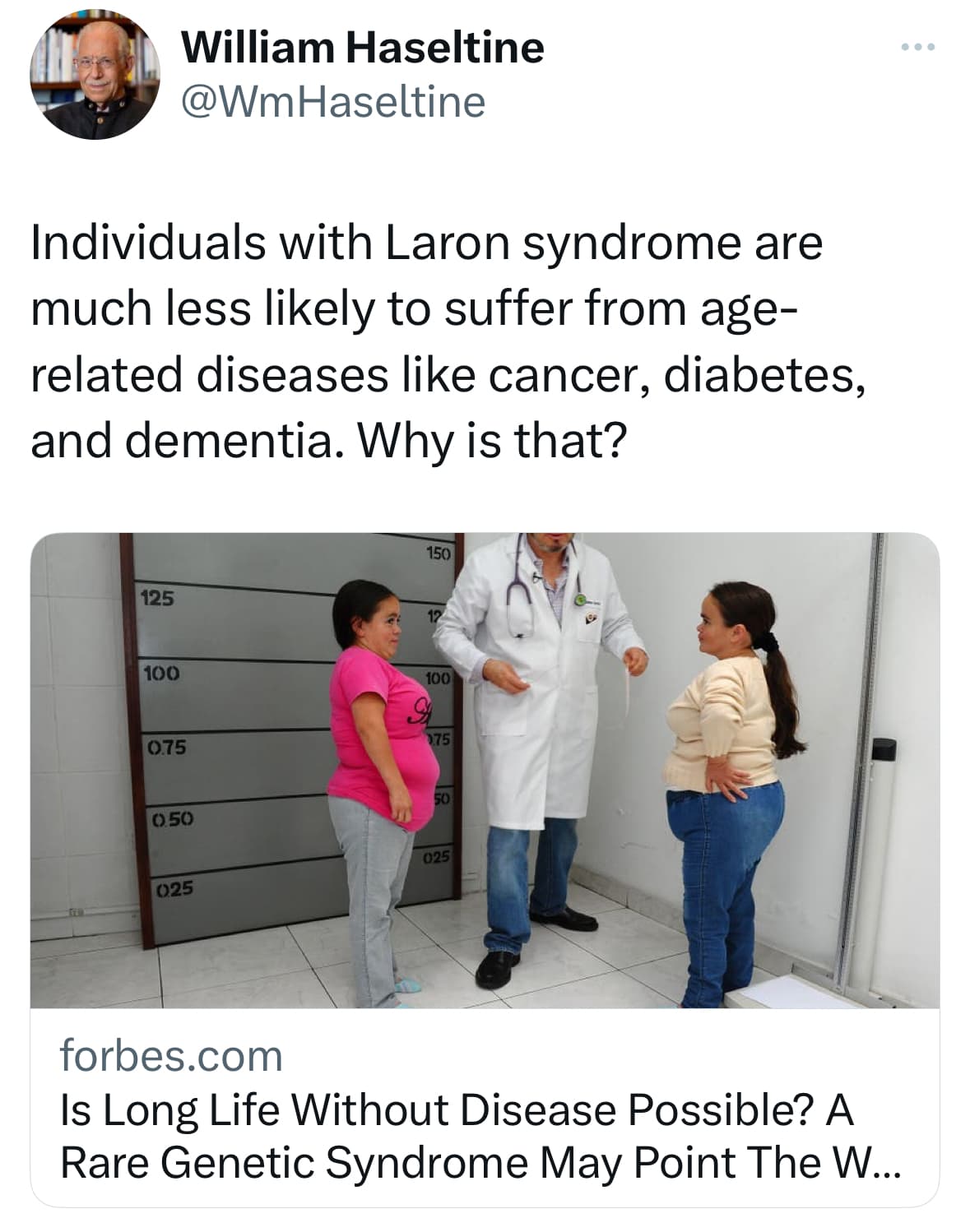
Yes - hyper function theory of aging, and antagonistic pleiotropy all wrapped up in one ![]()
Hyperfunction theory of Aging:
https://www.aging-us.com/article/203937/t
After taking rapamycin for a couple of years, I am on a 2 month break that probably ends in March. Before I restart, I’ll report on my IGF-1 as a baseline and get it remeasured three months after that. Any problems with allowing 3 months to establish a possible change in results?
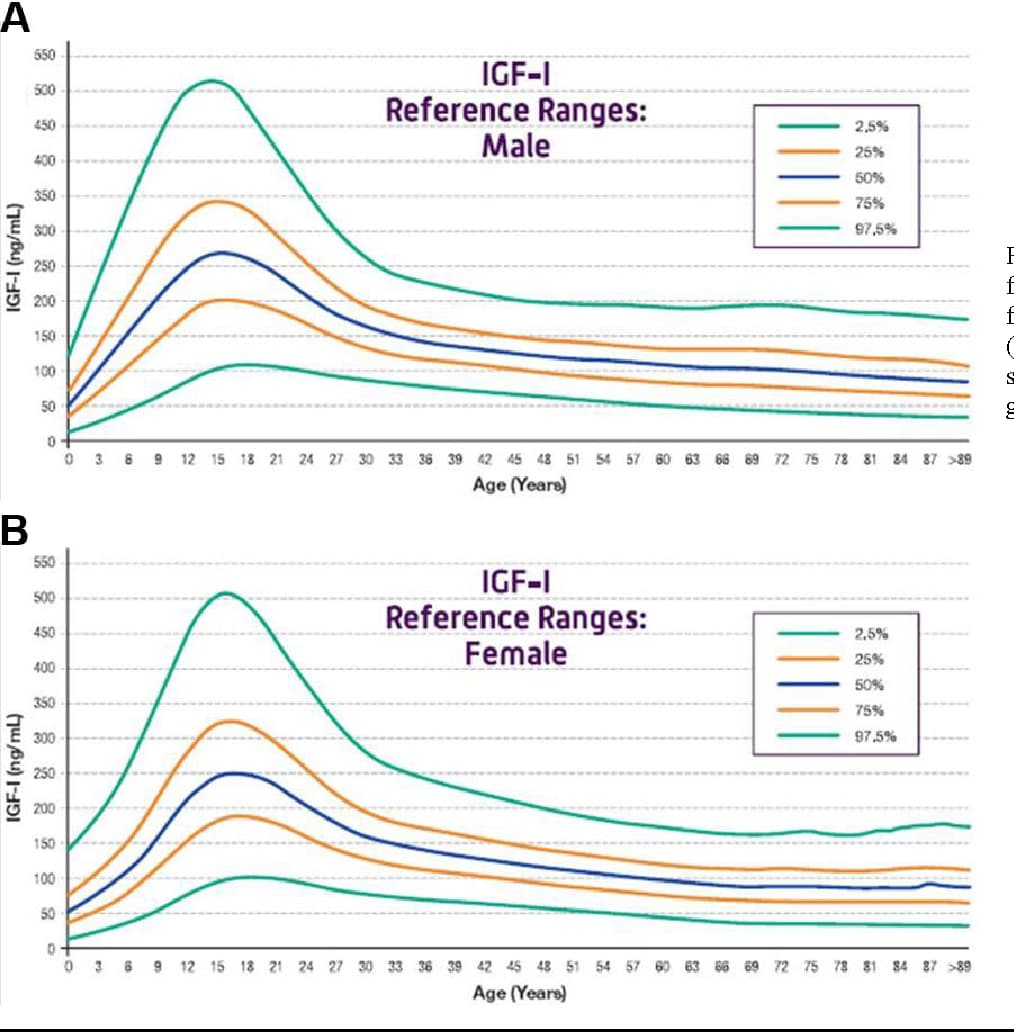
My test results, after a 2 month layoff of rapamycin, followed by 4mg rapamycin with 10oz grapefruit on a Friday, then the IGF-1 test on Monday: 74ng/mL (reference: 68-247). I’m in the 25th percentile as a 60yo male, which sounds good to me for longevity purposes. I’ll test again after a couple of months of intermittent rapamycin.
According to this:
THE HYPOTHALAMUS AND PITUITARY PART II
plasma half-life of IGF, which is around 12 h
so perhaps at least part of my lower-but-normal IGF-1 is due to the rapamycin 3 days earlier.
New Open Access Paper Reduced insulin/IGF-1 signalling upregulates two anti-viral immune pathways, decreases viral load and increases survival under viral infection in C. elegans by Elizabeth M. L. Duxbury & AlexeiMaklakov et al.
I got my IGF-1 tested for the first time (thanks @Neo, for suggesting it): 40.3 ng/mL, so very low ![]()
I’m struggling to understand whether this is good or bad…
Yeah. It’s like free testosterone levels…. low might be best for longevity, medium might be better for (current) healthspan
… my personal goal is to maximize longevity while keeping current health status good, so rather lower than higher on IGF-1…., but seems tough to triangulate in on what exactly is optimal from the different data types that we currently have
Perhaps look into what things could be negative and make sure you don’t see any symptoms related to those.
Any idea why it might be low? I haven’t looked into it, but perhaps SGLTi nudges it down?
No idea. SGTLi don’t seem to have an effect on IGF-1. Weird: ARBs might increase it: AT1 receptor blockers increase insulin-like growth factor-I production by stimulating sensory neurons in spontaneously hypertensive rats 2009 (not sure if it’s a good paper).
Symptoms are very non-specific: https://www.testing.com/tests/insulin-growth-factor-1-igf-1/
In adults, abnormally low levels of GH and/or IGF-1 may cause subtle, nonspecific symptoms such as:
Decreased bone density
Fatigue
Adverse lipid changes
Reduced exercise tolerance
Depression
Thinning, dry skin
Curious, do you have any update on this?
What is the range of your test? (Your level seems just outside of the edge of the “normal” range from Quest Labs)
I’m not sure if you saw my posted results above. I’m not planning to do another test any time soon.
@EnrQay Sorry. Don’t seem to see anything after your message in Feb on having new OmegaQuant tests planned - am I missing that info somehow?
They give 79–900 ng/mL as the “normal” range. They write:
Many factors can lead to having low IGF-1 levels such as: nutritional deficiencies, disorders of the pituitary gland, aging, kidney disease, liver disease, elevated estrogen.
FWIW: Quest has 52 as lower range of “normal”
Perhaps good to include now and then in future so you can build a time series
here you go: