Never heard of this guy but apparently he has a phd and thinks it’s productive to just attack three people in the health space like this, making mostly false claims about them. I just don’t see how character assassinations like this are useful to anyone. He makes it sound like they’re on par with the liver king or something.
It’s someone trying to stand out and make a name for themselves. I can’t find any substance to his posts besides name-dropping and telling people to ‘stop wasting money on saunas and supplements.’
Well, I for one enjoy my annual sauna, so I’m not giving that up! ![]()
4 Likes
He’s right that every other exercise and health professional doesn’t advocate certain therapies as he said. That doesn’t mean it is a good thing.
Doctors usually don’t want to test anyone unless they are symptomatic, and not care about any markers that aren’t outside the reference range, for example. They suck at preventative care unless it’s right obvious in their face or makes a hit in their risk calculator. They’re good at acute cases though and things like surgery, meaning diagnosing and treating a disease. Not prevention.
So yes, he’s right but it doesn’t mean anything on its own or what he thinks it means.
6 Likes
Most doctors aren’t that great about proactively treating due to malpractice concerns and lawsuits unless it is standard care.
“You should do daily saunas to prevent XXX!” was probably never uttered by a GP.
Just look at how hard it is to get a Rapamycin prescription. ![]()
Yet, there are still a lot of amazing doctors out there like @DrFraser @KarlT @Dr.Bart @DrM etc…
8 Likes
I just started doing a daily 30 minute sauna session. It hurts so good. It is a significant stress on my body. I love it. Thanks, Rhonda!
2 Likes
Thanks for letting me know. I didn’t know that I suck.
@KarlT Don’t worry, we all love you being here. @A_User is making broad blanket statements about the doctors not on this site, but his ire probably should just be directed at the original poster. ![]()
I meant on average of course.
3 Likes
I really enjoy my longevity medicine consults, because it is exactly this - it is a “What’s going to kill or disable you and what can we do to mitigate.”
-Vascular Disease (#1 CAD/#3 Stroke) [Lifestyle, lipids, BP, insulin sensitivity]
-Malignancy #2
-Respiratory disease (which I don’t see in many of my patients like COPD usually from smoking/exposures)
-Sarcopenia/Osteoporosis
-Trauma avoidance
-Hormone normalization for life along with metabolic health/optimal body composition
-Immunizations of value (Tetanus, Shingles, Influenza, probably pneumonia)
Once all those things are optimized then it’s time to start thinking about Rapamycin, SGLT2’s, PDE5’s etc … but taking on the high evidence stuff and doing it well, should be bread and butter primary care - it sadly isn’t, and I don’t think there are primary care doctors that sit down with their patients to have a discussion of what is going to kill or disable you, and how do we mitigate this.
@Joseph_Lavelle We will soon have a big sauna in our new house (if I can ever afford it) which will be lovely.
5 Likes
What about optimizing blood values? There’s always an optimal association lowest ACM risk for different blood values.
For example, optimal levels of ALP based on associations seems to be around 50 IU/L, and you can do this for every given biomarker:
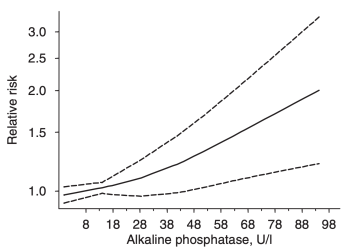
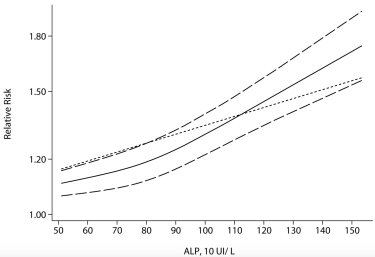
Two separate meta-analyses have investigated the association between serum levels of ALP with risk of death for all causes. First, in a meta-analysis of 4 studies that included ~9 million adults, ALP values greater than 48 IU/L were associated with a significantly increased all-cause mortality risk (Kunutsor et al. 2014):
In another meta-analysis that included 24 studies and 147,634 subjects (Li et al. 2014), lowest risk of death for all causes was identified for ALP values ~50 IU/L:
Note that mortality risk increased linearly up to 85 U/L (short dashed line, dark black line), but increased at a much greater rate for values greater than 85 U/L. In addition, the meta-analysis of Li et al. 2014 did not include the 8.9 million adults of Fulks et al. (2008), which were included in the Kunutsor meta-analysis. Nonetheless, the data from these 2 complimentary meta-analyses arrive at the same conclusion: lower ALP values may be better in terms of reducing risk of death from all causes.
Investigating further, ALP levels increase during aging from ~60-80 U/L in adults < 55y to > 80 U/L in adults > 55y (Strømme et al. 2005, Han et al. 2016), evidence that further suggests that lower may be better:
What’s in the normal reference range can many times be suboptimal according to association studies or better.
3 Likes
That is part of the process, the lab testing that is typical is:
Vitamin D, 25-OH, Total
Vitamin B12 & Folate
Thyroid Panel (TSH/FT4/FT3 if concerns thyroid antibodies)
Uric Acid
Testosterone, Free & Total w/ SHBG
Omega-3 and -6 Fatty Acids
PSA, Free and Total (men only)
Magnesium
Lipoprotein(a)
Lipid Panel
Iron + Total Iron Binding Capacity
Insulin, Fasting
IGF-1
Homocysteine
Hemoglobin A1c
GGT
Ferritin
FSH & LH
Estradiol (E2)
Comprehensive Metabolic Panel
CBC with Differential and Platelets
C-Reactive Protein, High Sensitivity (CRP, HS)
Apolipoprotein B
ApoE genotype
Yes all these things are measured and optimized - but then additional items might be relevant such as heavy metals, organics, molds, food sensitivity, microbiome … there is a lot more stuff that can be done, but it should be used sparingly and when we thing there is a problem likely to be discovered.
I’m also increasingly having people who are game to do it take the CNS Vital Signs neurocognitive testing and track this. It’s cheap and an evidence based way to track neurocognitive state in a broad way with lots of domains.
Crap I’m giving away my secret sauce … anyway, this is the construct and labs that are typical.
10 Likes
@DrFraser I wish your practice was in Michigan. I’m sure my parents would do well with you as their PCP!
2 Likes
That’s more an appeal to authority than an an hominem attack. I don’t like ad hominem attacks. I am not a fan of appeal to authority, but I don’t see it as being that bad.
1 Like
Tiller has a book out about being a sceptic in the area of sports science. It may be in his interest to raise these issues with names attached.
2 Likes
The internet is a wild ecology. Every niche will be exploited, and new niches are being invented by the second. The competition for eyeballs undermines the potential for value. I find that I cannot stand these algorithm based social media sites for long because I cannot afford the time to block enough a*holes to make the site tolerable. It’s a shame because there are many very interesting good people on X who try to be honest and helpful (and who know useful stuff).
Rapamycin news works because people here (despite being anonymous if desired) seem to feel a value in being decent human beings.
5 Likes
Just another screaming baboon. About 80% of social media is like WWF wrestling. Just a mass of people getting in these silly controversies with each other, with no real attempt at providing constructive information.
Simple test. Do you have anything to say that is based in fact and is constructive? If not, time to mute.
For myself, I retired from X awhile ago because there is just so much bile and horrible crap on it, its like crawling through a sewer to find loose change. Not worth it.
One hour on this forum is worth days on social media without the moron factor.
9 Likes