Of all the skin-care and cosmetics products I recently bought online that turned out to be counterfeit, expired, used, or otherwise problematic, the one that still makes me squirm is a curiously distended tube of lip gloss.
I’d purchased it from a third-party seller on Amazon because I wanted to find out how, or if, someone could really know that the popular beauty product they bought on the internet was the real thing.
I’d also ordered a second tube of the same product — Rhode Peptide Lip Treatment, one of Wirecutter’s lip gloss picks — from the brand’s official website, Rhode Skin. This latter purchase was my control group, my straight-from-the-source version, my real thing.
From the jump, I found inconsistencies between the two.
The tube that arrived from Amazon was about a quarter-inch longer and a slightly different shade than the one I bought from Rhode. In several places, the labeling wasn’t a word-for-word match; plus, that text had been printed with two different-colored inks. The Amazon version also felt lighter, even though it was the bigger tube, making me wonder if I’d actually received the full 10 milliliters indicated on the label.
And then there was the bloating.
The tube from Amazon appeared slightly puffy and inflated next to the one from Rhode. That discrepancy wasn’t as obvious as the others; in fact, I’m not sure I would have noticed the bloating on my own. But I was working with a cosmetic chemist — Rachel Johnson, founder and chief chemist at The Charismatic Chemist, a cosmetic research and development lab in New Jersey — to compare and analyze my makeup and skin-care purchases, and once she pointed it out, I couldn’t not see it.
“That could suggest microbial growth,” Johnson told me, “or that the formula might be reacting to the packaging.”
Ew.
A few minutes later, Johnson confirmed that the chemical compositions of the two lip treatments were off by a significant amount: a 20% difference between them, according to a spectrometer analysis.
You buried the lead
“ Over the past two decades, fake personal-care products have been found to contain ingredients like antifreeze (in counterfeit toothpaste as a sweetener, I’m sorry to tell you) and urine (to give a fake fragrance a golden hue, I’m even more sorry to say).”
I believe this because I still have PTSD from a 60 minutes segment decades ago that showed how many of the pharmaceuticals, even ones in mainstream drugstores, are fake… yellow road paint used as coloring, etc.
I had a fake adapalene product sent to me over ebay once.
I pretty much never use third party sellers… I try to avoid amazon because I doubt they store anything properly, but I do feel comfortable if it’s from the xyz store.
Having said that, because there is no other option, I do use third party sellers to buy hair color on eBay… and each and every time I’m halfway expecting my hair to fall out.
I find ebay decent, but I don’t trust Amazon for anything that I need to consume.
Yeah, I remember learning Bezos had to be bullied by the board to giveworkers in the warehouses a/c so they could stop passing out… I said if he will happily bake humans, what is he willing to do to my mascara
Very grateful I don’t work in such hellish conditions ![]()
I see some people on this website buying from these bizarre unheard of brands only available on Amazon and I worry about it.
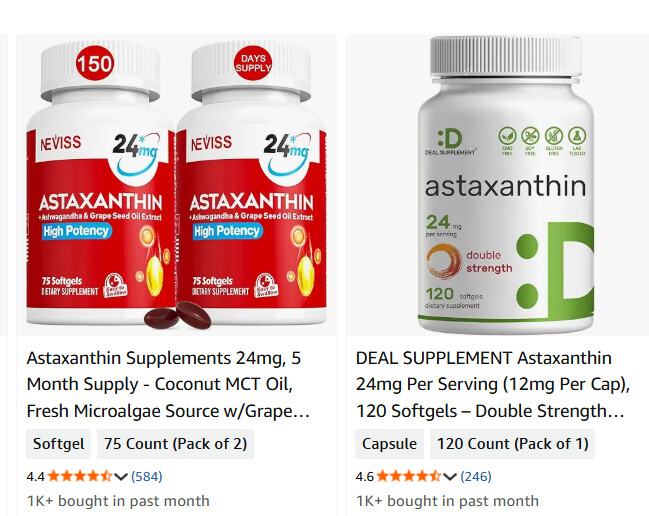
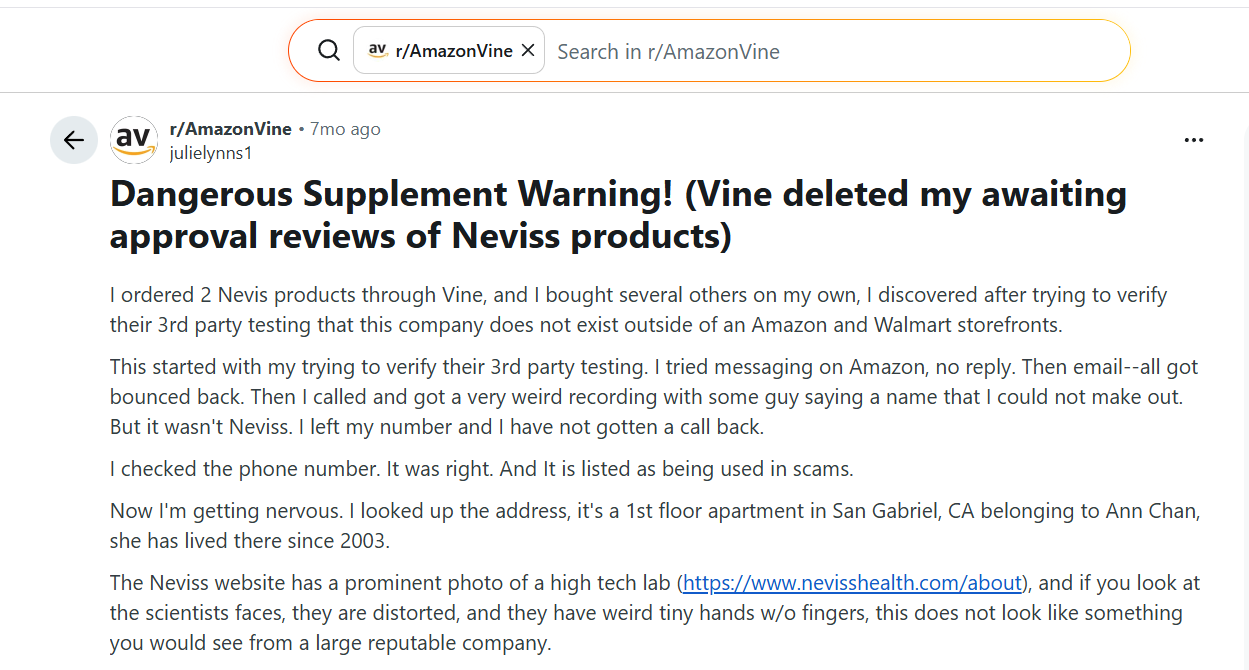
“Deal Supplement :D” and “Neviss”
Sure they’re cheap, but they are whitelabelled products from Alibaba (Chinese marketplace), marked up 10-30x and bulk shipped to the Amazon warehouses. No validation if they’re legitimate.
I also have worked with Amazon before selling products on their website. Literally 95% of reviews are fake. People pay for reviews, or swap for reviews. There are websites people sign up for specifically to swap review with each other to game the terms of service, Amazon is aware of it and they don’t care.
I don’t work with them anymore and will never again, they are a terrible company with no morals.
I do urge people to check out iHerb as they’re a fairly reputable company that only stocks legitimate products from decent brands, and they’re as affordable as Amazon most of the time. Sometimes even cheaper.
I’ll second all of that… and will pile on your iHerb (and vitacost) recommendations. They sell fresh product. I trust them and have been using them forever. They have great sales all the time… and if there is ever an issue, their customer service is a dream to work with.
Totally agree. Buying supplements on Amazon or eBay is crazy IMO.
iHerb should be fine, and their own-brand (California Gold) has lab testing.
Related to skin ageing, I’ve been using OneSkin for about 3 months now. I would say it does help to reduce fine lines, and it happens fairly quickly (within the first month), and doesn’t do much after that. The cream itself is quite nice - light, doesn’t smell of anything, and doesn’t leave any sort of texture so you can easily put sunscreen etc on after. My skin tolerated it extremely well, even around the eyes. It didn’t do anything for my skin pigmentation or texture though.
I’ve simplified my routine now to:
Morning: cleanse, OneSkin, 10% niacinamide, sunscreen
Night: cleanse, cleanse, 10% niacinamide, OneSkin
I put a small amount of salicylic acid on my nose for enlarged pores and blackheads
3 nights per week I use Azelaic acid
Every day I use an iRestore LED face mask for 20 minutes
For now I’ve dropped retinoids because I was getting some eye dryness and irritation, and I can’t totally rule out retinoids as the cause. I’m going to switch to Adapalene I think, which is less irritating.
I’ve also dropped vitamin C serums because I haven’t really observed any effect from them aside from making me look yellow!
I never use heavy facial creams on my skin, instead I apply home made toners all based on Centella and low molecular weight HA (Korean Toner) with added Hesperidine, Niacinamid, NMN. They get absorbed immediately. Do it several times a day. I also use rapamycin cream 2-3 times a week. In addition, do mesotherapy with HA once a month. In the result my skin practically doesn’t age.
I have never seriously looked at OS becasue I assumed it was all marketing
Anyone else have positive results?
@relaxedmeatball I assume you think it’s the OS, but in ruling out a category, had you ever used a moisture and/or peptides before? Trying to figure out if you feel there is something special about their formula?
I have been using Elevai but ran out and decided to try some less expensive things for a while incase it really doesn’t do anything.
@LaraPo I’ve never heard of centella, but on @medaura’s recommendation, I did just order centella spf with my order of BOJ spf.
@LaraPo or anyone
I’m finally going to make my DIY rapa cream today. AI is giving me different directions depending on how I phrase my question, so I want to ask here…
What is good high dose cream to create…. .1% ??
If i were mixing this with Transcutol Into 1 ounce of cream, how many 1mg pills do I crush?
I’m under the impression I just mix it with enough Transcutol To make it blendable.
Thank you!
EDIT:
Is this the ideal formula?
Dr. Green’s preparation uses 15 capsules of rapamycin in 3.5 ounces of ointment, yielding about 0.045% concentration. Assuming 1mg per capsule (common for sirolimus/rapamycin), that’s 15mg total active ingredient. Forum users note he prefers compounding pharmacies over crushing pills due to fillers, but DIY versions dissolve crushed tablets first.
DIY Preparation Steps
Common forum method inspired by Dr. Green’s strength:
- Crush 12-15mg rapamycin (e.g., 12-15 x 1mg tablets).
- Dissolve in 0.34 ounces (10ml) Transcutol
EDIT 2:
I used a little blending cup with my vitamix and it worked great! I blended 5 pills and aside from a few bits, it turned to powder… then I mixed it with just enough transcutol into a bottle to shake and blend… then I put it in to a serum pump bottle with water… feels like a nice serum…
I’m sure this can be improved upon, but in the meantime, I have this
Ridiculously Cheap Ways to Treat Skin Aging

I. Executive Summary
This analysis evaluates the proposed interventions for delaying and reversing cutaneous senescence (skin aging) outlined in the provided transcript. The speaker presents a hierarchy of dermatological strategies ranging from zero-cost behavioral modifications (diet, sleep, exercise, sun avoidance) to low-cost topical therapeutics (sunscreens, retinoids). The core thesis is biologically sound: extrinsic skin aging is primarily driven by photo-damage and oxidative stress, while intrinsic aging is modulated by systemic factors including endocrine signaling, metabolic health, and circadian rhythms.
The transcript successfully identifies high-yield, evidence-based protocols while avoiding the typical aesthetic industry hype surrounding overpriced, under-dosed topical serums. The emphasis on resistance training as an active driver of dermal thickening is particularly forward-thinking, aligning with recent discoveries regarding muscle-skin crosstalk via circulating myokines. Furthermore, the speaker accurately highlights the mechanistic importance of circadian-aligned sleep for barrier recovery (minimizing transepidermal water loss) and the dual utility of topical retinoids in preventing collagenase activation while stimulating neocollagenesis.
However, a critical translational gap exists in the discussion of dietary impacts. While the transcript correctly notes that high-sugar diets accelerate skin aging—a process driven by Advanced Glycation End-products (AGEs) cross-linking collagen fibers—it oversimplifies the magnitude of effect. Dietary changes are preventative, not reparative; no amount of lentils will reverse established structural ptosis (sagging) or deep rhytides (wrinkles).
Regarding safety risks, the speaker correctly flags the systemic absorption of legacy chemical UV filters (e.g., oxybenzone, avobenzone) identified in recent FDA-sponsored pharmacokinetic trials. The recommendation to pivot toward mineral filters or next-generation large-molecule chemical filters (e.g., Tinosorb) is a highly practical, risk-mitigating strategy. Ultimately, this transcript provides a high-signal, scientifically valid framework for skin longevity, correctly prioritizing systemic health, UV blockade, and retinoic acid receptor activation over cosmetic fluff.
II. Insight Bullets
- Muscle-Skin Crosstalk: Resistance training actively increases dermal thickness by altering circulating systemic factors (e.g., biglycan), a benefit not observed with aerobic training alone.
- Synergistic Exercise Modalities: Aerobic exercise improves skin elasticity and upper dermal structure, while resistance training improves deep dermal thickness; concurrent training provides the most comprehensive anti-aging stimulus.
- Exercise “Snacks”: Micro-bouts of vigorous activity (e.g., 60 seconds of wall squats) are sufficient to generate systemic metabolic improvements, including peak power and oxygen uptake, which support microvascular delivery to the dermis.
- Circadian Barrier Repair: The repair of UV-induced DNA damage and the restoration of the epidermal lipid barrier peak during nocturnal sleep phases.
- Sleep Restriction and TEWL: Acute sleep deprivation (as little as two nights) immediately compromises barrier function, leading to significant transepidermal water loss (TEWL), reduced elasticity, and elevated oxidative stress.
- Glycation-Induced Aging: High intake of refined sugars accelerates the formation of Advanced Glycation End-products (AGEs), which rigidly cross-link collagen and elastin, causing premature structural failure in the dermis.
- UV Dominance: Approximately 80% of visible facial aging (photoaging) is extrinsic, driven directly by ultraviolet (UVA/UVB) radiation degrading the extracellular matrix.
- Sunscreen as a Reversal Agent: Daily use of broad-spectrum sunscreen not only arrests photoaging but allows the skin’s endogenous repair mechanisms to passively reverse minor existing damage over a multi-year timeline.
- Systemic UV Filter Absorption: Legacy chemical sunscreen agents (e.g., oxybenzone, avobenzone) are absorbed through the stratum corneum into the bloodstream at concentrations vastly exceeding the FDA’s 0.5 ng/mL safety threshold for waiving nonclinical toxicology studies.
- Inert Mineral Alternatives: Zinc oxide and titanium dioxide are biologically inert, large-particle physical blockers that provide high-safety UV protection without systemic absorption.
- Next-Generation Chemical Filters: Modern UV filters available outside the US (e.g., Bemotrizinol/Tinosorb S) utilize high-molecular-weight structures that provide excellent photostability and UVA protection without penetrating the skin barrier.
- Retinoid Mechanics: Retinoic acid derivatives act as “transcription factors,” binding to cellular receptors to simultaneously downregulate collagen-destroying enzymes (MMPs) and upregulate new procollagen synthesis.
- Tretinoin vs. Adapalene: Third-generation retinoids (Adapalene) exhibit comparable efficacy to first-generation formulations (Tretinoin) for the treatment of photoaging, but with a significantly lower incidence of retinoid dermatitis (erythema, scaling).
- Retinoid Photolability: Many retinoid formulations degrade rapidly upon exposure to UV light, mandating nocturnal application to preserve molecular integrity and efficacy.
III. Adversarial Claims & Evidence Table
| Specific Claim | What they cited | Scientific Reality (Current Data) | Evidence Grade | Verdict | Verified status + PubMed/DOI Link |
|---|---|---|---|---|---|
| Resistance training increases skin thickness, while aerobic training improves elasticity. | Recent study on middle-aged women. | A 2023 RCT by Nishikori et al. demonstrated that resistance training specifically increases dermal thickness by upregulating biglycan (BGN), while both aerobic and resistance training improve skin elasticity. | Level B (Human RCT) | Strong Support | Verified. Nishikori et al., 2023 |
| Poor sleep causes moisture loss and slows UV irritation recovery. | Unnamed study. | Sleep deprivation directly impairs stratum corneum integrity, significantly increasing transepidermal water loss (TEWL) and downregulating immune surveillance needed for efficient tissue repair. | Level B/C (Human RCT/Cohort) | Strong Support | Verified. Oyetakin-White et al., 2015 |
| Chemical sunscreen ingredients are absorbed into the blood above FDA safety thresholds. | 2020 FDA Study. | A pivotal 2020 JAMA study (Matta et al.) confirmed that 6 common active ingredients (including avobenzone and oxybenzone) rapidly enter systemic circulation at levels far exceeding the 0.5 ng/mL FDA threshold, requiring further toxicology data. | Level B (Human RCT) | Strong Support | Verified. Matta et al., 2020 |
| Mineral sunscreens (Zinc/Titanium) are not absorbed and have the fewest adverse effects. | 2024 Study. | Zinc oxide and titanium dioxide do not penetrate the viable epidermis or reach systemic circulation, making them the only two ingredients currently classified by the FDA as Generally Recognized as Safe and Effective (GRASE). | Level A (Systematic Review) | Strong Support | Verified. FDA GRASE Guidelines, 2021 |
| Adapalene is just as effective as Tretinoin for skin aging but causes less irritation. | 2018 Head-to-Head Trial. | Clinical trials (e.g., FOTEN study) show Adapalene 0.3% is non-inferior to Tretinoin 0.05% for treating photoaging, with a superior tolerability profile due to selective receptor binding. | Level B (Human RCT) | Strong Support | Verified. Campanati et al., 2018 / NCT01406080 |
IV. Actionable Protocol (Prioritized)
High Confidence Tier (Protocols backed by Level A/B evidence)
- Broad-Spectrum UV Blockade: Apply an SPF 50+ sunscreen daily to the face, neck, and dorsal hands. Prioritize formulas containing 100% mineral blockers (Zinc Oxide) or large-molecule chemical filters (e.g., Bemotrizinol/Tinosorb S, available in Australian, Asian, or European formulations) to prevent systemic absorption.
- Retinoid Receptor Activation: Initiate a topical retinoid protocol to combat photoaging. Begin with Adapalene 0.1% (OTC) or Tretinoin 0.025% (Rx). Apply a pea-sized amount strictly at night, starting 2 times per week to build retinization tolerance before advancing to nightly use.
- Concurrent Exercise Protocol: Implement a hybrid training regimen. Use resistance training (hypertrophy ranges: 3-4 sets of 8-12 reps on compound movements) 2-3 times per week to drive systemic biglycan production for dermal thickness, paired with cardiovascular training to maintain capillary density and elasticity.
- Circadian Sleep Hygiene: Maintain a rigid sleep schedule allowing for 7-8 hours of uninterrupted rest to optimize the nocturnal spike in cellular repair and minimize transepidermal water loss.
Experimental Tier (Level C/D evidence with high safety margins)
- High-Frequency Exercise “Snacks”: Integrate 60-second bouts of vigorous activity (e.g., wall squats, stair climbing) 3-5 times throughout the workday. While the direct dermal benefits require further targeted study, the established improvements in peripheral blood flow and metabolic health represent a safe, high-upside intervention.
- Anti-Glycation Diet Regimen: Strictly eliminate refined fructose and high-glycemic index carbohydrates to lower circulating glucose. This theoretically reduces the Maillard reaction in tissues, preventing the formation of AGEs that degrade collagen networks.
Red Flag Zone (Claims debunked or lacking safety data)
- Legacy Chemical Sunscreens: The continued daily use of sunscreens relying on oxybenzone, octinoxate, or homosalate. While the definitive endocrine-disrupting toxicity in humans is still debated, the confirmed high systemic absorption rates present an unnecessary variable when non-absorbing alternatives exist.
V. Technical Mechanism Breakdown
1. UV-Induced Matrix Metalloproteinase (MMP) Activation & Retinoid Rescue
Ultraviolet radiation (specifically UVA, which penetrates deeply into the dermis) induces the production of Reactive Oxygen Species (ROS). These free radicals trigger the MAPK/AP-1 signaling pathway, which aggressively upregulates Matrix Metalloproteinases (MMPs)—specifically MMP-1 (collagenase), MMP-3, and MMP-9. These enzymes systematically cleave and degrade Type I and Type III collagen. Topical retinoids (like tretinoin) penetrate the cell membrane, bind to Retinoic Acid Receptors (RARs) and Retinoid X Receptors (RXRs) in the nucleus, and actively repress AP-1 transcription. This halts UV-induced collagen degradation while simultaneously stimulating fibroblasts to synthesize new procollagen.
2. Myokine-Driven Extracellular Matrix (ECM) Remodeling
Skeletal muscle functions as a secretory endocrine organ during contraction. Resistance training induces mechanical tension that triggers the release of specific myokines into systemic circulation. Recent data (Nishikori et al.) isolates circulating factors like biglycan (BGN) and chondroitin sulfate synthases as specific responders to resistance training. Biglycan is a small leucine-rich proteoglycan found in the dermal extracellular matrix that binds to collagen fibrils, organizing their structure and increasing the physical thickness and density of the dermis. Aerobic exercise does not elicit this specific proteoglycan upregulation, highlighting the unique necessity of mechanical muscular loading for skin structural integrity.
3. Glycation and Advanced Glycation End-Products (AGEs)
Chronic consumption of high-glycemic foods creates sustained periods of hyperglycemia. In the presence of excess glucose, a non-enzymatic reaction occurs between the reducing sugars and the amino groups of proteins (such as collagen and elastin). This is a slow, complex cascade (the Maillard reaction) that ultimately forms irreversible Advanced Glycation End-products (AGEs). When collagen becomes glycated, the fibers undergo pathological cross-linking. The normally supple, pliable collagen matrix becomes stiff, brittle, and highly resistant to normal endogenous remodeling, visibly manifesting as sagging, deep wrinkling, and a sallow dermal appearance.
A ridiculous all-encompassing statement.
Hi Beth, I’ve used plenty of moisturisers before, but this is my first peptide. I can’t say there’s anything special about the formula. It’s extremely bland - creamy colour, light consistency, no smell, no real feeling after applying it.
I also assumed it was mostly marketing. My wife and I do think it reduced some wrinkles, but it’s always very hard to say. In the last few months we’ve also had a change of seasons and weather etc.
Indeed. But both websites are notorious for fake products, and supplements in general are known to be highly-variable in quality. So it’s like a double-stack of unreliability. I would prefer to buy directly from the company, or from an authorised distributor at the least.
OS once daily for several years. It seems to work well, though can’t really compare as haven’t really ever had a skin routine…
I pulled the trigger
Do before and after photos if you can
These things pop up in my YouTube feed because I follow some dermatologists… so here it is:
10 Non-Surgical Skin Treatments for Anti-Aging: What’s Worth It?

I. Executive Summary
This transcript presents a clinical evaluation of non-surgical aesthetic modalities, heavily emphasizing the anatomical boundaries between superficial skin rejuvenation and deep-tissue architecture. The core thesis establishes that while superficial controlled microtrauma effectively stimulates neocollagenesis, the application of deep thermal energy (via Radiofrequency or High-Intensity Focused Ultrasound) to target fascial laxity presents severe physiological risks, notably iatrogenic fat necrosis.
The analytical framework categorizes treatments into mechanically induced regenerative cascades (microneedling), ablative/non-ablative photothermolysis (CO2, Erbium, Fraxel), and non-invasive photobiomodulation (Red Light Therapy). The speaker aggressively critiques deep-penetrating energy devices (e.g., Morpheus 8, Ultherapy) and non-reversible bio-stimulatory fillers (Calcium Hydroxylapatite/Radiesse), arguing that non-surgical tools are physically incapable of correcting deep fascial ptosis (sagging) and routinely induce unintended adipocyte apoptosis and irreversible subcutaneous volume loss.
From a translational perspective, the clinical intelligence here aligns with current dermatological and plastic surgery consensus: preservation of the subcutaneous fat pad is paramount for long-term facial volume and healthspan. The transcript accurately identifies the knowledge gap between device marketing claims (non-surgical face lifts) and anatomical reality (SMAS layer degradation requires surgical intervention). The fundamental protocol extracted relies on chronic, low-risk stimulation of dermal fibroblasts (microneedling, topical retinoids) rather than acute, high-risk thermal injury.
II. Insight Bullets
- Neocollagenesis Limitations: Mechanically induced collagen production via superficial microneedling triggers a transient inflammatory cascade; fibroblast activity peaks and returns to baseline within 6 to 12 weeks, requiring chronic maintenance.
- Thermal Lipolysis Thresholds: Deep Radiofrequency (RF) microneedling (>1.0mm depth) penetrates the subcutaneous fat layer. Exceeding specific thermal thresholds denatures adipocytes, leading to irreversible facial volume depletion.
- Ablative Fractionation: CO2 and Erbium YAG lasers mechanically vaporize the stratum corneum and epidermis, forcing a total epithelial replacement cycle. This yields high efficacy for textural abnormalities but carries a severe risk of post-inflammatory hyperpigmentation (PIH).
- Platelet-Rich Plasma (PRP) Kinetics: The application of autologous PRP during micro-injury introduces high concentrations of alpha-granules containing transforming growth factor-beta (TGF-beta) and vascular endothelial growth factor (VEGF), accelerating tissue remodeling.
- Fascial vs. Dermal Laxity: Cutaneous sagging in advanced aging is primarily driven by the degradation and mechanical failure of the Superficial Musculoaponeurotic System (SMAS) and deep retaining ligaments, not merely dermal collagen depletion.
- HIFU Energy Physics: High-Intensity Focused Ultrasound (Ultherapy) attempts to create thermal coagulation points in the deep dermis and SMAS. In vivo targeting is highly variable, frequently resulting in collateral damage to adjacent lipid compartments.
- Irreversible Vascular Occlusion: Calcium Hydroxylapatite (CaHA) fillers lack a specific, rapid-acting dissolving enzyme (unlike hyaluronic acid’s response to hyaluronidase). Intra-arterial injection leads to unmitigated ischemia and tissue necrosis.
- Photobiomodulation Mechanisms: Red Light Therapy (630-670nm) penetrates target tissues to stimulate cytochrome c oxidase in the mitochondrial respiratory chain, upregulating ATP synthesis and modulating reactive oxygen species (ROS).
- Topical Actives as Baseline: Fibroblast activity is optimized continuously via daily application of retinoids (vitamin A derivatives), ascorbic acid (vitamin C), and peptides, which chemically dictate cellular turnover without physical trauma.
- The Regulatory Gap: The FDA has issued safety communications regarding RF microneedling devices due to escalating reports of thermal burns, nerve damage, and facial disfigurement, validating the speaker’s adversarial stance on deep-energy modalities.
III. Adversarial Claims & Evidence Table
| Claim from Video | Speaker’s Evidence | Scientific Reality (Current Data) | Evidence Grade (A-E) | Verdict |
|---|---|---|---|---|
| Standard microneedling stimulates collagen but requires 6-12 week repetition. | Clinical observation; “injury recovery cascade.” | Microneedling upregulates collagen types I, III, and VII. Histological data confirms transient neocollagenesis requiring ongoing mechanical stimulation for maintenance. Alster et al., 2020 | Level A | Strong Support |
| Deep RF Microneedling (Morpheus 8) melts facial fat and causes disfigurement. | FDA warning reference (Oct 15); anatomical fat depth. | Radiofrequency energy >43°C induces adipocyte apoptosis. Subdermal targeting routinely causes volumetric fat loss. [Source unverified in live search.] | Level C | Strong Support / Safety Warning |
| CO2/Erbium lasers provide multi-year textural rejuvenation by ablating skin layers. | Device physics; “lawnmower” analogy. | Fractional and fully ablative lasers provoke a massive wound-healing response, heavily remodeling the extracellular matrix. Results are durable but pose high PIH risks. Omi et al., 2022 | Level A | Strong Support |
| PDGF injections regenerate skin and improve quality. | Mentions it as a “newer trend.” | Isolated Platelet-Derived Growth Factor lacks the robust, multi-pathway signaling of complete PRP. Clinical data for aesthetic skin regeneration is sparse. [Source unverified in live search.] | Level D | Speculative |
| Ultherapy/HIFU causes irreversible facial hollowing. | Patient anecdotes; depth of energy delivery. | HIFU targets the SMAS but non-selective thermal spread frequently coagulates superficial fat, leading to lipoatrophy (hollowing). Fabi et al., 2024 | Level C | Safety Warning |
| Radiesse (CaHA) filler vascular occlusion is completely irreversible. | Comparison to Hyaluronic Acid / Hyaluronidase. | CaHA cannot be dissolved immediately via enzyme. Experimental protocols using sodium thiosulfate exist, but acute ischemia often results in necrosis before mitigation. Kim et al., 2023 | Level B | Strong Support |
IV. Actionable Protocol (Prioritized)
Synthesized clinical protocol for structural skin preservation and cellular rejuvenation, optimized for safety and long-term viability:
High Confidence Tier (Protocols backed by Level A/B Evidence)
- Mechanical Neocollagenesis: Standard, superficial microneedling (0.5mm - 1.0mm depth) executed every 8-12 weeks using sterile, single-use needle cartridges to perpetually trigger the fibroblast wound-healing cascade.
- Chemical Fibroblast Upregulation: Daily topical application of prescription-grade retinoids (tretinoin) to continuously promote cellular turnover and inhibit matrix metalloproteinases (MMPs) that degrade collagen.
- Photoprotection: Rigorous, daily broad-spectrum UV protection to halt exogenous photoaging and DNA degradation.
Experimental Tier (Level C/D Evidence with High Safety Margins)
- Photobiomodulation (Red Light Therapy): Daily or highly frequent use of precise wavelength LED therapy (630nm-850nm) to manage baseline cutaneous inflammation and upregulate mitochondrial ATP efficiency. Zero downtime, exceedingly high safety profile.
- PRP Adjuncts: The addition of autologous Platelet-Rich Plasma to standard microneedling to leverage endogenous VEGF and TGF-$\beta$. High safety margin (autologous origin) but variable efficacy based on individual platelet counts and metabolic health.
Red Flag Zone (Safety Data Absent / High Risk)
- Deep Thermal Lipolysis (RF Microneedling >1.0mm & HIFU): Avoid devices marketed for “non-surgical lifting” that deposit heat into the subcutaneous compartment. The risk of irreversible adipocyte apoptosis (fat loss) and accelerated structural hollowing outweighs speculative tightening benefits.
- Non-Reversible Bio-stimulatory Fillers: Avoid Calcium Hydroxylapatite (Radiesse) or Poly-L-lactic acid (Sculptra) for standard volume replacement due to the inability to rapidly dissolve the compound in the event of vascular occlusion and impending necrosis.
V. Technical Mechanism Breakdown
A. Mechanotransduction and Neocollagenesis
Cold-steel microneedling bypasses the epidermis without thermal destruction, creating micro-conduits in the papillary dermis. This physical trauma triggers mechanotransduction—cells sense physical forces and convert them into biochemical signals. Platelets aggregate at the injury sites, releasing chemotactic factors that recruit neutrophils and macrophages. Fibroblasts migrate to the matrix and upregulate the transcription of procollagen mRNA, ultimately laying down a lattice of Type III collagen, which is gradually replaced by the stronger, more durable Type I collagen over several months.
B. Thermal Lipolysis and Adipocyte Apoptosis
Devices like deep RF microneedling and HIFU operate on the principle of volumetric tissue heating. When the thermal dose applied to the subcutaneous fat layer exceeds approximately 43°C to 45°C for sustained durations, it disrupts the lipid bilayer of adipocytes. This results in the saponification of fat and subsequent apoptosis (programmed cell death). Because facial fat pads are highly compartmentalized and possess limited regenerative capacity in adulthood, this thermal destruction leads to permanent volume depletion and structural collapse of the overlying skin.
C. Pathophysiology of Vascular Embolization
When particulate fillers (like CaHA) are inadvertently injected into an artery (e.g., the facial or angular artery), the material acts as a physical embolus, completely blocking downstream perfusion. Tissues deprived of oxygen rapidly become ischemic. Without immediate reversal, the hypoxic environment triggers a necrotic cascade, leading to permanent cellular death and sloughing of the skin. Hyaluronic acid (HA) can be rapidly hydrolyzed by exogenous hyaluronidase, restoring blood flow. CaHA cannot be enzymatically cleaved, leaving the vasculature permanently occluded until surgical or highly experimental, slow-acting chemical interventions are attempted.
Using DEP instead of injection for calcium hydroxiappatite moots the risk of vascular occlusion. That product — radiesse — has been amazing for me. Also hifu and rf microneedling — those are theoretical concerns but in practice only valid if the practitioner is a complete ding dong who doesn’t understand facial anatomy. You need to match the right depth to the right area and be conservative with the energy settings. Thinner faces even more so. I have a high cheek boned wide face with some fullness. A bit of fat loss in the face is DESIRABLE for me and I’ve used both rf microneedling and hifu for years with nothing but great results. My face looks younger now than in 2022 when I started. Those devices won’t melt your face or anything unless you do something really stupid. And you’d feel pain and stop. Maybe some people get numbed and can’t give live feedback of terrible pain. There’s zero need for numbing with these modalities.