@desertshores So what does PhenoAge say about you? Just curious. I’ve never used any of those clocks.
This is the calculator that I use.
If you do not want to use the spreadsheet, you can enter your results into the age calculator. You can also download the spreadsheet from Dr. Kara Fitzgerald’s website or
Nick Engerer’s website.
This particular version is attributable to:
John G. Cramer, PhD, Professor Emeritus of Physics at the University of Washington, Seattle
These are the results from the last time I entered my test results (Unlike Michael Lustgarten, I do not update the calculator frequently). Twice a year is sufficient for my needs.):
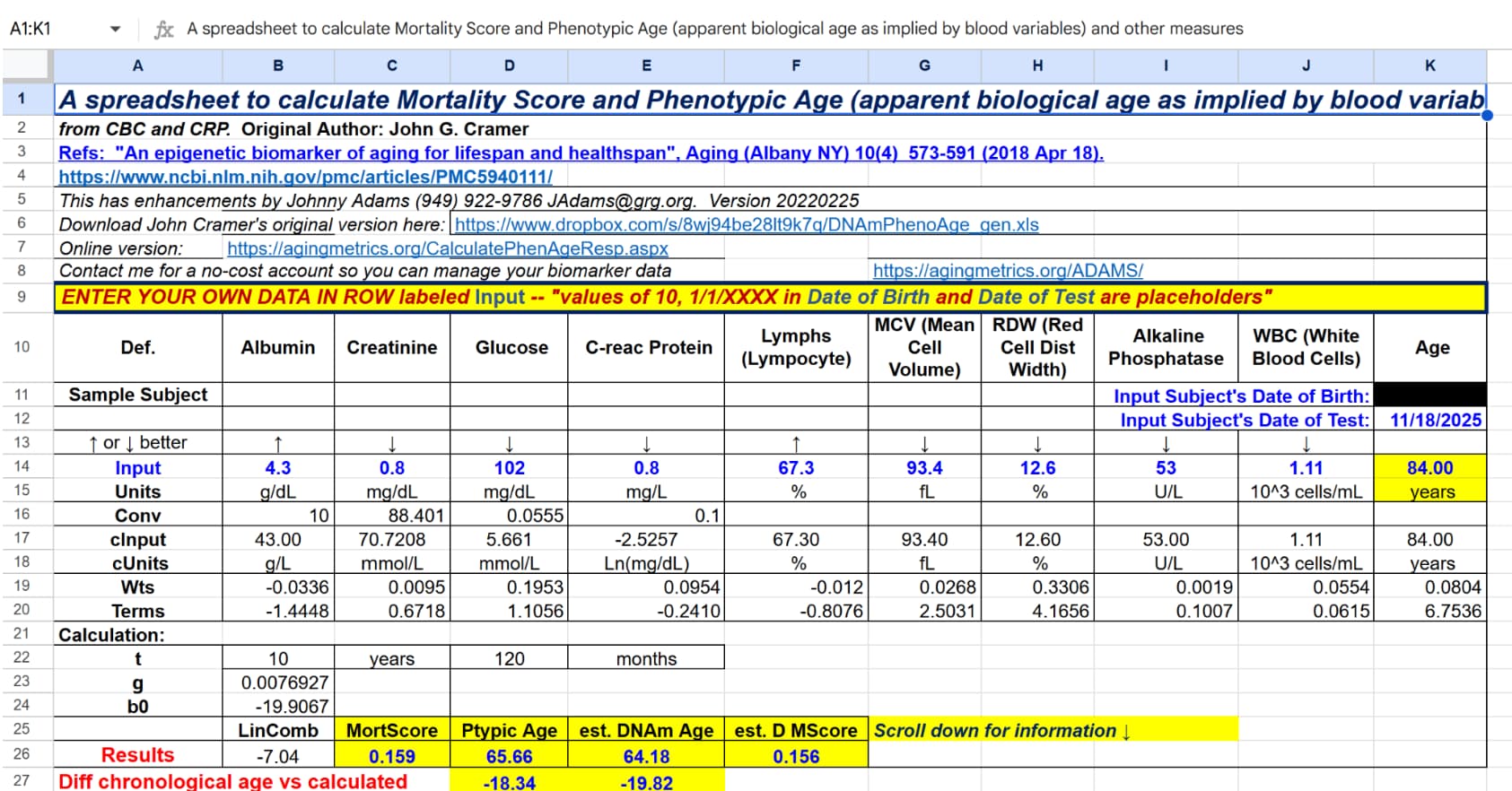
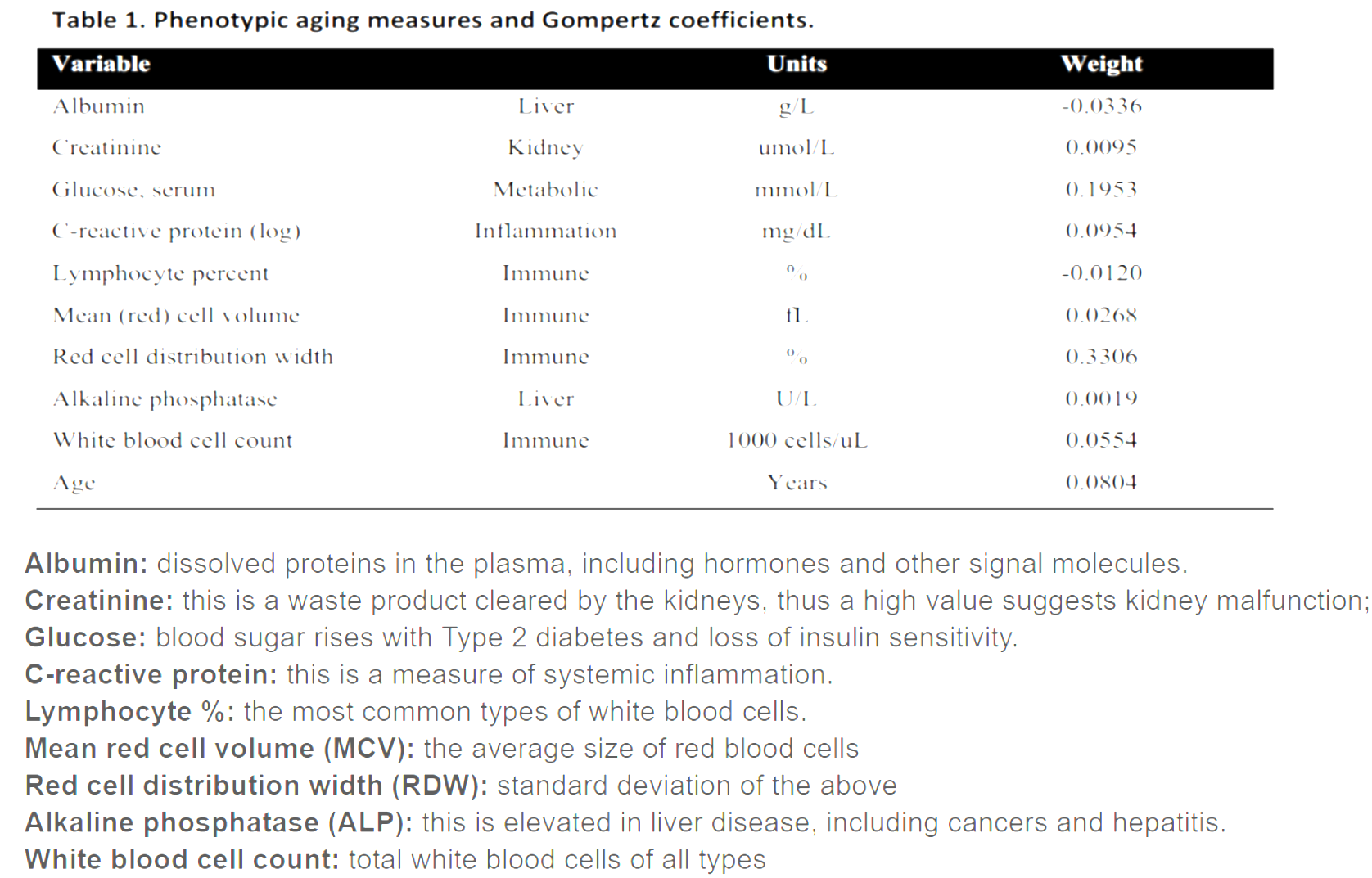
An epigenetic biomarker of aging for lifespan and healthspan
6 Likes

This report provides a clinical analysis of the dermatological protocol combining AmLactin (ammonium lactate) and topical retinoids. It synthesizes the insights from Dr. Dray’s clinical experience with peer-reviewed data on alpha-hydroxy acids (AHAs) and vitamin A derivatives.
I. Executive Summary
The combination of ammonium lactate (lactic acid) and topical retinoids represents a high-potency, non-invasive strategy for reversing photoaging and structural skin atrophy. While often overlooked due to potential irritancy, this duo utilizes a dual-mechanism approach: chemical exfoliation/humectancy and cellular receptor-mediated remodeling.
AmLactin serves as a unique AHA due to its humectant properties and its concentration-dependent biological effects. Clinical data confirms that while lower concentrations (5%) provide superficial epidermal smoothing, a 12% concentration is required to induce measurable changes in the dermis, including increased dermal thickness and firmness Smith, 1996. Lactic acid achieves this by dissolving desmosomal bonds in the stratum corneum and potentially stimulating glycosaminoglycan synthesis in deeper layers.
Topical retinoids (e.g., tretinoin, adapalene) complement this by binding to nuclear retinoic acid receptors (RARs) to normalize epidermal maturation and stimulate type I collagen production. When combined, these agents address skin aging at multiple biological levels: the AHA clarifies the surface and enhances hydration, while the retinoid rebuilds the structural matrix from within. However, this is an advanced protocol. The primary risk factor is barrier dysfunctioncaused by the compounding effects of retinization and chemical exfoliation. Success requires a staged introduction, mandatory UV protection—as AHAs significantly lower the Minimal Erythema Dose (MED)—and an “experienced user” profile to avoid irritant contact dermatitis AAD, 2024.
II. Insight Bullets
- The 12% Threshold: A 12% lactic acid concentration is the clinical minimum for stimulating dermal remodeling; 5% is limited to epidermal hydration Smith, 1996.
- Humectant Dual-Action: Unlike glycolic acid, lactic acid is a natural component of the skin’s NMF (Natural Moisturizing Factor), drawing water into the stratum corneum while exfoliating.
- Retinoid Mechanism: Retinoids do not “exfoliate” in the traditional sense; they normalize cellular behavior via receptor signaling, leading to a more compact stratum corneum and thicker dermis.
- Synergistic Architecture: The AHA addresses “top-down” (texture/dullness), while the retinoid addresses “bottom-up” (collagen/firmness).
- Photo-Sensitivity Shift: AHAs lower the skin’s MED (Minimal Erythema Dose), making the skin burn faster under UV exposure FDA, 2023.
- The “Retinization” Barrier: Beginners must complete the 3–9 week retinization phase (initial peeling/sensitivity) before adding AHAs to avoid severe inflammation.
- Collagen Preservation: Retinoids suppress the matrix metalloproteinases (MMPs) that degrade collagen following UV exposure.
- Molecular Compaction: Consistent use of this combo results in a “shredded wheat to smooth surface” transition of the stratum corneum, enhancing radiance.
- Waxing Contraindication: Due to stratum corneum thinning/compaction, facial waxing while on this protocol carries a high risk of skin lifting (tearing).
- Maintenance Frequency: After 12 months of consistent retinoid use, anti-aging benefits may be maintained with 2–3 applications per week rather than nightly.
- pH Dependency: The efficacy of Amlactin is heavily dependent on a low pH (ideally ~2.8–4.0) to maintain the free acid required for penetration.
- Pigment Clearance: The combo hastens the clearance of melanin-laden keratinocytes while the retinoid inhibits new pigment production.
- Neck and Eye Fragility: The thinner skin in these areas has fewer oil glands, making them high-risk zones for irritant contact dermatitis with this protocol.
- Layering Uncertainty: No definitive RCTs prove the superiority of simultaneous layering over alternating nights; “alternating” remains the safer clinical recommendation.
- Barrier Support: The use of niacinamide or ceramides is recommended to mitigate the “retinoid-compromised” skin barrier during this intensive treatment.
III. Actionable Protocol
High Confidence Tier (Level A/B Evidence)
- Pre-Conditioning: Establish a stable, nightly retinoid habit for at least 3 months (no active peeling or redness) before introducing AmLactin.
- Concentration Selection: Utilize 12% Ammonium Lactate (e.g., AmLactin Daily) to ensure dermal-level stimulation Smith, 1996.
- Sun Protection: Mandatory application of broad-spectrum SPF 30+ daily. AHAs increase sunburn risk by approximately 20% during and one week after use.
- Hair Removal Safety: Discontinue both actives at least 5–7 days prior to any facial waxing or laser treatments.
Experimental Tier (Safe but Unproven for Synergy)
- Alternating Schedule: Use Retinoid on Night 1, AmLactin on Night 2. This reduces the risk of additive irritation while maintaining 100% of the active dose of each.
- Split Application: Apply AmLactin in the morning (for humectancy/exfoliation) and Retinoid at night (for cellular repair). Note: This requires hyper-vigilance with morning sunscreen.
- Patch Testing: Test the combo on a small area (e.g., behind the ear or side of the jaw) for 14 days before full-face application.
Red Flag Zone (Safety Data Absent / Risk High)
- Eyelid Application: Avoid the orbital bone area. The risk of chemical blepharitis or severe dermatitis is high.
- Simultaneous Layering: Applying both at the exact same time is not clinically “wrong” but may lead to unpredictable pH changes that neutralize the retinoid or cause extreme irritation.
- Acute Inflammation: If skin is red, “raw,” or stings upon applying a simple moisturizer, discontinue both actives immediately and use only occlusives (e.g., petrolatum) until the barrier recovers.
- Aggressive Multi-Acid Use: Do not combine this protocol with other AHAs (Glycolic) or BHAs (Salicylic) simultaneously, as this causes cumulative barrier failure.
3 Likes
I had forgotten about this. I used it for several years, decades ago, and was using it as a substitute for tretinoin because my doctor wouldn’t prescribe tretinoin. It is usually, if not always, behind the counter at such places as Walmart pharmacies. You have to ask for it. No prescription required. I consider it a very good product, especially for sun-damaged skin.
2 Likes
I had tried Amlactin in the past but couldn’t stand the smell. The newest versions have the smell greatly reduced.
I expanded on the research, including Dr. Greger’s emphasis on the VATTC study risks, and got the following takeaways:
Tretinoin is, by a wide margin, the best-evidenced topical drug in dermatology for both acne and photoaging. The Griffiths NEJM 1993 collagen data, replicated in subsequent 2-year and 22-month studies, are real and clinically meaningful. For melasma in fixed triple combination, for acne, and as an adjunct to minoxidil in androgenetic alopecia, the evidence is genuinely strong. For striae rubrae, post-inflammatory hyperpigmentation, and pre-procedure priming, the evidence is moderate. For keratosis pilaris, warts, scarring, and most of the other off-label uses you’ll see on social media, evidence is thin and largely empirical. For chemoprevention of skin cancer, the largest RCT was negative.
If you’re evaluating it for yourself, four honest framing points:
1. It is a real drug with a real side-effect profile, not a cosmetic. Perhaps 1 in 7 users will quit because of irritation. Tolerability protocols (low concentration, infrequent dosing, dry skin, buffering, short-contact therapy) can significantly reduce that.
2. OTC retinaldehyde or adapalene 0.1% gel is a reasonable starting point if you want to test whether your skin tolerates retinoids before committing to a prescription, or if you want most of the benefit with fewer side effects. The Creidi 1998 head-to-head suggests retinaldehyde 0.05% can deliver tretinoin-comparable wrinkle reduction with about a third of the irritation.
3. The VATTC mortality finding deserves acknowledgment, not dismissal. Mainstream consensus is that it’s likely a statistical artifact in an elderly, comorbid, high-smoking population on extreme dosing — but it has not been mechanistically explained, and “probably nothing” is not the same as “definitely nothing.” For typical adult facial use at 0.025–0.05%, the absolute risk implied is very small. For long-term, large-surface, high-strength use in elderly smokers, the risk-benefit conversation should be explicit.
4. Visible benefit takes 3–6 months, peak benefit 12 months, and effects regress within months of stopping. This is a long-term commitment.
Tolerability and How to Minimize Irritation
About 85% of tretinoin users develop “retinoid dermatitis” (erythema, scaling, stinging, dryness) at some point; ~20% experience moderate-to-severe irritation, and ~15% discontinue treatment entirely for this reason. The phenomenon is called retinization and reflects compromised stratum corneum barrier function while the epidermis adapts. It is usually worst in weeks 2–6 and improves thereafter.
Evidence-based strategies to reduce irritation:
1. Start low and slow. Begin with 0.025% cream (cream > gel for tolerability) two or three nights per week, then increase frequency over 6–12 weeks as tolerated.
2. Apply to completely dry skin. Wait 15–20 minutes after washing — applying to damp skin meaningfully accelerates penetration and irritation.
3. Use a pea-sized amount for the whole face. More is not better.
4. Buffer with moisturizer. Either apply a bland moisturizer first (“buffering”), or moisturize ~20 minutes after the tretinoin (“sandwich method”). A Draelos Cutis 2006 RCT showed pre-treating with a barrier-supporting moisturizer containing niacinamide/panthenol/tocopheryl acetate significantly reduced retinization-related irritation without diminishing efficacy.
5. Short-contact therapy. Veraldi et al. 2013 showed that applying 0.05% tretinoin once daily for only 30 minutes and then washing it off achieved acne efficacy comparable to overnight use, with markedly less irritation (only 5.4% discontinuation for irritation versus the typical 15%).
6. Avoid same-night use of other actives that compromise the barrier — alpha-/beta-hydroxy acids, benzoyl peroxide (which also chemically degrades tretinoin if the formulation isn’t a stable microsphere), strong physical exfoliation. Niacinamide, hyaluronic acid, and ceramide products are compatible.
7. Rigorous daily SPF. Tretinoin thins the stratum corneum and is itself UV-degraded; sunscreen is non-negotiable.
Foundational Mechanism & Photoaging
Griffiths CE et al. “Restoration of collagen formation in photodamaged human skin by tretinoin.” N Engl J Med. 1993;329(8):530–535.
The landmark RCT behind the 80% collagen increase finding.
![]() Restoration of collagen formation in photodamaged human skin by tretinoin (retinoic acid) - PubMed | Full text: https://www.nejm.org/doi/full/10.1056/NEJM199308193290803
Restoration of collagen formation in photodamaged human skin by tretinoin (retinoic acid) - PubMed | Full text: https://www.nejm.org/doi/full/10.1056/NEJM199308193290803
Darlenski R et al. “Topical retinoids in the management of photodamaged skin: from theory to evidence-based practical approach.” Br J Dermatol. 2010;163(6):1157–1165.
Broad mechanism and clinical evidence review.
![]() Novel approach to gene expression profiling in Sézary syndrome - PubMed
Novel approach to gene expression profiling in Sézary syndrome - PubMed
Systematic review of tretinoin RCTs for photoaging (Yin et al., Int Wound J. 2022)
Reviews 23 RCTs confirming efficacy through 24 months.
![]() Topical tretinoin for treating photoaging: A systematic review of randomized controlled trials - PMC
Topical tretinoin for treating photoaging: A systematic review of randomized controlled trials - PMC
The VATTC Mortality Signal — Most Important Safety Reading
Weinstock MA et al. “Topical tretinoin therapy and all-cause mortality.” Arch Dermatol. 2009;145(1):18–24.
The trial that was stopped early. Read the actual conclusions — the authors themselves call causation unlikely.
![]() Topical tretinoin therapy and all-cause mortality - PubMed | ResearchGate PDF: https://www.researchgate.net/publication/23801055
Topical tretinoin therapy and all-cause mortality - PubMed | ResearchGate PDF: https://www.researchgate.net/publication/23801055
Schilling LM, Dellavalle RP. “Dealing with unanticipated mortality in a large randomized clinical trial of topical tretinoin.” Arch Dermatol. 2009;145(1):76.
The editorial response calling for transparency rather than alarm.
![]() Dealing with unanticipated mortality in a large randomized clinical trial of topical tretinoin - PubMed
Dealing with unanticipated mortality in a large randomized clinical trial of topical tretinoin - PubMed
Sangolli commentary — “Does topical tretinoin used for chemoprevention cause increased mortality?” J Cutan Aesthet Surg. 2009;2(2):101–102.
The most accessible plain-language analysis of why causation is implausible.
![]() Does Topical Tretinoin Used for Chemoprevention Cause Increased Mortality? - PMC (free full text)
Does Topical Tretinoin Used for Chemoprevention Cause Increased Mortality? - PMC (free full text)
1 Like
My microspheres Tretinion tubes are ready - I’ll start this fall to avoid summer sun exposure during the first few months of application.
Revize Micro 0.025% and 0.04% 20 gm gel tubes found for about $3.25/tube from India.
Hello,
I don’t understand why the concentration of topical rapamycin for skin (>=0.1%) is insanely higher than for scalp (2 μM ≈ 0.00018%). It is about 1,000 times difference in concentration.
I don’t see any reason why topical rapamycin shows such a huge difference depending on skin and scalp. You know that scalp is skin too.
And, I found papers showing that low concentration of rapamycin also shows skin improvements too.
rapamycin (10 μM, or 0.001%):
“This prospective, randomized, placebo-controlled, exploratory study was conducted to test the hypothesis that a topical application of rapamycin (10 μM) would decrease the number of senescent cells in the skin”
“A notable aspect of this study is the use of such a low dose of rapamycin (10 μM, or 0.001%) for topical application.”
“In summary, we present the first evidence that rapamycin treatment improves function and reduces markers of aging in human tissue.”
Topical rapamycin reduces markers of senescence and aging in human skin: an exploratory, prospective, randomized trial - PMC
rapamycin (0.003–0.015%):
" Conclusion: The application of low-dose topical rapamycin (0.003–0.015%) to the face can safely decrease the appearance of facial angiofibromas in patients with tuberous sclerosis complex."
Topical Rapamycin Therapy to Alleviate the Cutaneous Manifestations of Tuberous Sclerosis Complex | Drugs in R&D | Springer Nature Link
They show that rapamycin low-dose (10 μM(0.001%)~150 μM(0.015%)) can be effective in anti-aging in skin.
My guess is that rapamycin in high-dose (>=0.1%) has been mainly used for treatments of severe skin diseases rather than anti-aging.
In case of oral intake of rapamycin, high-dose has been used for patients of organ transplant. and low-dose is for people who want anti-aging.
In the same way, I started to think that high-dose topical treatment is for treatment of severe skin diseases, and low-dose could be for anti-aging purpose.
This issue is important to determine whether I can cut down the cost of rapamycin to make topical cream. I gave up making rapamycin cream after I saw the required amount of rapamycin pills and their cost. But, I would like to try to make it if low-dose is effective. The cost is pretty cheap to make low-dose cream.
Please let me know if you have any idea about this issue. Thanks in advance.
1 Like
I see so much going on in this thread and am genuinely curious how many people actually execute and on what? So many interventions, so little time and money in the grand scheme of things. I think anyone who isn’t doing tretinoin, sunscreen, estradiol cream, and amlactin for at least the body but trying to optimize the potency of his homemade rapamycin cream is wasting time and brain cells.
1 Like
This is a great thread for me to read because I don’t know much about skin care, and from the science I can see that sunscreen is good enough and tretinoin is the most effective treatment for aged skin.
1 Like
Yes it seems like tret, sunscreen, and a good moisturizer will get you 80 to 90 percent of the way to optimization
2 Likes
I’m not talking percentages but they’re definitely the low hanging fruit. Estradiol cream is huge after a certain age for women too. Then there’s injectables and devices. And to me it would be about pruning this list to the highest ROI items not looking for the next shiny object.
1 Like
I’m a long time tret and spf devotee.
I was occasionally using retinol on my body with acids (not daily out of laziness) and just replaced it with a touch of low dose tret mixed into a lotion.
I use a body wash with enzymes which works well to soften with no effort, but I just learned here that 12% lactic acid (or equivalent) is key to skin thickening. You could read a newspaper through my skin,even when I was young, so I’m intrigued by this. I always say if this longevity shtick works, I might outlive my skin!
After reading Relaxed Meatball’s review, I started using One Skin two months ago and adore it. Their lip mask is now my favorite thing to put on before bed. I have no idea if their cream is doing anything magical, but I love using it and my skin is very happy. I will be repurchasing.
I’ve made one batch of rapa serum but have been too lazy to make it again. Partially, it’s because I never know which things I can mix together without deactivating the active ingredients… one skin peptides, rapa, tret, acids, etc. I was all ready to buy ghk-cu powder to mix in, but once again, paralysis by analysis.
Recently, instead of washing right after applying my estradiol gel, I’ll wipe any excess on my face (thanks to the discussion here). I’m only doing part of my face so if I have any kind of result, I’ll eventually notice… not expecting anything, but ??
On some mornings I’ll put a cheap vit c on my face (Timeless) as insurance.
A few months ago I stopped using my very expensive exosome serum that contained many steps in one… my skin is no worse.
Oh, and red light therapy a few days per week… again, no idea if it’s doing anything but I enjoy it.
@medaura ha, I just saw your last comment… well, I’m turning 60 this month… when you are my age, you’ll start looking for all the shinny objects you can find :)!
3 Likes
Hahaha shiny object tip: Sculptra!
3 Likes
No kidding! My face used to be more toxic than Chernobyl, and I looked great until I realized I over did it!! I let all of it dissolve (and paid to have some of it taken out… talk about insult to injury!)
My face currently only has worn off Botox at the moment… I’m in desperate need of some volume but I’ve been procrastinating going down that rabbit hole again… the puffy face sorta creeps up on you!
How do you dissolve Hesperine effectively for topical use? Pure Hesperidin has very poor solubility in both water and oil. In its raw form, it tends to precipitate out, which can feel “gritty” or simply sit on top of the skin without penetrating.
1 Like
I dissolve it in a few drops of Tanscutol and then mix with HA toner.
1 Like
Yeah lactic acid is totally under-rated, the best one is from Korea called Anua 10+ recommended by Doctorly of youtube. It does a great job for giving you an overall polished look.

2 Likes
I need to start using lactic acid. I’ve put glycolic acid from the brand The Ordinary in a spray bottle and spray this all over my body (minus the face) 2-3x a week after I shower.
Topical estradiol and estriol cream/gel on the face for men is also fine. The amount needed to apply to the face to increase collagen production isn’t enough to throw hormone balance out for most guys. I do it occasionally. It’s alternative active to retinoids.
2 Likes
There you go. It is definitely not systemically absorbed. But I didn’t know whether men’s skin was responsive. I wouldn’t use it as an alternative to retinoids. Use them together for really good results.
1 Like