I’ve noticed a strange increase in my insulin resistance lately. My glucose spiked to 190 last night after a meal of just chickpeas + tomatoes + strawberries (I ran it off to 90 but then it went back to 132 after vegan queso + 1 cauliflower head + 3 bags of target cole slaw).
But I’ve noticed that fruit and other food just spike my glucose to 160 or 170 now (more recently), as opposed to me getting BG only up to max 145 just a few months ago. I don’t know what happened, other than me taking rapamycin over longer periods of time. Most days of the last few weeks were fine but only because I recently stripped out most fruit out of my diet.
Fasting glucose can still go down to roughly 80 (though only for short periods of time)
I’m still surprised by how high your blood glucose is spiking even with metformin. I wonder if its your dosing schedule that is the issue. If you take metformin an hour before the meal / food - Is suspect you’d see something more like my BG curve.
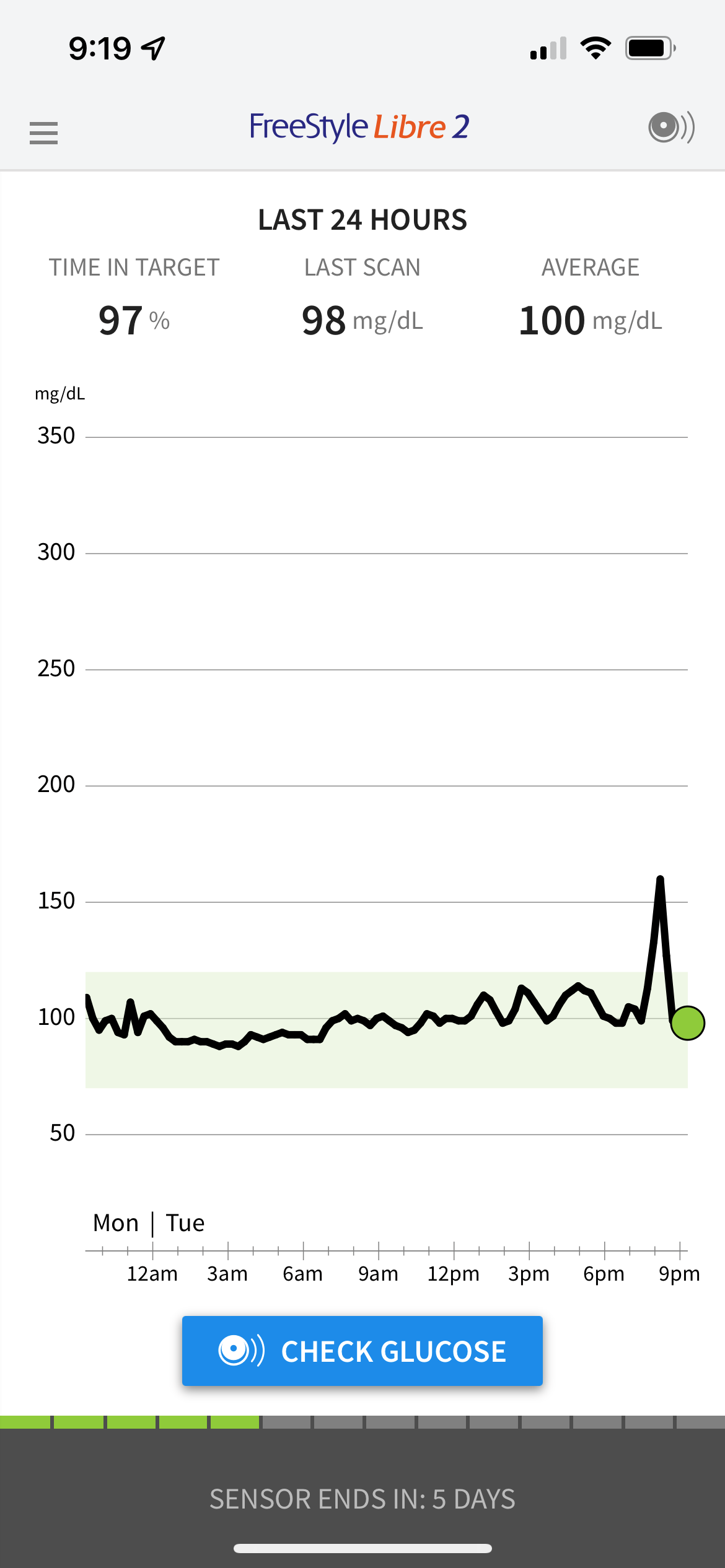
Below is what I’m seeing while taking a lower carb diet with acarbose right now (just ran out of empagliflozin) but took 10mg rapamycin on Sunday. My target range is from 70 to 120.
Alex - I was just relistening to the Peter Attia Matt Kaeberlein podcast and he covered some of the blood glucose / rapamycin issues. I recommend you listen to it too. In short, I don’t think its the rapamycin causing the blood spikes - you need to be taking it continuously at higher doses I suspect. See below…
Here are some notes that are relevant to the issue:
Dave Sabatini and Dudley Lamming’s work led to the idea that rapamycin’s side effects (especially metabolic) are caused by chronic inhibition of mTORC2
Matt thinks this is at least partially wrong
In mice, rapamycin induces a pseudo diabetes
in humans, chronic long-term treatment leads to glucose intolerance
A mouse who has taken rapamycin for a year will not clear glucose as rapidly as a mouse that never took rapamycin
Most of the data linking this effect with chronic effects on mTORC2 comes from genetic experiments with mTORC2-deficient mice
While Matt considers this a reasonable model, “I have yet to see a really clean experiment showing that that’s what accounts for the rapamycin effects on glucose tolerance”
the experiments that have been done involved genetic manipulation of mTORC1 and mTORC2 rather than experiments where mice were given rapamycin
Peter doesn’t think Rich Miller did this in any ITP studies, but he wonders whether, in studies where the animals are getting rapamycin every single day, they had impaired glucose tolerance despite longer life
Matt doesn’t think the ITP studies measured this, but he thinks some studies using the C57 black 6J mouse strain (different from the strain used in ITP studies) found changes with a glucose tolerance test on older mice at a higher dose (42 ppm)
there’s evidence in organ transplant patients for impaired glucose homeostasis as well
Matt does think it’s due to mTORC2 because there is no reason to doubt it, but he just doesn’t think there’s clean evidence yet
But he is less convinced than Dudley Lamming that these glucose homeostasis effects are bad
It might reflect is an underlying change in metabolism that could account for part of the beneficial effects of rapamycin
It could be a shift away from primarily relying on glucose as the preferred carbon source and switch over to fat metabolism (and maybe even ketogenesis to some extent)
in that context, when you challenge them with a non-physiological amount of glucose, they don’t respond the same way
Instead of a defect in glucose homeostasis, it might reflect a different underlying physiological state, but we don’t really know
rapamycin treatment has pretty profound effects on fat mobilization, fat metabolism, adipogenesis, and, at higher doses, ketogenesis
that metabolic adaptation could account for some of the beneficial effects of rapamycin and also result in the apparent aberrant response to a glucose tolerance test
Another doc who uses rapamycin liberally showed Peter some of his data that was quite dramatic (although also messy and uncontrolled)
Triglycerides fell from unhealthy levels of 200 mg/dL to 70 mg/dL
And this doc is seeing improved glucose homeostasis
When you do an oral glucose tolerance test on people who are calorie or carbohydrate restricted, you can see a physiologic insulin resistance, but that initial form of muscle insulin resistance is actually protective
However, I try to remain in keto or take acarbose+SGLT-2 inhibitors when I’m ending an extended fast. This is because I believe that these possibly benevolent insulin spikes also make me ravenously hungry and likely to overeat while breaking a fast. Without thinking too much about the implications of this, I have also adopted a similar keto or acarbose+SGLT-2 approach when I’m on rapamycin.
Even if this insulin resistance is physiological and not pre-diabetic, it would seem likely that rapamycin extends overall life span in spite of insulin resistance, which is still a bad thing if you’re eating a diet with any substantial amount of carbs; after all, we know repeated “hits” of post-meal hyperglycemia cause cumulative damage to the blood vessels and organs over time. This is why I take an SGLT2 inhibitor (to directly keep glucose down) and berberine (to decrease insulin resistance as well as for its lipid-lowering and anti-cancer properties). Hopefully I’m doing the right thing, but with combinations, who knows? I saw an interesting YouTube discussion the other day by the creators of the patented AKG supplement who said that berberine and AKG canceled each other out when they tested them together…
Good to hear we kind of have similar strategies! I do however try to avoid high amount of carbs despite sglt2 during initial days of taking rapamycin to avoid any risks of UTI (given that bacterial infections can be a bit more likely with rapamycin).
"Most studies exploring the dimensions of this paradox have been based on rapamycin treatment in mice for up to 20 wk. We sought to better understand the metabolic effects of oral rapamycin over a substantially longer period of time in HET3 mice. We observed that treatment with rapamycin for 52 wk induced diabetes in male mice, characterized by hyperglycemia, significant urine glucose levels, and severe glucose and pyruvate intolerance. Glucose intolerance occurred in male mice by 4 wk on rapamycin and could be only partially reversed with cessation of rapamycin treatment. Female mice developed moderate glucose intolerance over 1 yr of rapamycin treatment, but not diabetes. "
I have noticed, that the first 2 days or so after taking rapa, I am extremely sensitive to glucose. Having one packet of plain oatmeal (22g or carbs) spikes me 60+ points. A few days later, I am back to normal, and I actually see less of a rise in general and a flatter baseline. I am running a test this week, eating the same oatmeal every evening to see how it changes as i get further from dosing.
Here is the spike from the 22g about 10 hours post taking 6mg of rapamune. I will continue to update as more time passes.
On a practical note, my takeaway is to eat very little carbs the first 48-72 hours after taking rapa. Even assuming that its a “fake” resistance similar to coming off a long fast, I dont think its good for the body to spike this high. I have not yet tested if taking metformin will significantly blunt the rise. (that will be next weeks test).
I am currently taking 6mg of rapamune every tuesday morning together with a fat source
I think its so great that we can share our CGM results here so easily to see what our profiles are - very helpful.
In the image shown above are you taking any blood glucose reduction medicine - metformin, acarbose, SGLT2 inhibitors? Please post again on days you are (if you do try metformin).
This is supported by both the strong tendency toward smaller adipocyte diameter (P = 0.057, [Fig. 1](javascript:;),B and C) and significantly fewer adipocytes (lower DNA content per depot, [Fig. 1](javascript:;),B and C) in the rapamycin-treated group relative to control. In line with these observations, chronic rapamycin treatment increased plasma triglycerides (32%) and nonesterified fatty acids (65%) ([Table 1](javascript:;)), suggesting that adipose triglyceride deposition was impaired.
In that image i did not take anything. I wanted to isolate how my body does without anything else.
Since I started rapa two weeks ago, I have been taking
Ramaycin every tuesday morning
Metformin ER fri-sat (when i generally dont eat as well or exercise much)
Acarbose 100mg, as needed only if i want to eat a lot of carbs at once
I do my main weight lifting session on Mondays, and I wanted to be as clear of rapa and metformin as possible
Rapamycin treatment substantially impairs the initial TCR-induced upregulation of glucose transporters, glucose uptake and glycolytic enzymes in both CD4+ and CD8+ T cells (Shi et al., 2011; Finlay, 2012). Similarly, genetic ablation of Rheb (Pollizzi et al., 2015) or raptor (Yang et al., 2013) impairs the upregulation of aerobic glycolysis in TCR-stimulated T cells, whilst hyperactivation of mTORC1 in Tsc1 or Tsc2-deficient T cells is associated with enhanced glycolytic metabolism. Furthermore, mTORC1 activity is required to sustain high levels of aerobic glycolysis in effector T cells (Finlay, 2012; Hukelmann et al., 2016). In this regard, rapamycin treatment caused an approximate 50% reduction in levels of GLUT1 and GLUT3 in IL-2 maintained effector CTLs and a proportional decrease in glucose uptake and lactate production
This is really interesting info, thank you! I can’t get a CGM to stay on through BJJ sparring, so I’ve stopped wearing it. Which is why I’m very interested in other people’s readings.
Are you still seeing the glucose spikes for 48 to 72 hours? That’s longer than I expected.
I take rapa Sunday mornings and eat nothing except a bit of heavy cream in my coffee until 8PM, at which point I have a very light salad (mostly leafy greens with some olive oil). But by Monday afternoon, I go back to eating and exercising normally.
We proceeded to test the effects of two more frequent rapamycin dosing schedules, rapamycin dosed once every three (1×/3d) or five (1×/5d) days, on glucose tolerance (Fig. 1D). While rapamycin delivered 1×/3 days significantly impaired glucose tolerance, rapamycin delivered 1×/5 days had no effect on glucose tolerance (Fig. 1D), or in performance during an insulin tolerance test (Fig. S1F). All of the intermittent dosing regimens had a decreased impact on AUC compared to daily rapamycin treatment (Fig. 1E). Rapamycin treatment once every 5 days (1×/5 days) had the smallest impact on glucose tolerance, and we therefore selected this dosing schedule for further analysis.