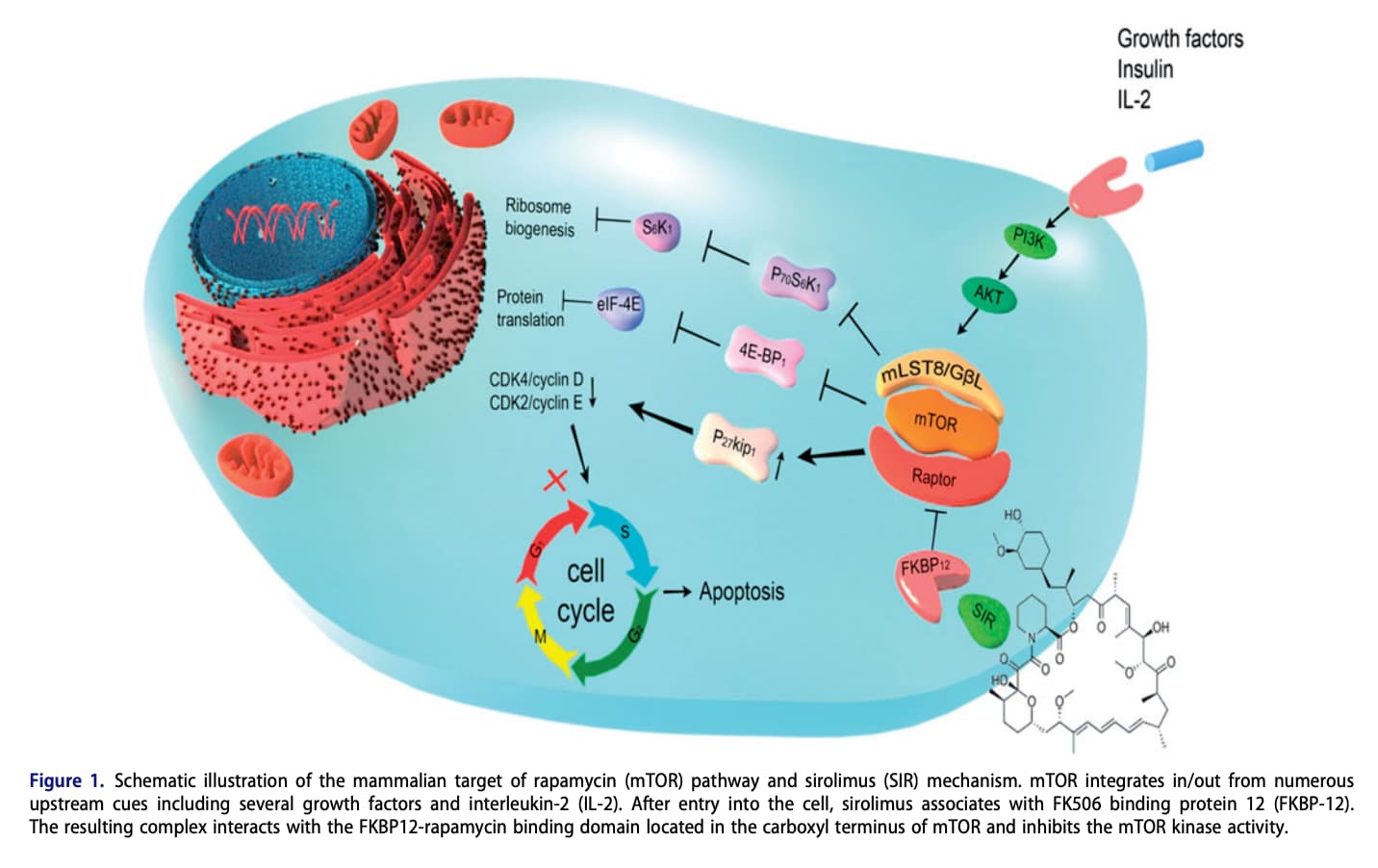
mTOR and the cascade of reduced cellular proliferation rate. It’s abundantly clear, rodents given rapamycin have reduced growth factors, which “slows” the aging process across various tissues/organs. They still die of cancer…just later. A recent study of post natal mice given rapamycin was glaringly indicative of this paradigm…growth was crushed. Middle aged mice given rapamycin undergo significant mass reduction. The rodent literature is filled with repeated confirmation of this central thesis. There are likely DOZENS of other pathways, not known, or fully elucidated/measured; infinitely complex with a myriad of genes up/down regulated, and intersecting.
I am agnostic on a singular “holy grail” pathway to longevity; I don’t believe it exists in humans, most especially translating from mice. Does slowing cellular proliferation from rapamycin teachings “influence” my approach to longevity, yes somewhat. Eating less, eating a less cellular growth stimulating diet, and fasting are direct human translation outputs for me.
I am highly skeptical on exogenous supplementation and pan cellular autophagy in humans, so I would hardly categorize exogenous as “major”…more like fanciful. I do, however, strongly believe that “some type” of extended fasting is pro-longevity. Fasting is a quasi mTOR mimetic, that is my rationale for why I think it has some very strong tangible benefits, even IF it has very little to do with autophagy per se, and acts on other pathways (lower inflammation, stronger immune system, suppression of cancer and tumor cells, lower IGF-1/glucose AUC, removal of pathogens and toxins, improved mitochondrial functioning, stem cell rejuvenation). This is low hanging fruit. Autophagy has never been measured in humans, so pure translation speculation. Last I read, we’re a decade+ away.
Agreed, why I’m agnostic to one pathway. My philosophy is very simply to hit as many pathways as practically possible in an attempt to “dampen” the aging signal, with human data most compelling.
Good points MAC, but to me fasting, while on rapamycin, especially after age 60, just seems redundant.
Melatonin works on a whole series of anti aging pathways and could be very synergistic with rapamycin. Not just a CR mimetic. Would love to see someone test the combination.
I don’t…there are way too many pathways to make a one sided best. I am not over hedging rapamycin as a panacea, take my foot off the pedal. Consider just ONE biomarker…chronic rapamycin will increase lipids and glucose, yet fasting QUASHES! You call that redundant…I call that “stack and hack”
We’re suppose to take a leap from an in-vitro study?
Why hasn’t melatonin been studied in the ITP?
A critical paper in 1995, called “Melatonin Madness,”pointed out this mistake (ME: the use of mice strains that’ don’t produce melatonin, which mice normally do not), and pointed out that in another study on a strain of mouse that does produce melatonin (C3H/He), the treated mice actually had shorter lifespans because they developed more tumors. On the other hand, there’s been additional evidence that melatonin can extend life, even in melatonin-producing animals. In C3H mice (which produce melatonin), melatonin in drinking water prolongs the life of male mice by about 20% (p < 0.01) but not female mice.[4] In CBA mice, which also produce melatonin, those given melatonin in their night-time drinking water were significantly more likely than controls to get lung cancer and lymphoma, but their lifespan still was extended by 5% relative to controls.
Hmmm, dosen’t seem too compelling to me since we’re in the rodent translation protocol.
Here’s a very interesting paper, on CR vs ad libitum fed rats, longevity, and melatonin.
Fasted (and long lived) rats had reduced melatonin through impact on pineal gland.
“When compared with 3-month-old, ad libitum fed rats, pineal N-acetyltransferase (NAT) activity had declined to less than 30% and pineal and serum levels of melatonin to 40% after 28 months when feeding had been ad libitum. It is concluded that aging in the rat (Fisher 344) is accompanied by a reduction of pineal NAT activity, thereby reducing the production of melatonin and causing a buildup of 5-HT in the pineal gland. It is furthermore proposed that food restriction, which markedly increases the life span and reduces age-related physiological deterioration and diseases in many animals, may mediate some of its effects through a SUSTAINED pineal activity in old age.”
“Several studies have shown that the aging pineal undergoes ultrastructural changes, including loss of pinealocytes which may progressively reduce the gland’s ability and capacity to produce melatonin. When food restriction was continued for the whole life span, as in the present study, it was reported that old rats had preserved a 'youthful pineal’. This observation was based on histological evidence of a profound retardation of cell loss when compared with rats that had been fed ad libitum and is in good accordance with the present demonstration of maintained
pineal function.”
And this paper suggests that exogenous melatonin may suppress endogenous production which might have theoretical potential for pineal gland atrophy.
So reduced melatonin is associated with aging…an association effect. And we think exogenous administration is going to causally increase pineal activity and increased lifespan?
If you show me the study showing this comparison, especially with dysregulation from rapa, I’m on board. Until then, I’ll hedge with some form of fasting.
This is yet again a HUMAN IMPOSED constraint…biology cares not. Don’t forget your rapamycin!
This is tricky.
Many of the HSC’s have probably also lost their Y’s but if you have Some that have retained their chromosomes then it may be possible with blood donations. Of course, it would only replace RBC’s and not the WBC’s.
I feel like I’m a stuck record on this point but everyone consistently overlooks it. You must start CR early in life to have a significant impact on longevity.
And even assuming you do I am almost certain that 2+2 < 4
True - and CR (for most of us) is really hard and greatly lowers quality of life, so I’m with you on that issue.
But - and the data isn’t really complete from what I’ve seen - it seems that fasting for 3 to 7 days may provide some benefits via autophagy that at least increases healthspan, but we have to be careful to not lose muscle.
Ah, a new research paper that seems to cover what I wanted to know in this area of autophagy:
This review will focus on the latest development of autophagy research, covering molecular mechanisms in control of autophagosome biogenesis and autophagosome-lysosome fusion, and the upstream regulatory pathways including the AMPK and MTORC1 pathways. We will also provide a systematic discussion on the implication of autophagy in various human diseases, including cancer, neurodegenerative disorders (Alzheimer disease, Parkinson disease, Huntington’s disease, and Amyotrophic lateral sclerosis), metabolic diseases (obesity and diabetes), viral infection especially SARS-Cov-2 and COVID-19, cardiovascular diseases (cardiac ischemia/reperfusion and cardiomyopathy), and aging.
Autophagy has long been considered as a double-edged sword in cancer. At the early initiation stage, autophagy acts as tumor suppressor via removal of potentially harmful cytosolic contents and damaged organelles, thereby avoiding cell injury such as DNA mutation. At the stage of progression, autophagy acts as a survival mechanism to sustain tumor viability under stressful microenvironment, which also contributes to therapeutic resistance. Therefore, in-depth understanding of the roles of autophagy during various stages of carcinogenesis and in tumor therapeutic responses will provide important therapeutic strategies to eliminate cancer cells, reverse drug resistance and prevent recurrence.
3.2 Autophagy in neurodegenerative diseases
Autophagy is essential for maintaining the homeostatic demands of neurons, both at the level of the central and peripheral nervous systems.172, 173 Based on the observations that neurodegenerative disorders occur in autophagy-defective mice, it has been hypothesized that autophagy defect is an important etiological factor for neurodegenerative diseases in humans. Pathologically, most neurodegenerative diseases are associated with accumulation of protein aggregates, including mutant α-synuclein in Parkinson disease (PD), Aβ and C-terminal fragments of the amyloid precursor protein (APP) in Alzheimer disease (AD), pathogenic mutant huntingtin (mHtt) in Huntington disease (HD), and mutant SOD1 (superoxide dismutase 1) as well as TDP-43/TARDBP (TAR DNA binding protein) in amyotrophic lateral sclerosis (ALS).172, 174 These protein aggregates are toxic drivers of neurological lesions and are supposed to be degraded by the autophagy–lysosome pathway.172 Consistently, gene mutations of autophagic receptors (e.g., SQSTM1 (sequestosome 1), OPTN (optineurin), NBR1 (neighbor of BRCA1 gene 1)) are closely associated with neurodegenerative diseases.175-177 As a result, modulating autophagy is believed to be a promising strategy for treating neurodegenerative diseases. For example, autophagy activation of the aggregating receptor SQSTM1 promotes the clearance of mHtt, insoluble tau, and Aβ42.178, 179 Conversely, inhibition of autophagy with 3-methyladenine (3-MA) results in accumulation of mHtt aggregates.180, 181 Here, we review the recent advances in understanding the pathogenesis of neurodegenerative diseases associated with defective autophagy and discuss the therapeutic interventions for these diseases via targeting autophagy.
3.3 Autophagy in metabolic diseases
Overnutrition and reduced energy expenditure, mirrored by aberrant activation of the trophic axis (e.g., insulin signaling), contribute to the development of metabolic diseases such as obesity, insulin resistance, and type 2 diabetes (T2D). Mechanistically, excess fat accumulation causes insulin resistance and elevated serum free fatty acid levels, leading to systemic lipotoxicity and β-cell dysfunction.268 In fact, autophagy responds to minimal oscillations in intracellular and extracellular metabolism, thereby maintaining a tightly regulated balance between the anabolic and catabolic pathways.269 For instance, the essential molecular players of cellular energy status, such as MTORC1 and AMPK, are involved in nutrient deprivation-induced autophagy. Autophagy performs inherent metabolic tasks in major organs such as adipose tissue, liver, and the exocrine pancreas and participates in maintaining energy balance in the body.270 As a result, dysregulated autophagic flux contributes to the pathogenesis and progression of metabolic diseases. In this section, due to space limitation, we will focus on the implications of autophagy in obesity and T2D.
MODULATION OF AUTOPHAGY AS THERAPEUTIC STRATEGY IN HUMAN DISEASES
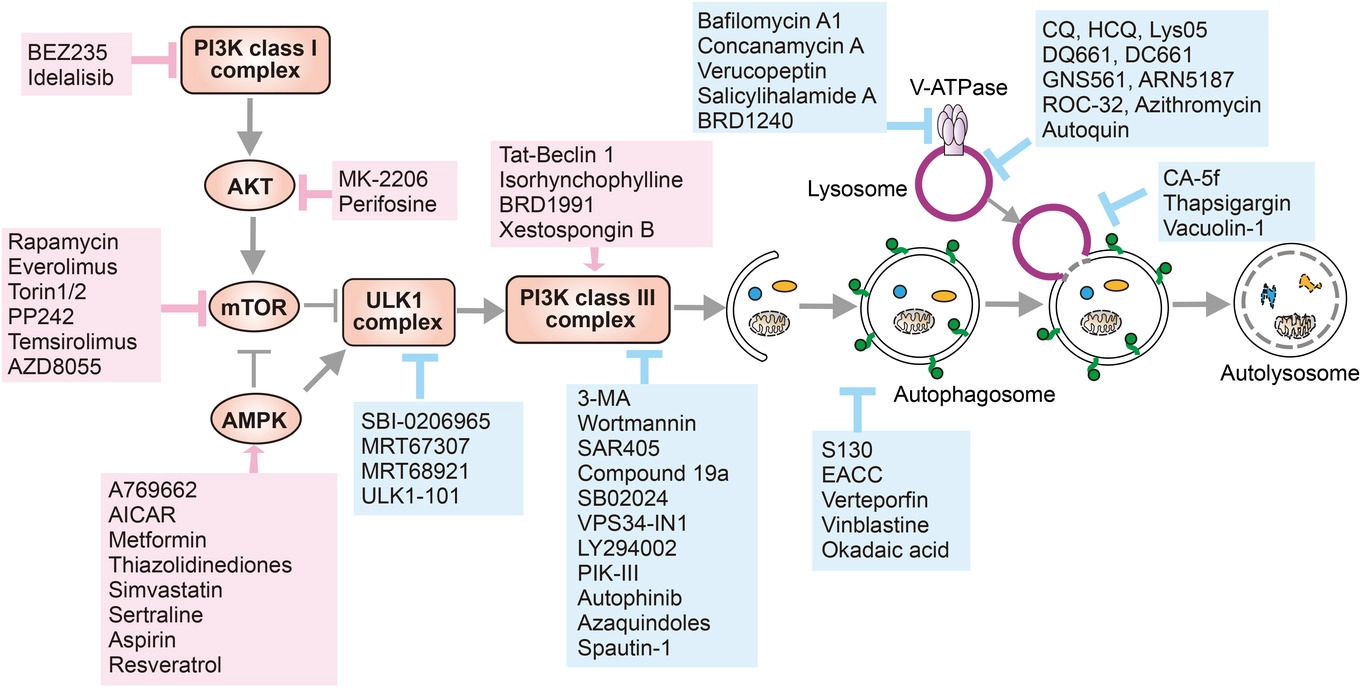
As we discussed in the previous section, approaches modulating autophagy are demanded by its important role in human health and disease. Based on the intention of different clinical applications, both autophagy activators and inhibitors have been developed and tested in the past several decades (Figure 8). Here, we reviewed and grouped the known autophagy modulators in this section.
So where does this leave us?
Is rapamycin not sufficient for autophagy?
Do we add things like melatonin and curcumin? Even add additional things?
But how do we know and what are we measuring?
I think cap-dependent and cap-independent translation of the mRNA also plays into longevity. Rapamycin, 7-alpha estradiol, acarbose, CR, fasting, and genetic longevity mutations all switch your body from cap-dependent translation to cap-independent.
I came across this on twitter - Combining sodium bicarbonate with rapamycin resulted in increased tumor necrosis, increased cancer cell apoptosis and decreased cancer cell proliferation as compared to single treatment.