Chinese paper, just published, not sure if it has any value though: EPA but not DHA improve systemic IR through activating muscle IL-6/AMPK pathway in high-fat diet-fed mice 2025
3 Likes
The last remaining argument in favor of DHA is some association studies such as this one from 2024: Circulating Docosahexaenoic Acid and Risk of All-Cause and Cause-Specific Mortality 2024
Massive association study:
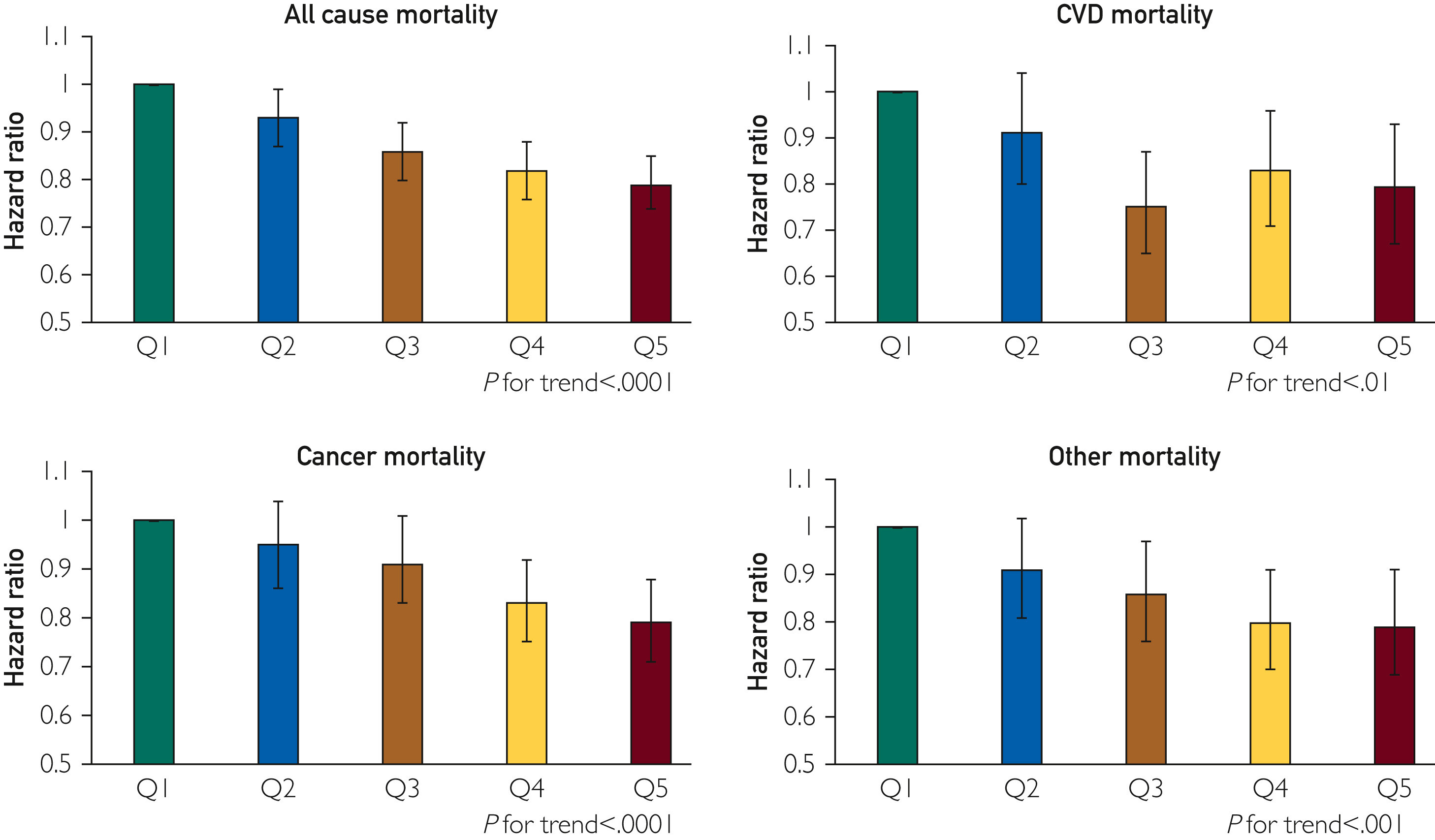
We analyzed data from UK Biobank, which included 117,702 subjects with baseline plasma DHA levels and 12.7 years of follow-up between April 2007 and December 2021. Associations with risk for mortality endpoints were analyzed categorically by quintile of DHA plasma levels.
The results look great, except for CVD mortality (more DHA is not better). The trend is also good, but Q5 is not statistically significantly better than Q3. So it looks like as long as you’re not super low (Q1), you’re good:
Digging more into the paper, they adjusted for:
Age (years), biological sex (male, female), race (white, mixed, Asian, black), marital status (living with a partner, not living with a partner, other/unknown), employment status (not employed, low activity work, high activity work, strenuous work), education (college or higher, post high school, high school, less than high school, unknown), Townsend Deprivation Index (continuous measure of relative deprivation), physical activity (very low, low, medium, high, very high), smoking status (never, former, current, unknown), alcohol intake (daily, 3-4x/week, 1-2x/week, 1-3x/month, special occasions, never, unknown), Body Mass Index ([BMI] continuous, kg/m2), prevalent dyslipidemia (yes/no), prevalent hypertension (yes/no), prevalent diabetes (yes/no), physical activity (very low, low, medium, high, unknown), self-rated health (excellent, good, fair, poor, unknown), and total circulating omega-6 polyunsaturated fatty acid (PUFA) levels (continuous, % of total fatty acids).
So, they did not adjust for income. We know that income and omega-3 intake are associated: Omega-3 Long-Chain Polyunsaturated Fatty Acids Intake by Ethnicity, Income, and Education Level in the United States: NHANES 2003–2014 2020. It is a first confounding factor. However, they adjusted for education attainment, which is correlated to income.
Other recent association studies that adjusted for income did not find benefits (or even found detrimental effects) for high-dose DHA:
They also show that serum DHA levels are highly correlated with fish oil supplementation:
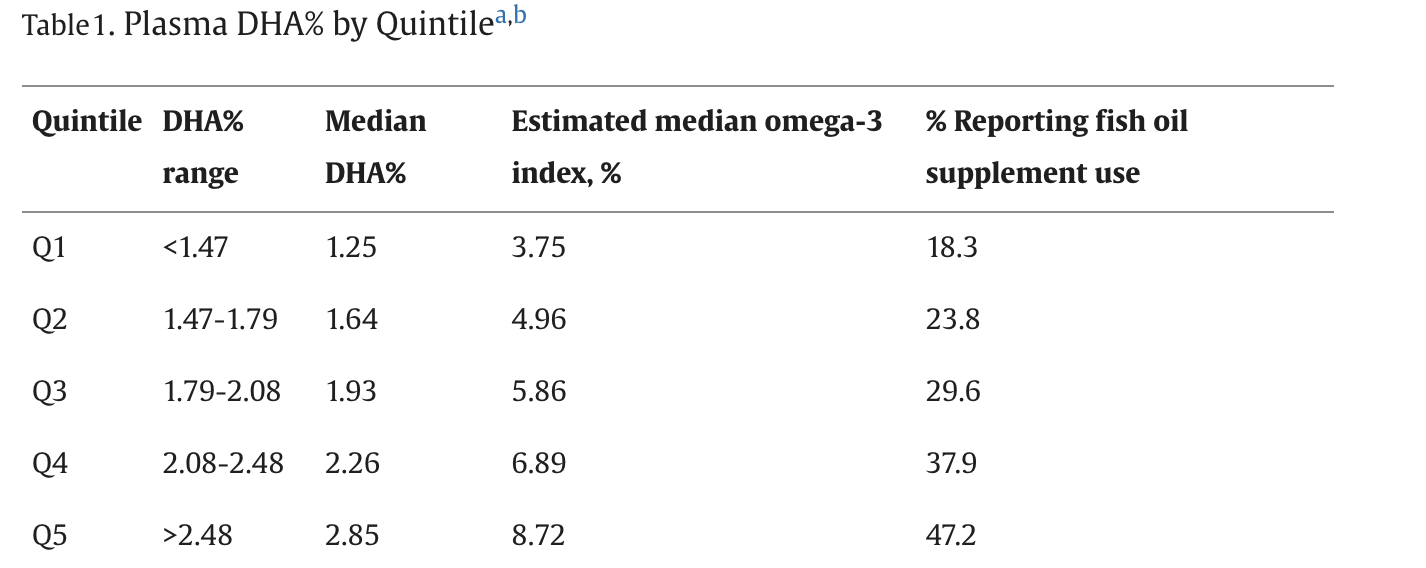
There’s a massive healthy user bias here if you don’t adjust for fish oil supplementation: people who take fish oil are likely to be more health conscious. They probably also have a better diet, they might take other supplements, they might go to the doctor more often, they might be wealthier, etc. How come they didn’t adjust for that? Or just show the results stratified by self-reported fish oil use?
I also find the ~18.3% fish oil use in Q1 surprising. It’s self-reported, so maybe these people use a low dose infrequently, but even with low-dose intermittent fish oil supplementation, I would expect most people to be at least in Q2 (omega 3 index around 5%). So maybe other factors impact DHA absorption that are not accounted for? DHA levels might therefore represent something else?
Then, they looked at DHA only. Indeed: “Blood levels of DHA but not EPA were available in ∼25% of the individuals enrolled in the UKBB.” They note:
We focused on DHA in this meta-analysis as it was the only specific omega-3 fatty acid level available in the UKBB because nuclear magnetic resonance technology was not able to reliably measure plasma EPA in this population. Blood levels of DHA but not EPA show strong statistically significant inverse associations with risk of Alzheimer disease. On the other hand, EPA monotherapy has been shown to be effective in reducing risk for major adverse CV events. No similar trials of DHA monotherapy have been undertaken. Levels of EPA+DHA have been shown to be inversely associated with mortality; however, whether EPA or DHA is more strongly associated with improved life expectancy remains uncertain.
So, even them don’t know what’s best between EPA and DHA. I guess that there’s a strong correlation between EPA and DHA levels. What if the best is actually high EPA and average DHA? We just don’t have the data here, and we cannot conclude.
To finish, there’s a risk of bias of the authors. All these association studies are always published by O’Keefe and Harris. O’Keefe is the Chief Medical Officer of Cardiotabs, a nutraceutical company selling omega 3 supplements. Harris works for OmegaQuant, which sells the Omega-3 Index test… What a surprise!
That paper (and other similar ones) is the only argument left in favor of DHA supplementation. And I think for the reasons explained above, it’s not a strong one. Especially when considering all the arguments against.
2 Likes
I’m one of the people who has switched to EPA as a result of his hard work!!! *raises hand enthusiastically
Until I hear a better idea, for now I’m going to supplement with DHA one day per week because I don’t eat fish. The thought is most of you are consuming some dha in your food, and this would help prevent me from having a deficiency.
6 Likes
Yes. I think getting rid of all DHA is a mistake. It seems to be a U-shaped curve for this one. However, EPA seems the more the better. So I’ll be increasing my EPA intake and decreasing but not eliminating DHA.
2 Likes
Just pointing out that they jury may still be out re above
There could be overadjustment bias in those last studies
And given that the current study not only adjusted for education, but ALSO for 4-5 or so other variables that are correlated to income adding income to this study could lead to overadjustment bias here.
1 Like
100 mg/day of DHA is probably enough. But you get more than that with just one portion of salmon per week. So no need to supplement.
4 Likes
Which ones?
I don’t know about overadjustment. In any case the lack of adjustment for income isn’t the worst to me. The worst is the healthy user bias and the lack of presentation of results stratified by fish oil use. What if you don’t have any significant trends anymore when you look at fish oil users only or non fish oil users only? How come they didn’t present that data?
Matt Kaerberlein’s answer:
I don’t really disagree with your position, although I don’t find the evidence against DHA to be all that convincing. Having said that, I haven’t closely read all the latest literature in this space, mostly because of time constraints and also because I get frustrated at how poorly many of these studies are designed and/or analyzed.
One of the biggest limitations to most studies in this area that I’ve seen is that they don’t actually measure omega-3’s either before or after supplementation. It’s tough to draw any conclusions - other than that population level supplementation probably doesn’t have big effects either way - in the absence of actually measuring biomarkers to see where folks started and where they ended up. If you know of good studies that did this, let me know.
Obviously, the relationship between omega-index or specific omega-3’s and health outcomes is extremely complicated and impacted by genetics and other environmental (diet, exercise, etc.) factors, likely as well as whether the source comes from diet versus supplements. Even brand of supplement may matter…
I do agree the evidence for benefit from supplementation tilts toward EPA for many outcomes, at least for now. The one I take is 3:1 EPA:DHA.
Honestly, like most supplements, I think the real answer is that supplementation is unlikely to move the needle much for most people. Especially if you are eating a crappy diet and don’t get other lifestyle factors dialed in. How much does it help if you do practice an otherwise healthy lifestyle? Hard to say, but for now it makes sense to me to get your omega-index up near the range is that most correlated with better health outcomes across populations.
I feel like he didn’t really read my email ![]() (at least he’s honest: “Having said that, I haven’t closely read all the latest literature in this space”), but he seems to directionally agree (he takes 75% EPA).
(at least he’s honest: “Having said that, I haven’t closely read all the latest literature in this space”), but he seems to directionally agree (he takes 75% EPA).
7 Likes
Actually, checking this, many studies looked at the baseline levels and it seems that, unfortunately, supplementation is worse in people with low baseline levels!
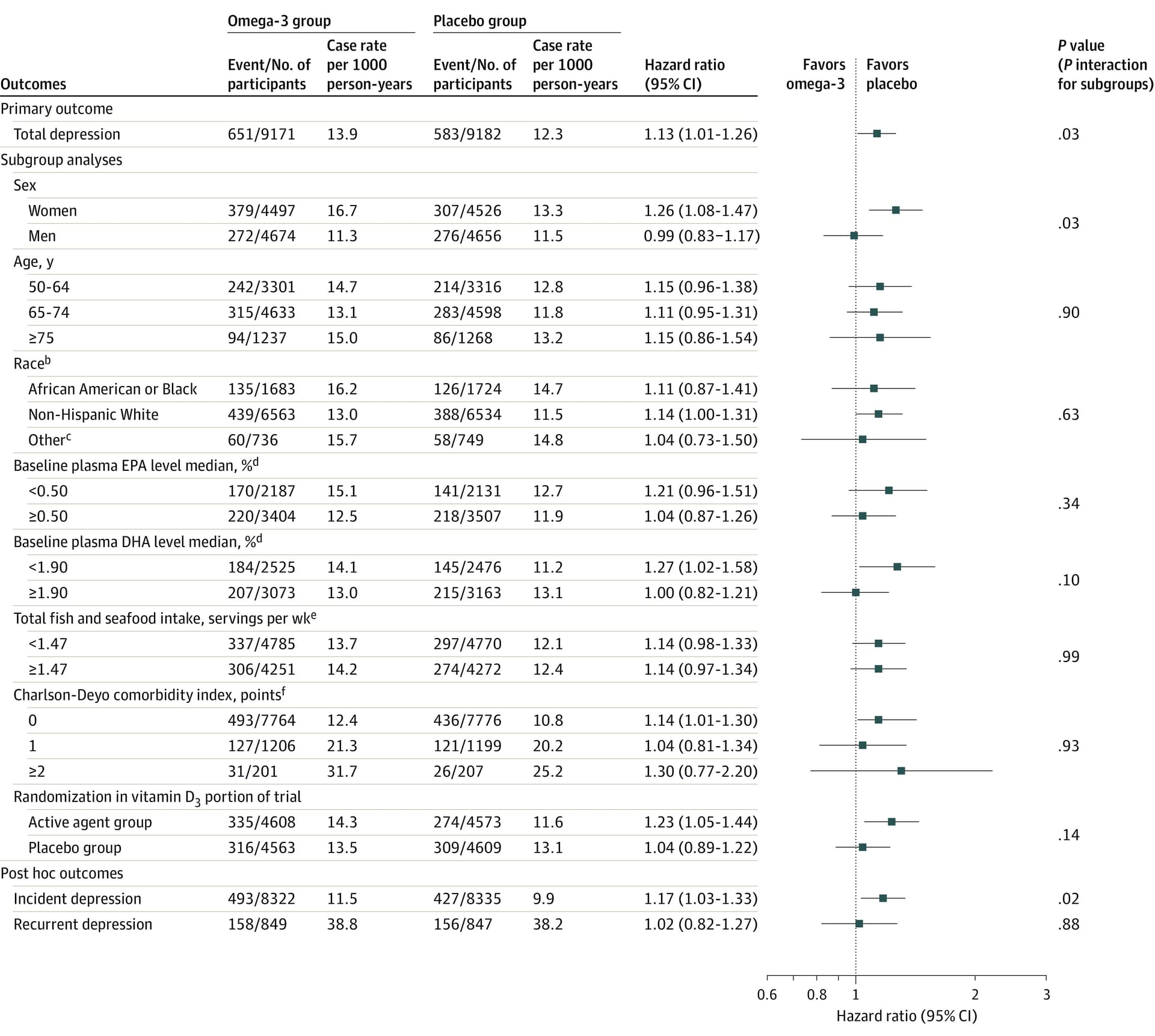
People with low omega 3 levels were worse off with supplementation!
This was also noted by @Neo regarding another study: “The best responders were those with higher (aggregate) initial levels” Omega 3 makes me depressed: why? - #80 by Neo
So it’s even worse than I thought…
3 Likes
It looks like there’s a big sex based difference? There seems little effect on men? Confidence intervals for women is completely within the favoring placebo, strong effect; for men, of course straddling neutral. The thing that’s interesting here is that if you eat fish, skip fish oil supplements.
However, it is also important to note: this is in regards to depression, depressive symptoms, mood disturbances. OK, but not everyone experiences such effects from EPA/DHA. On a population level, prevalence is relevant. And what does that mean? Does it affect brain health only in those who experience such symptoms from supplementing and those who don’t experience symptoms are unaffected?
I don’t supplement with DHA, but do modestly EPA (3x week, 500mg EPA). So I don’t know if I would get depressed if I took DHA. But if EPA supplementation also causes this effect, at least in those with low baseline levels, then it becomes a question of dosage - at what dose is this noticeable. FWIW, I don’t have any depressive symptoms or mood disturbances, and never had them. My modest EPA supplementation hasn’t changed that over the span of 2 years, which is how long I’ve supplemented. But I’m also male, so…
2 Likes
Yes, gender effect. Women absorb omega 3 more so I guess that beneficial and detrimental effects, if any, are more obvious in women: Study: omega-3 uptake higher in women; we must account for gender in research, GOED VP says
Based on other studies (MR + RCT + animal models), DHA is the cause. Not EPA.
For what it’s worth I’m a male with above average EPA and DHA levels and I get depression from (EPA + DHA) but not from EPA-only (even at 2 g/day).
5 Likes
Looking at this chart again, the most impressive thing is that there’s not a single subgroup that benefits from 1 g/day omega 3 (EPA + DHA) over 5 years. Even at this relatively low dose, supplementation was either detrimental or absolutely useless when it came to depressive symptoms.
4 Likes
Dr. Greger gives his 2 cents:
Should You Take Fish Oil

1 Like
He doesn’t mention the brain at all. It would be interesting to hear his thoughts on why he left that out, since it’s a big reason why so many people take fish oil.
2 Likes
Here’s my talk with Bill Harris, PhD of OmegaQuant about Omega 3’s. He might be biased (he sells the omega index test) and he might not know about every single omega 3 study ever completed but the guy has 40 years of scientific study in the field and 300+ published research papers. I’m inclined to trust his opinion.
Bill says:
- an omega index of 8+% is ideal, and higher omega index (EPA + DHA in red blood cell membrane) associated with lower ACM, lower mortality from CVD, cancer, and everything aside from CVD and cancer, on average). ALA does not seem to matter so it is not included in the test.
- get 1.5 grams of combined EPA and DHA (fish and supplements combined) everyday (or on a daily average taking a couple times a week); the ratio of EPA:DHA doesn’t matter as far as anyone knows
- you don’t need an expensive fish oil; the oxidation risk is a marketing ploy in his opinion
- no reliable evidence that DHA is harmful; no evidence DHA is good for the brain or better than EPA
- some omega 6’s are good for health (as good as EPA/DHA), so an omega 3:6 ratio is meaningless without knowing which omega 6’s. Just get enough EPA/DHA
- Afib risk is questionable and tiny in any case
- fatty15 is completely unproven
- SPMs are not necessary to supplement (the body makes SPMs from EPA and DHA) and the currently available SPM supplements are not SPMs but rather substrate.
And here is my own Omega Index (full version). I recommend everyone get tested and then use the calculator on the OmegaQuant website to determine EPA / DHA need to reach 8%.
Omega-3 Index 2025.pdf (3.7 MB)
7 Likes
Bill the grifter strikes again!
2 Likes
Fine to be skeptical, but lets not be cynical. Be specific in criticisms please.
2 Likes
Are you joking? I’ve spent hours researching the evidence and posting it everywhere on the forum. Especially here:
- Vitamin O (Omega 3) for athletes - #4 by adssx
- How much omega-3 do you need? - #62 by adssx
- How much omega-3 do you need? - #70 by adssx
Not a single person has denied the evidence other than gesturing “But we’ve been doing it for a long time based on association studies!”. Matt Kaeberlein “doesn’t really disagree with my position”: How much omega-3 do you need? - #69 by adssx Bill/OmegaQuant never got back to me.
The evidence on omega 3, EPA and DHA is the opposite of every single thing that Bill said (based on the list of bullet points).
His arguments are mostly based on weak association studies that he published.
He sells and promotes the omega 3 index.
He is the definition of a grifter.
Prove me wrong.
4 Likes
Yikes. Hard to trust someone who describes RCTs and MRs as not reliable.
2 Likes
The data you’ve provided is very helpful.
I haven’t listened to the podcast, and have not followed the EPA DHA thread that closely - which is likely the situation with most people. So rather than just calling someone a grifter, its helpful to explain why a person is wrong.
2 Likes