FWIW, I had this recommended to me by a doctor whom I asked:
https://www.amazon.com/Igennus-Triglyceride-Absorbable-Concentration-Sustainable/dp/B007TUK2IE/
FWIW, I had this recommended to me by a doctor whom I asked:
https://www.amazon.com/Igennus-Triglyceride-Absorbable-Concentration-Sustainable/dp/B007TUK2IE/
I saw that. It’s double the price for the same thing.
Yeah, and frankly what reason is there to think one is better than the other, I mean I’m relying on a doc’s recommendation, but what was he relying on? They swear up and down that it’s free from various toxins, independently tested and certified by IFOS, but what does that mean, and is it true; besides the GNC product also claims to be free from toxins. Probably makes sense to go for the lower price.
I’m sticking with this one despite the price, because I use so little of it that it lasts me a long time, so spread over that, I’m not hit over the head with the price difference. YMMV.
My brother got omega 3 supp from our doctor, pretty good but it said ethyl ester on the label and I told him it was way less absorbable. Pick something else next time. He asked his little AI friend who said triglyceride was 70% more absorbable.
I don’t remember who brought that up here, but good job. Otherwise you’re paying for something that won’t go in anyway. The first bottle doesn’t say the form, so you have to assume it’s the bad one.
Actually, I will have to go with the brand you recommend as GNC doesn’t ship to Hong Kong.
Just published: Dose-response association between the intake of various subtypes of polyunsaturated fatty acids and depression 2025
Chinese paper but George Institute for Global Health, so I think it’s good.
The paper concludes:
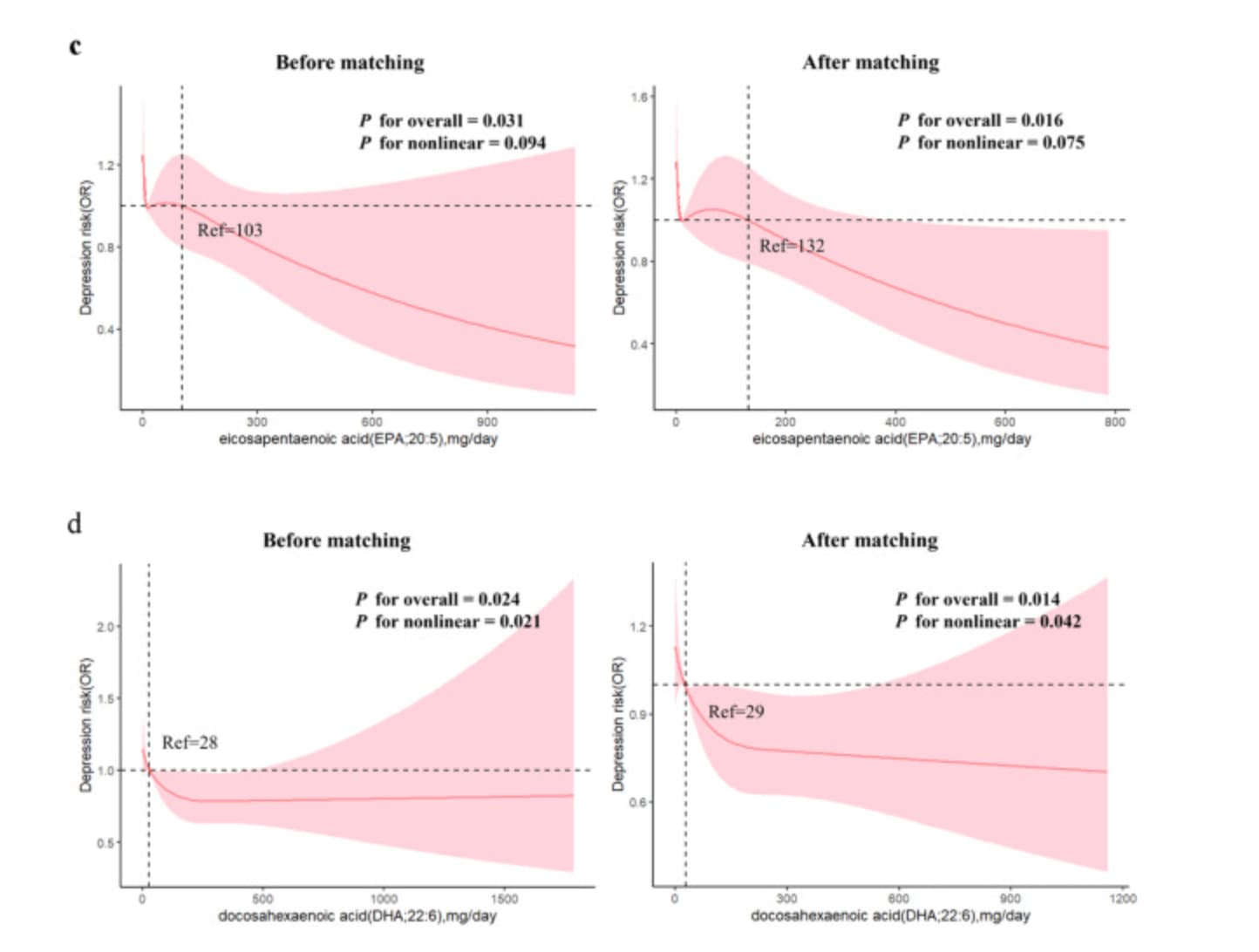
Post-propensity score matching, multivariate logistic regression analysis revealed an inverse correlation between the intake of AA, ALA, EPA, and DHA and the risk of depression. Restricted cubic spline analysis demonstrated a linear inverse relationship between AA, ALA and EPA intake and depression. Conversely, DHA intake exhibited a nonlinear relationship with depression.
Different types of PUFAs appear to influence depression risks differently in adults, with increased intake, AA, ALA, EPA and DHA providing a protective effect against depression.
However, I bought the full paper I think it’s a bit more complex for DHA:
Daily intake of n-3 and n-6 PUFAs was assessed using two 24-h dietary recall interviews, with average intake values used for analysis.
Participants were categorized into depression (cases) and non-depression (controls) groups based on their PHQ-9 scores.
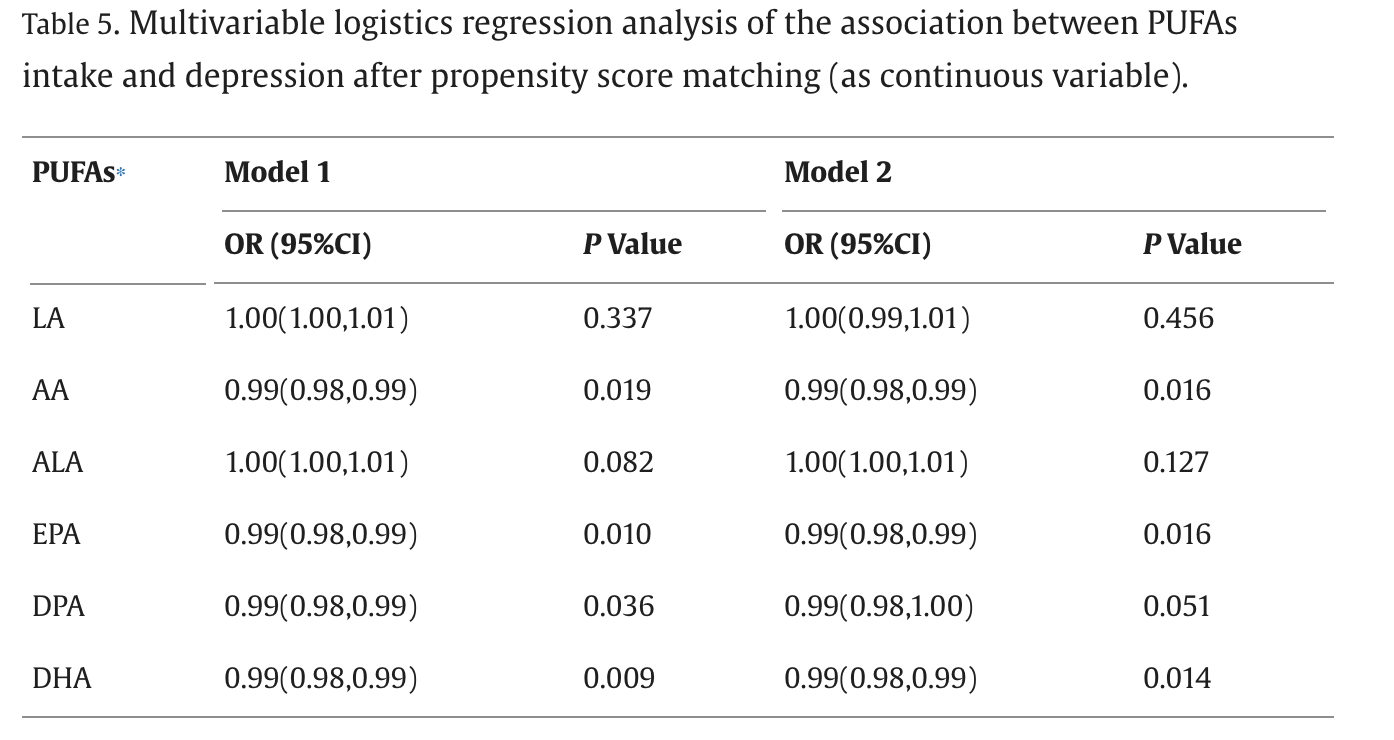
Model 1 adjusted for age, sex, and race, while Model 2 further adjusted for marital status, education, BMI, Poverty Income Ratio (PIR), alcohol consumption, smoking status, physical activity, diabetes, hypertension, kidney failure, heart failure, CHD, stroke, liver disease, and cancer.
PUFAs were initially analyzed as continuous variables and later categorized into quartiles for comparison of interquartile increases. A four-node restricted cubic spline (RCS) was used in Model 2 to assess the dose-response relationship between PUFAs intake and depression risk, with nodes at the 5th, 35th, 65th, and 95th percentiles. Statistical analyses were performed using R version 3.6.1, with significance defined as a two-tailed P-value of <0.05.
Daily intakes (after PSM):
They don’t give the values for the quartile.
As a continuous variable (“per 1 mg/day increment”), after adjustments (Model 2) and propensity score matching, there’s a tiny beneficial effect for both EPA and DHA:
If I interpret Fig. 2 and Fig. 3 correctly, for both EPA and DHA, the potential protective effect is stronger in young (<60), non-smoking, non-drinking, non-diabetic, non-hypertensive women.
For EPA, it seems that the more, the better (linear dose-response relationship), whereas for DHA, it’s non-linear and the confidence interval goes above 1 past some point, so we cannot exclude that high-dose DHA causes depression:
Our study addresses a gap in the literature by demonstrating that both EPA and DHA intake are negatively correlated with depressive symptoms. Specifically, DHA intake showed a nonlinear association with depression risk, whereas EPA intake exhibited a linear relationship. Despite both being n-3 PUFAs, EPA and DHA appear to have distinct impacts on depression. For example, some studies have shown that EPA-enriched supplements are more effective than DHA-enriched supplements in preventing and treating depression (Liao et al., 2019; Grosso et al., 2014; Su et al., 2014). Additionally, EPA was shown to be more effective than DHA in mitigating weight loss and depressive-like behavior in a mouse model (Peng et al., 2020). Moreover, a study has indicated that EPA is effective in improving depressive symptoms, whereas DHA does not demonstrate such efficacy (Hallahan et al., 2016). The results of our study indicate that consumption of DHA within a specific range may also be associated with a reduced risk of depression. These findings indicate a need for further research to clarify the comparative effectiveness of EPA and DHA in treating depression. Furthermore, the multivariate logistic regression analysis indicated a significant linear trend in the association between DHA intake and depression risk, suggesting that higher DHA intake is generally associated with a lower risk of depression. However, the RCS analysis revealed a significant nonlinearity, with a plateau observed at higher intake levels. This suggests that while higher DHA intake is beneficial, the protective effect may not continue to increase linearly beyond a certain threshold. Further research, particularly longitudinal studies, could help determine the optimal intake level for DHA’s protective effects. Our analysis also revealed a negative correlation between DPA intake and depression, but this association disappeared after PSM, potentially due to confounding factors. Further research is needed to explore the relationship between DPA intake and depression.
Based on the dosage-response charts, the optimal daily dose might be 500 mg EPA + 300 mg DHA. However, VITAL-DEP used a similar dose (465 mg EPA + 375 mg DHA) and found an increased risk of depression after 5 years in their RCT.
My own conclusion: I think this paper strengthens the case for EPA and against high-dose DHA supplementation (anything above 100 mg/day being high-dose, given that Q3 = 62 mg/day). For DHA, 62 mg/day = 434 mg/week. A single serving of salmon, anchovies, mackerel, sardines, or herring gives you more than that.
I believe the IFOS is pretty credible. Any product listed as tested by them can be looked up on the website by lot code.
That brand has some DHA. Didn’t you want to avoid it?
@DeStrider, on @LaraPo ’s point
It’s more expensive, but is there any way you can get the epa rx Vascepa shipped to Hong Kong?
It might have been Anuser who posted you can get it for under $100 for 120 pills. That seems like a great deal and it’s apparently the ‘best’ one available.
I was even tempted to get over my fear of fish (vegan) and try it, but google said one might taste fish… and then I would hurl, so I’m out ![]()
Carlon Elite EPA (EPA-only) on iHerb can be shipped to HK: https://hk.iherb.com/pr/carlson-elite-epa-gems-1-000-mg-120-soft-gels/13839
Otherwise, Vascepa is approved in HK: NAVLIN DAILY
GPR120 internalization: a key mechanism for EPA in antidepressant action
The incidence of depression is on the rise, and currently available antidepressants often exhibit limited efficacy in many patients. Additionally, the underlying mechanisms of depression remain poorly understood. Research has shown that neuroinflammation, driven by M1 microglial phenotypic polarization, contributes to neuronal abnormalities implicated in the development of depression. Eicosapentaenoic acid (EPA) has emerged as a promising therapeutic agent for depression. However, the specific target of EPA’s anti-stress effects is yet to be identified. This study aimed to explore the pathogenesis of depression and elucidate the central regulatory mechanisms underlying EPA’s antidepressant efficacy. In this study, mice were orally administered EPA for five consecutive weeks. During this period, they were subjected to daily chronic unpredictable mild stress (CUMS) and treated with lipopolysaccharide (LPS, 0.5 mg kg−1, intraperitoneally) every other week. The results demonstrated that EPA significantly alleviated neuronal degeneration in the medial prefrontal cortex. Furthermore, EPA improved synaptic plasticity impairments induced by CUMS combined with LPSs, as indicated by the increased protein levels of Nlgn1, PSD95, GAP43, and Syn. EPA also reduced neuroinflammation by inhibiting M1 microglial polarization and NLRP3 inflammasome activation. Notably, EPA exerted antidepressant-like effects by modulating GPR120. These findings suggest that EPA intake can mitigate abnormal mood and behavior induced by elevated immune-inflammatory signals. These findings suggest that EPA intake can attenuate abnormal moods and behaviors induced by elevated immune-inflammatory signals. Therefore, EPA may be a promising strategy for the clinical treatment of inflammatory depression.
The results of several meta-analyses suggest that eicosapentaenoic acid (EPA) supplementation is therapeutic in managing the symptoms of major depression. It was previously assumed that because EPA is extremely low in the brain it did not cross the blood-brain barrier and any therapeutic effects it exerted would be via the periphery. However, more recent studies have established that EPA does enter the brain, but is rapidly metabolised following entry. While EPA does not accumulate within the brain, it is present in microglia and homeostatic mechanisms may regulate its esterification to phospholipids that serve important roles in cell signaling. Furthermore, a variety of signaling molecules from EPA have been described in the periphery and they have the potential to exert effects within the brain. If EPA is confirmed to be therapeutic in major depression as a result of adequately powered randomized clinical trials, future research on brain EPA metabolism could lead to the discovery of novel targets for treating or preventing major depression.
The potential effect of DHA feeding to slow the conversion of EPA to downstream metabolic products in the liver could explain some of the differences between EPA and DHA on major depression outcomes.
But, more surprisingly, we observed that EPA and DHA entered the brain at similar rates in the in situ model, raising the question that if EPA and DHA entered the brain at a similar rate, why were EPA concentrations 250 – 300 times lower than DHA? We found, that even in situ and in under 45 seconds, EPA appeared to undergo rapid metabolism, including beta-oxidation. By using radiolabelled EPA in an in vivo infusion model developed by Stanley Rapoport, we assessed the kinetics of EPA uptake into the brain (Chen et al., 2013). Consistent with our in situ 8 findings, the incorporation coefficient (a marker of the brains capacity for taking up a fatty acid) was similar for EPA and DHA in vivo. Any differences in their rates of uptake could not explain their massive difference in brain concentrations, a finding that was confirmed by Igarashi and colleagues (Igarashi et al., 2013)
We and others have observed that DHA supplementation increases EPA levels (Conquer and Holub, 1996; Metherel et al., 2017; Metherel et al., 2019; Rey et al., 2019; Schuchardt et al., 2016). While this is commonly referred to as retroconversion, a process by 16 which DHA is enzymatically converted "back” to EPA, we have recently reported that the increase in EPA is predominately due to a decrease in its metabolism relative to its synthesis (Metherel et al., 2017; Metherel et al., 2019). While it is not exactly clear which metabolic pathways are involved in the DHA-induced increases in EPA, DHA does appear to be blocking aspects of EPA metabolism.
Brain eicosapentaenoic acid metabolism as a lead for novel therapeutics in major depression 2019
Thanks. The case against DHA is becoming stronger everyday…
I’m compelled to reply because I have been looking for someone else with this experience for years.
I used to take what I now recognize was a low-quality rancid omega-3 supplement, and it did not make me depressed, it made me a jerk. Irritable, snappy, impatient, judgemental, and downright angry, and the effect was fairly immediate. I’m e3/e4 and really wanted to be able to supplement but just could not tolerate how it affected my mood and personality.
Fast forward a few years and I’m now taking a high quality supplement and have none of these effects.
But having spent most of the morning reading on this forum I’m now seriously doubting my high-dose high-DHA strategy. I’m new to this forum although not new to the subject matter. I’m learning a ton, the level of science here is much superior to most of the Internet.
I can agree with that.
I’m so glad that you felt compelled to respond. Your description of how you responded to supplementation exactly matches my experience, but you described it even better than I had! It’s oddly comforting and satisfying to compare notes and know someone truly understands!
What are some of the good epa only supplements? I’m finding that even the ones marketed as “epa” contain a small amount of dha. There’s the Carlson one but the label doesn’t specify the entire composition of the fish oil.
I take Ingennus Pharmepa Restore 1000mg Pure EPA Fish Oil High Absorption rTG Omega-3 IFOS Certified
Readily available on Amazon. I like that it’s IFOS certified, as I’m worried about contaminants. However I only take 500mg dose three times a week. My OmegaCheck reading in April was 5.5 % by wt., according to their range, right at the limit of Relative Risk: LOW. Some people advocate 8 as a minimum, but I’m comfortable at 5.5. YMMV.
I’m reconsidering this, but I take daily:
1400 mg TG-ALA
1688 mg TG-EPA
210 mg LPC-EPA
1313 mg TG-DHA
105 mg LPC-DHA
Which is two capsules Nature Made Flaxseed Oil Extra Strength, three capsules Nordic Naturals Ultimate Omega 2x, and two capsules Fenix Accentrate Omega Max.
My Omega3 Index is 12.8%
Now I’m wondering if I’m getting too much DHA and disturbing the downstream metabolism and neuronal incorporation. My interest is in AD prevention, I have my lipids dialed in with ezetimibe and low-intensity statin.
Unsure why. Have you ever tried plasmologen omega 3?