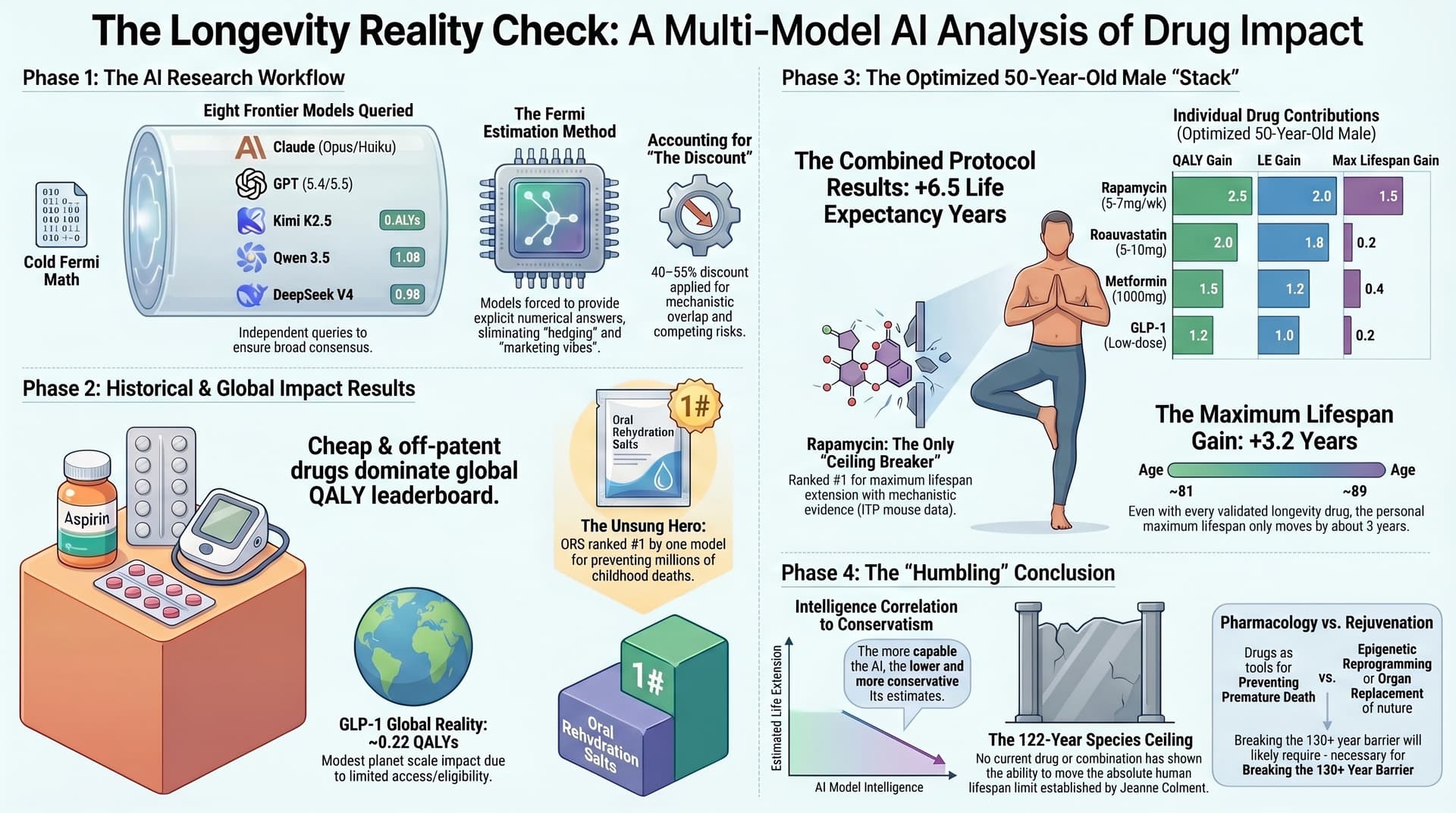
This is where it gets personal. I asked each model: if you had a healthy, well-optimized, exercising 50-year-old male — what are the top 10 drugs, and what happens if he takes them all in a perfectly optimized protocol?
Every model included rapamycin, statins, metformin, an SGLT2 inhibitor, a GLP-1 agonist, and an ARB/ACEi. Most included acarbose, aspirin, and some form of NAD+ precursor or hormonal optimization. Rapamycin was the only drug that most models credited with any maximum lifespan extension potential.
It says he’s “directionally right” (a polite phrase LLMs often use), and supports the anti-hype.message. but it also writes:
The biggest methodological problem is that the article’s “study” is not a study. It is an LLM Fermi-estimation exercise. The author acknowledges this, but then leans heavily on the convergence of model outputs as if that convergence were a form of validation. It is not. LLMs can converge because they share training data, common priors, internet consensus, and similar failure modes.
I also asked it about the Loma Linda “blue zone”, and it wrote:
Yes — that’s a very important counterweight to the drug-centric framing.
Your memory is basically right, with a nuance: the strongest Adventist Health Study finding was that California Adventist men lived about 7.3 years longer and women about 4.4 years longer than other Californians; among vegetarian Adventists, the advantage was larger: about 9.5 years for men and 6.1 years for women. Loma Linda University summarizes this similarly: roughly 7 extra years for Adventist men, 4.5 for women; 9 and 6 years for vegetarian Adventists.
That is huge. And it supports your main point: lifestyle can plausibly move average lifespan by several years, which is larger than what most proposed “longevity drugs” have proven in human
I agree with him that longevity drugs are not going to move the needle much in isolation.