Association of lipoprotein levels with mortality in subjects aged 50 + without previous diabetes or cardiovascular disease: a population-based register study
Lise Bathum et al. Scand J Prim Health Care. 2013 Sep.
Abstract
Objective: This study aimed to investigate the association of lipoprotein and triglyceride levels with all-cause mortality in a population free from diabetes and cardiovascular disease (CVD) at baseline. The European Guidelines on cardiovascular disease prevention state that in general total cholesterol (TC) should be < 5 mmol/L (190 mg/dL) and low-density lipoprotein cholesterol (LDL-C) should be < 3 mmol/L (115 mg/dL).
Design: A population-based register study in the period 1999-2007 including 118,160 subjects aged 50+ without statin use at baseline. All-cause mortality was related to lipoprotein and triglyceride levels and adjusted for statin use after inclusion.
Results: All-cause mortality was lower in the groups with TC or LDL-C above the recommended levels. Compared with subjects with TC < 5 mmol/L, adjusted hazard ratios for the group aged 60-70 years ranged from 0.68 (95% confidence interval (CI) 0.61-0.77) for TC 5-5.99 mmol/L to 0.67 (95% CI 0.59-0.75) for TC 6-7.99 mmol/L and 1.02 (95% CI 0.68-1.53) for TC ≥ 8 mmol/L in males and from 0.57 (95% CI 0.48-0.67) to 0.59 (95% CI 0.50-0.68) and 1.02 (95%j CI: 0.77-1.37) in females. For triglycerides, ratios comparednn with the group < 1 mmol/L in the females agedb 60-70 years ranged from 1.04 (95% CI 0.88-1.23) to 1.35 (95% CI 1.10-1.66) and 1.25 (95% CI 1.05-1.48) for triglycerides 1-1.39 mmol/L, 1.4-1.69 mmol/L, and ≥ 1.7 mmol/L, respectively. Statin treatment after inclusion provided a survival benefit.
Conclusion: These associations indicate that high lipoprotein levels do not seem to be definitely harmful in the general population. However, high triglyceride levels in females are associated with decreased survival.
From the Full Text:
The most striking finding was that compared with the reference levels, high TC, HDL-C, or LDL-C levels were associated with lower mortality in the elderly and this was the case for even very high levels. The finding that high TC or LDL-C levels were associated with a lower mortality is contrary to the general assumption that there is a higher mortality among subjects with high lipoprotein levels. Our findings could seem controversial. However, most studies performed in older adults show an inverse association between TC and mortality and a recent study demonstrated an inverse association between TC and non-cardiovascular mortality in a population free of CVD and statin use at baseline. These findings were significant from the age of 65 years and were largely due to an inverse association with non-HDL-C. Our study demonstrates the same significant inverse association between high levels of TC and its subfractions and mortality in all age groups from as early as 50 years.
PubMed Abstract
Full Text - Open Access
@RapAdmin Addition (4/26) - Google Gemini 3 Pro paper analysis:
A critical nuance of the study lies in its pharmacological findings. While baseline lipid levels above recommended thresholds were robustly associated with unassisted survival, the downstream initiation of statin therapy independently provided a profound mortality benefit across almost all evaluated groups. Because the statin survival advantage occurred completely independent of baseline lipid values, the data suggests that the lifespan-extending properties of statins in the elderly likely derive from pleiotropic effects—such as anti-inflammatory action, immune modulation, and endothelial stabilization—rather than simple lipid reduction.
Ultimately, this analysis implies that the physiological function and prognostic value of lipids shift profoundly as the human organism ages. In primary prevention populations over 50, higher cholesterol may not strictly act as an atherogenic catalyst, but rather as an indicator of robust nutritional status, somatic reserve, and biological resilience. Extremely low cholesterol, by contrast, should elevate clinical suspicion for underlying frailty, sarcopenia, or smoldering chronic illness.
Context: This research was published out of the Department of Clinical Biochemistry at Slagelse Hospital and the University of Southern Denmark, Denmark, in the Scandinavian Journal of Primary Health Care.
Impact Evaluation: The impact score of this journal is 1.8, evaluated against a typical high-end range of 0–60+ for top general science, therefore this is a Low impact journal.
Critical Limitations
-
Reverse Causality: Although researchers excluded subject deaths within the first year, latent and undiagnosed diseases often systematically suppress cholesterol levels long before the patient dies. Consequently, the reference group with the lowest cholesterol may inherently comprise a sicker, failing demographic.
-
Selection Bias: Laboratory tests in this registry were ordered by physicians for specific, unlisted clinical reasons. Truly healthy, asymptomatic subjects without clinical complaints may be systematically underrepresented in this dataset.
-
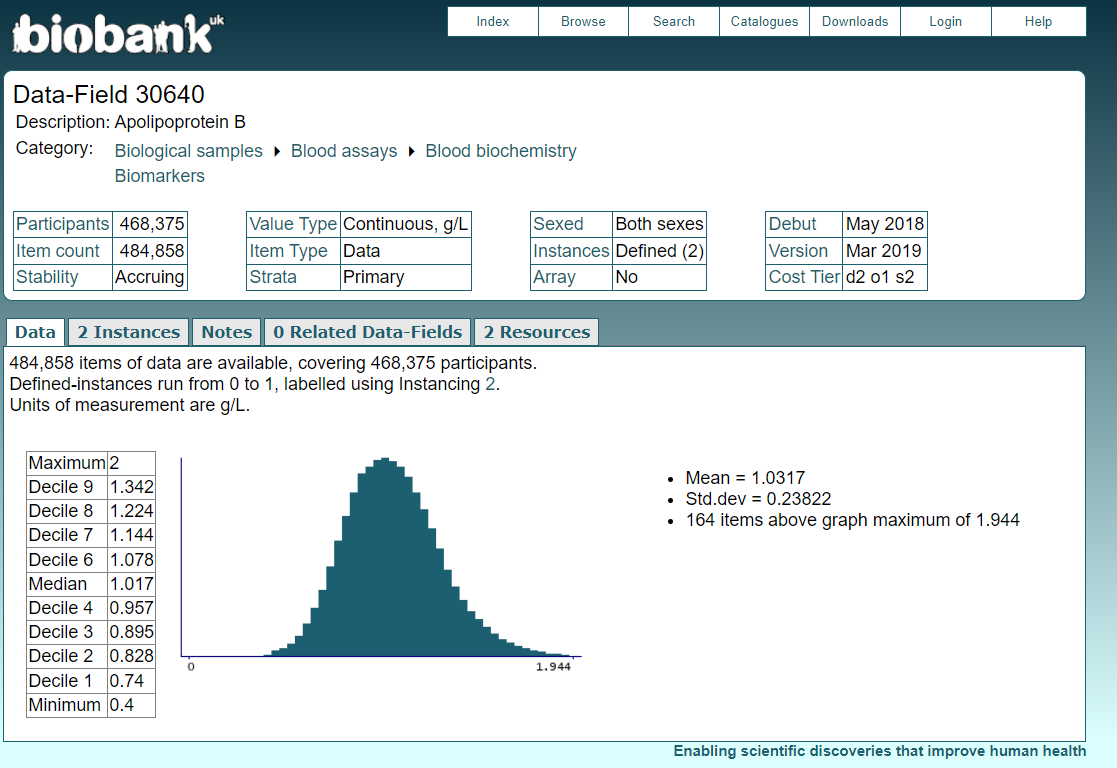
Missing Precision Biomarkers: The study relied entirely on outdated standard lipid panels, notably estimating LDL-C via the Friedewald equation. There is zero data on Apolipoprotein B (ApoB) or Lipoprotein(a), making it impossible to accurately assess atherogenic particle concentration versus harmless buoyant lipid cargo.
-
Lack of Cause-Specific Mortality: The primary endpoint is strictly all-cause mortality. It is entirely unknown whether these subjects died from cardiovascular events or non-CVD causes (e.g., cancer, sepsis), which severely obfuscates the actual physiological mechanism behind the observed lipid “protection”.
-
Data Needed for Full Answers: To separate correlation from biological causation, future human longevity studies require Mendelian randomization involving ApoB variants paired with multi-omic profiling. This is required to determine if structural lipid protection genuinely exists in the elderly, or if high cholesterol is merely a trailing biomarker of a non-frail state.