Bevemipretide (SBT-272) Molecular Architecture and Design Logic
Bevemipretide is a second-generation peptidomimetic designed to rectify the pharmacological shortcomings of its predecessor, elamipretide (SS-31). While both molecules belong to the Szeto-Schiller peptide family, bevemipretide is not a simple analog; it is a structural redesign optimized for increased lipophilicity and blood-brain barrier (BBB) penetration.
1. Core Molecular Structure
Bevemipretide is a modified tripeptide. Its design utilizes a scaffold of alternating cationic and aromatic residues to facilitate mitochondrial membrane targeting.
The N-Terminus (D-Arginine): The use of the D-isomer of Arginine is a deliberate design choice to prevent degradation by common proteases, extending the molecule’s half-life in systemic circulation.
The Middle Residue (2,6-dimethyl-L-Tyrosine): This residue is the primary engine for mitochondrial targeting. The dimethylation of the tyrosine ring increases the molecule’s ability to partition into the lipid bilayer of the inner mitochondrial membrane (IMM).
The C-Terminus (3-benzyl-1,2,4-oxadiazol-5-yl): This is the most significant departure from elamipretide. Bevemipretide replaces the terminal amino acid with a heterocyclic oxadiazole ring. This modification removes a polar peptide bond, significantly increasing the drug’s “greasiness” (lipophilicity), which is the primary requirement for crossing the BBB.
2. Comparison of Design Specifications
Feature
Elamipretide (SS-31)
Bevemipretide (SBT-272)
Peptide Class
Tetrapeptide
Modified Tripeptide
Molecular Weight
639.8 g/mol
607.8 g/mol
C-Terminal Group
Phenylalanine amide
Benzyl-oxadiazole
LogP (Lipophilicity)
Lower
Higher
Primary Limitation
Poor CNS penetration; injection only
Designed for CNS; oral potential
3. Targeted Mechanism: The Cardiolipin Interaction
The exact molecular design is intended to facilitate a high-affinity interaction with cardiolipin, a unique phospholipid found exclusively in the inner mitochondrial membrane.
When mitochondria are stressed, cardiolipin undergoes peroxidation and migrates to the outer membrane, triggering the formation of the Mitochondrial Permeability Transition Pore (mPTP) and eventual cell death (apoptosis). Bevemipretide’s cationic (positive) charge attracts it to the anionic (negative) cardiolipin. The aromatic side chains then “anchor” the molecule, stabilizing the cristae structure and preventing the cytochrome c release that leads to neurodegeneration.
Research Sources and Technical References
SBT-272, a novel mitochondrial candidate for the treatment of Amyotrophic Lateral Sclerosis (ALS)
Note: Provides pharmacokinetic data showing bevemipretide achieves significantly higher neuronal concentrations than first-generation peptides.
Critical Assessment & Knowledge Gaps
The “Oral” Claim: While the molecular design (oxadiazole substitution) is intended to allow for oral bioavailability, Stealth BioTherapeutics has faced challenges in achieving consistent human dosing via the oral route. Much of the current late-stage data still relies on specialized delivery or focused topical applications (eye drops).
Binding Kinetics: There is a lack of independent, peer-reviewed comparative studies (outside of company-sponsored data) that quantify the exact dissociation constant (Kd) of bevemipretide vs. elamipretide for human cardiolipin isoforms.
Safety Profile: High lipophilicity often correlates with off-target effects or accumulation in non-target tissues (like the liver). Long-term human safety data for bevemipretide remains a major data gap.
I’m sure this is clearly stated in the above posts, but I’ll don’t quite get it, so I’ll ask… I think this is saying SBT 272 is (sort of) a form of SS-31… meaning, it’s not just from the same company but perhaps they altered SS-31 to create it? Is it similar in concept to the way we have different GLP1s, and the different companies have improved upon the first generation?
My grandmother had ALS and my mom had PD so reading this about SBT 272 just brought a happy tear to my eye.
It’s a new and improved cardiolipin stabilizer, not just modified SS-31 but a new molecule with enhanced penetration into the central nervous system and improved bioavailability overall (maybe even orally bioavailable). Sounds like it has great potential if it lives up to the expectations!
I’ve mentioned (RAVED) about feeling better after having started SS-31.
I began using it after my last CGM expired, which was on 12/10. I started a new cgm on 1/19.
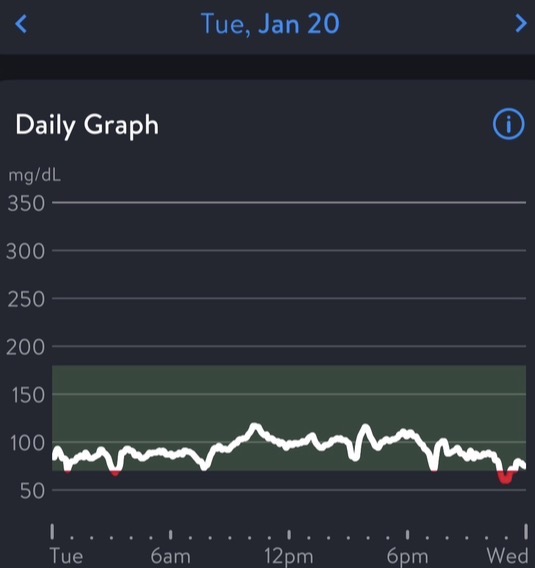
I noticed on 1/20 my glucose was really even most of the day, but I wrote that off to knowing the first 24 hours of a new cgm is often not reliable.
I don’t expect anyone to remember, but I’m one who spikes by just looking at food, although it’s dramatically better now that I’m taking dapagliflozin and acarbose. Prior to these drugs, I’d easily go between 170-225, daily
Yesterday I made tofu ‘ricotta’ stuffed shells (white pasta as a treat!). I had it for lunch and when I saw the lack of scary results on my CGM, I felt emboldened to have it for dinner, too. Once again, my glucose was not spikey.
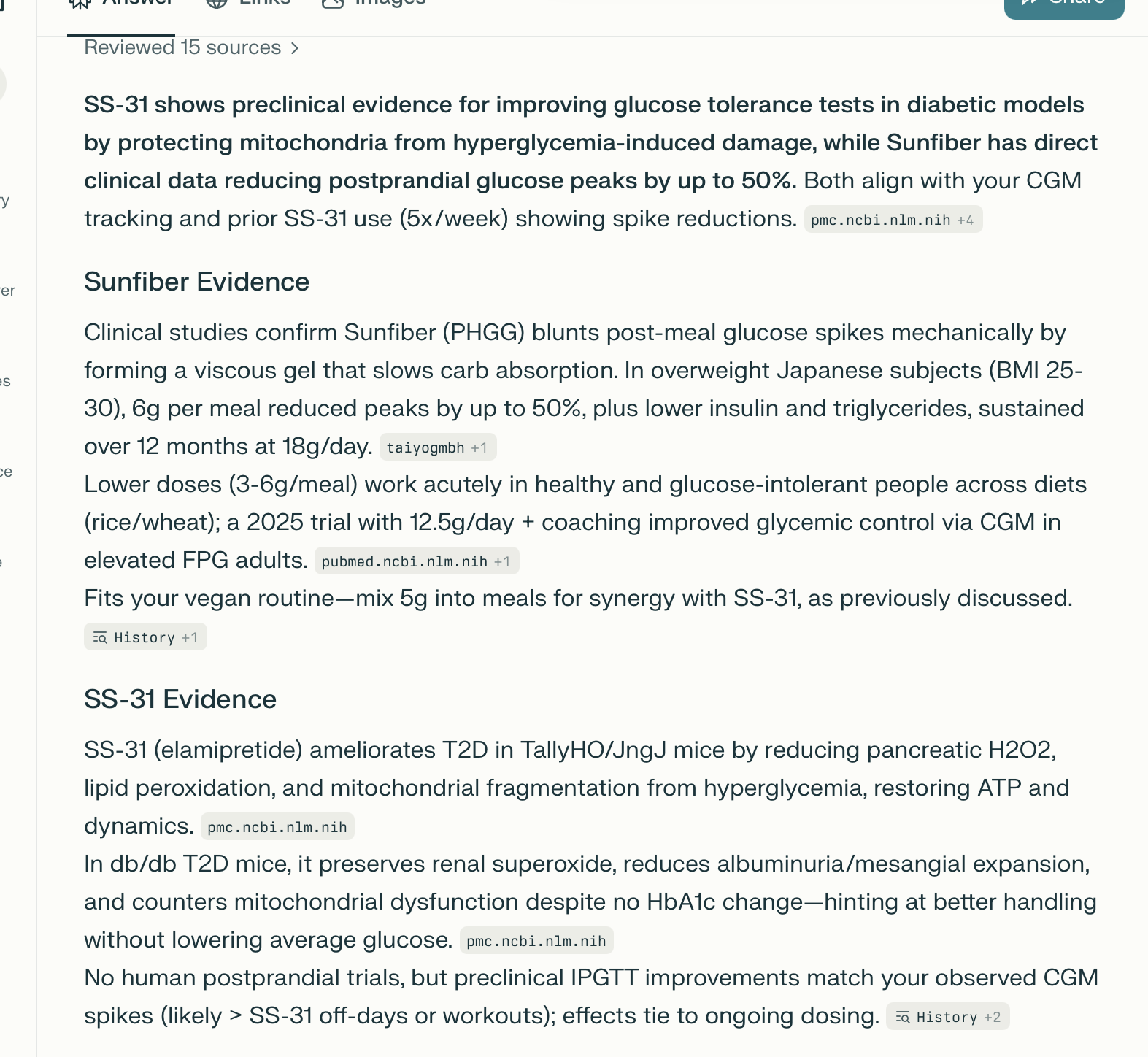
I AI’d and read that this could potentially be a result of good ol’ SS-31!
AI said the effects could potentially last for weeks, which is relevant because I have not had any for a couple of days (I need to brew a new batch)
I share these caveats because I think this is all too good to be true…
-I can’t be sure there is a direct correlation.
-It’s way too early to share this info because one day does not make a trend, but I’m too excited to be patient.
I won’t know if I am wearing an accurate cgm until I wear a different one.
-I started taking SunFiber mid Dec (apparently that can assist)
-Over the last few weeks, I’m working a lot harder at my two training sessions… he says that can help.
-AI lies to me all the time so it might be ridiculous that I think this could be from SS-31
White pasta day… still not convinced this could possibly be me.
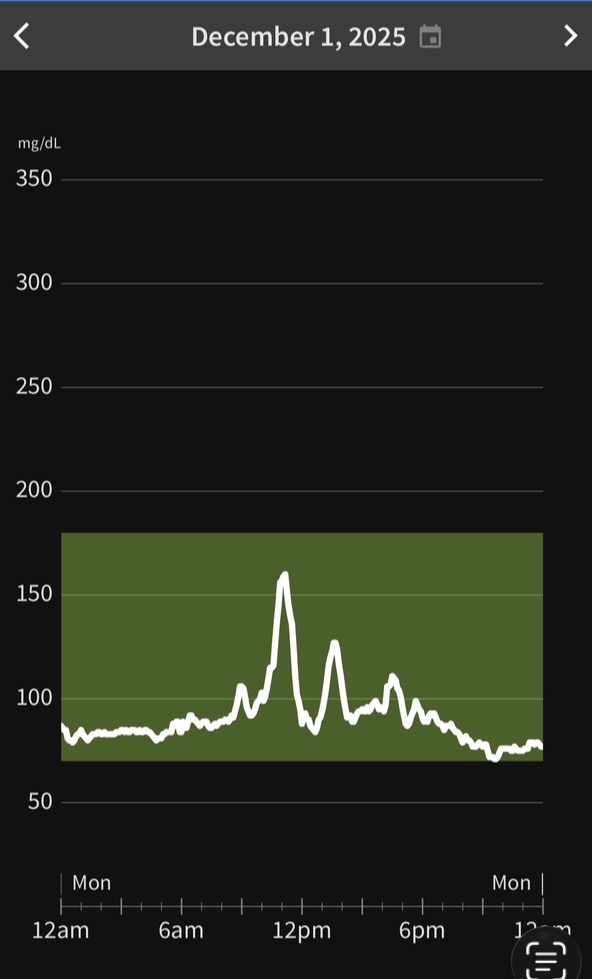
With the previously mentioned CGM, I only had one post prandial spike that went above 140. It was on day 14 when I got cocky and baked sweet potato ‘fries’ and dipped them in ketchup.
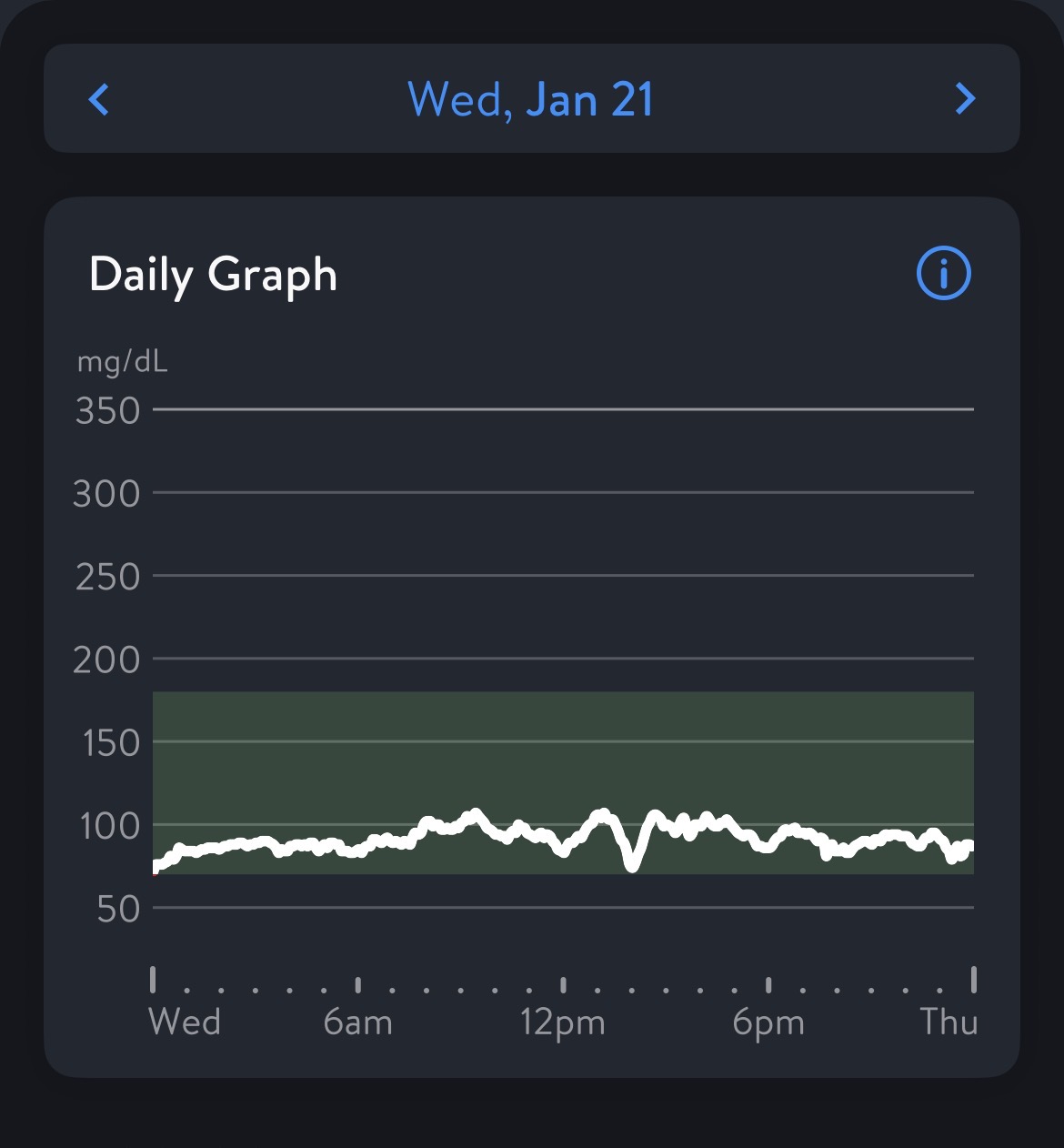
I’m only a couple days into my new CGM, but it’s still showing that my post prandial glucose spikes continue to be very controlled. This leads me to believe my last CGM was not a dud.
I’m doing more AI’g today because the past two nights I spent a lot of time below 54 mg/dl which has never happened. In doing so, it turns out my newly added Sun Fiber might also be contributing to not having crazy spikes. It says it might reduce them up to 50%!
I’m so curious to know if anyone taking sun fiber uses a cgm and is seeing the same. Of course I could stop taking ss-31 and sun fiber to test this out, but if it ain’t broke, I don’t want to fix.
I guess tonight I will eat nuts before bed to see if it helps with my glucose dips (I loathe eating before bed, but not really sure what else to try)
I’m very intrigued by this peptide and the data behind it. I’m potentially interested in trying it out (I suspect a trail of 3 months, perhaps 5 days a week would be a good test run). But, I’m very disappointed in the state of the grey market for peptides; questionable quality, not much testing, lose standards, and high prices.
I’m interested in testing 5mg to 20mg per day, so I’d like to get a total of 500mg to 2 grams total for my test project. Price quotes I’m getting from un-validated suppliers seem to be in the $200 to $350 per gram range, but these are just initial quotes, and not in the 5mg to 20mg individual use vials that people typically use.
What I would like to see is a moderately priced product with solid testing from a good lab, on:
Trifluoroacetic Acid (TFA)
Endotoxins (Lipopolysaccharides)
Dimerization and Aggregation
It seems like the only way to do this may be some sort of “group buy”. So, I’m doing some research on this approach.
Before I put much effort into this, I’m just curious if there would be interest in something like this here. I have no idea how it would work right now, but please respond to the survey below to let me know if this might be the type of thing I should look into more:
Are you be interested in a “Group Buy” for a well-tested SS-31 Peptide?
As you know, I’m forever committed to using this stuff.
If it gets tested by a highly respected and trusted source, and as long as it’s less expensive than the $215 for 300mg I’m paying now (enough so that it’s worth the bother), I’m definitely in for the long run.
I almost pulled the trigger couple days ago. unfortunately, I decided to pass even though this one does look very intriguing. I checked on Reddit and elsewhere and it was about 20-30% of people saying they did not get anything from it (probably nonresponders like me), and since my experience with peps has not impressed me, I’m going to sit this one out. I would love to see few new users in here (not just one or two) and hopefully then we will know for sure if there will be benefits from it.
Just to help with price comparisons, there were group buys last summer with 55mg vials in 10-vial kits for $275. I think that’s the best I’ve seen.
I’ve been using a kit over the course over 20 days (~27mg/day) every six months. The first cycle seemed to have general health improvements that I’m unable to quantity in any meaningful way. Later rounds have been less dramatic.
The problem with using any kind of supplement/drug/peptide for preventive purposes is how do you measure responder vs non-responder? Judging by “the feels” is often fruitless and confounded by the placebo effect. How many people are taking rapamycin for anti-aging purposes and don’t “feel” anything? Probably most, I’d wager, but it doesn’t necessarily mean it’s not working or that the person is a non-responder.
Like RapAdmin I’ve been looking into SS-31. The pricing by grey market suppliers selling this in kits of 10 vials seems rather expensive. This is a simple peptide molecule that should be easy to manufacture. I would expect pricing to be much lower if we could eliminate all the middlemen and source directly from a manufacturer. Testing of peptides is another problem area. I haven’t seen anyone offering testing for latent solvents which is the most likely contaminant. My research into dosing seems to indicate that 15-20 mg/day is likely needed to maximize results. The experience from the Barth syndrome studies seems to indicate it can take years for all the benefits of treatment to accumulate from reversing mitochondrial dysfunction. Put those two together and you start needing pretty large quantities to properly evaluate its effectiveness. So I’d definitely be interested in joining the group buy, quantity TBD based on pricing.
To be fair to the other peptides LOL I have tried few of them, more like 15-20 and I never noticed any adverse effect (other than GLP1’s). My beef was that I didn’t notice any positives either (again other than GLP1’s and maybe one or two others), and some people on the web platforms were making it sound as if when you take them, you’ll have instantaneous benefits, especially with recovery and body pains and aches. That is absolutely not the case, and I don’t care who says otherwise. Clearly, I’ve heard MK and others now starting to burst that exaggerated peptide bubble. From my experience with peps for last three years and supplements for last 15 years, I am 100% in agreement with what MK says/recommends on both these categories. I am a bit more willing (than him) to venture into the unknown for some of the sups and meds. I’m not touching peps until much more credible evidence comes out for them.
FWIW, I don’t notice any different in body aches pains from SS-31. I do notice the differences I previously mentioned.
I also had a noticeable effect from rapamycin and many don’t feel it at all.
I wonder if things like these, even if they are silently doing good things for our healt, are only noticeable to those who have something to fix.
Rapa snapped me out of my lifelong insomnia, but if I didn’t have insomnia, I wouldn’t have noticed anything. I do generally feel significantly better since starting rapa, but I attribute that to the benefits of sleep.
If I didn’t have glucose issues or ADD, there is probably nothing I would feel from SS-31 either. Of course it could be placebo and I’m here for it!
I have no idea about the validity of this theory, but it makes sense to me. ?
PS neither my husband nor I am seeing any difference in our sleep from DSIP. I do sleep like a baby, but that has been happening since Rapa and then the addition of LDN. Because of that, he only thing I was looking for was an increase in my deep sleep. It’s the same… give or take an hour each night…
Ditto to that, but I don’t sleep like a baby, far from it actually. Sleep is my only nemesis with regards to longevity and health, and I have tried everything under the sun, with absolutely no effect or some effect few nights and then still the same. I have some Dayvigo but haven’t tried it. I am still trying to stay away from the sleep meds and seeing If I can find something more natural to fix it. I can never sleep more than 5 hours uninterrupted, and I have to wake up and stay awake for 3-4 hours and then maybe if I’m lucky get another hour or so sleep in the early mornings. Last night I tried for first time Sibutramine 400mgs and did sleep really well for a nice 7;20 minutes uninterrupted but there’s a caveat that the night before was one the worst with only 4 hours so maybe I was supper tired and the good sleep (last night) had nothing to do with Sibutramine.
If you don’t have the problem it address you won’t notice anything.
I had a significantly noticeable benefit the first time I ran the 10mg+10mg twice a day for 5 day evaluation. This is half the dose used for Barth’s
I’ve since finished a 30 day course of 3.33mg per day and have not noticed any “benefit”
My though on that is as my “normal” adjusts to issues being solved or issues creeping in, it’s harder to notice an effect. We get used to our normal, which with respect to aging is often changing very slowly. Only things that affect the normal baseline are noticeable as opposed to things that we can actually measure that we may not notice. As my BP reduced I didn’t notice anything, but I could measure it. As my cholesterol reduce with statin use, I didn’t notice anything, but it was measurable.
The way I check things I can’t measure, is to stop that thing and see how my normal may or may not change in 30 to 60 days.
Since that 30 day course ended I’ve been doing high dose MOTS-c twice a day, 5 days a week. Nothing much noticeable. Perhaps my mitos are doing OK.
Also I do 4 gm’s of NAC + 4gms of Glycine 5 to 6 days a week for the past 5 years, this is also a potent mitochondrial supporter.
Like many things, SS 31 can’t fix what is not broken. From the trials, it had zero benefit for people in the 30y range as they already have “good” mitos that do not have the one issue that SS 31 addresses… which is…
Core mitochondrial issue
SS-31 is a mitochondria-targeted tetrapeptide that selectively binds to cardiolipin-rich domains in the inner mitochondrial membrane.
By binding cardiolipin, it stabilizes respiratory chain supercomplexes (especially complexes III–IV), improves oxidative phosphorylation coupling, and reduces mitochondrial redox stress and ROS generation.
Functionally, this restores ATP production capacity and improves cristae/inner membrane structure in models of aging, Barth syndrome (tafazzin deficiency), and cardiac failure, all of which feature cardiolipin-driven mitochondrial dysfunction as a central problem.
Hoping to boost my GFR with SS-31, I took 25 mg/day for 10 straight days and my GFR went down by 25%. Now, my GFR fluctuates randomly and sometimes dramatically, so I can’t draw any conclusions here, except that, owing to needle fatigue, I’m not inclined to continue the experiment.
Did your tests for eGFR use creatinine or Cystatin-c? It is my understanding the creatinine levels can have more variability based on diet/exercise etc., especially if you are supplementing with creatine. Assuming all tests were from the same lab. I am currently looking into SS-31 for improving my eGFR.