Super Panda Peptides, a new vendor selling on Discord and PeptideChat. $300 for 50 mg X 10. I have a vial being tested by Finnrick, but I was too impatient to wait for the results. I did filter the solution.
1 Like
I test my GFR every two or three months, always with creatinine, using both Labcorp and my local hospital. I don’t use creatine and I’m not a mesomorph.
GFR decreases with age, and the drop accelerates after age 70. I’m 78 and I have CKD, so this is not entirely unexpected.
You’ve never checked your GFR by cystatin C just to make sure it’s consistent with the creatinine-based measurement? I certainly would, for something this important. My cyst C GFR tends to run 20+ points higher than my creatinine-based GFR, even when I completely stop creatine supplements for several weeks and avoid exercise for 3 days prior to creatinine measurement.
4 Likes
Now that you mention it, I did have a strenuous workout on the day before the test, a day when it was 60 degrees, the first nice day in four or five months and so I really pushed it. I was sore when I had the blood draw. I bet my GFR would be 10 points higher if I took the same test tomorrow. I’m glad you brought it up.
3 Likes
Where do you inject yourself, Beth?
I’ve tried stomach and thigh and prefer my stomach. I’m not sure if it’s less sensitive or if it’s just about it’s a closer reach ?
1 Like
Beth, do you notice anything with regard to your energy levels when taking SS-31?
2 Likes
It’s really hard to tease out.
Am I getting more things done now because it’s tamping down my ADD or is some of it attributed to more energy…?
I do feel I can go off my t3 now, so there very well might be an energy component in there. I am just not sure about this one. My hunch is if there is more energy, it’s not drastic enough for me to be sure about it.
3 Likes
The ADD effect is interesting. That gives some weight to the theory of mitochondrial dysfunction being the root cause of many psychological conditions. Are you currently taking anything else for the ADD? How does SS-31 compare to other interventions you’ve tried for the ADD?
@Beth , this is really interesting. I have never heard of this - it seems to suggest that there is a reasonable theoretical basis for it to be helpful:
Scientific and Clinical Evidence of Mitochondrial Dysfunction in ADHD
1. Clinical and Biomarker Evidence
Mitochondrial dysfunction (MD) is increasingly recognized as a foundational factor in the pathophysiology of attention-deficit/hyperactivity disorder (ADHD). Because direct brain biopsies are clinically prohibitive, evidence is primarily derived from peripheral biomarkers and ex vivo cellular models.
- Mitochondrial DNA Copy Number (mtDNA-cn): Clinical studies demonstrate that children diagnosed with ADHD exhibit significantly higher mtDNA-cn in peripheral blood compared to healthy controls (Öğütlü, 2021). This elevation is generally interpreted as a cellular compensatory mechanism attempting to offset bioenergetic deficits and mitochondrial impairment (Almutairi, 2024). Notably, a one-year follow-up study observed that as ADHD symptom severity decreased in treated patients, mtDNA-cn also showed a correlated reduction, suggesting that ameliorating ADHD severity may coincide with normalized mitochondrial function (Öğütlü, 2021).
- Cybrid Cell Models: To isolate mitochondrial pathology from nuclear DNA, researchers have utilized cybrid cell lines by fusing platelets from ADHD patients with neuroblastoma cells lacking mitochondrial DNA. ADHD cybrids demonstrate significantly reduced cellular and mitochondrial respiration, decreased ATPase 6/8 transcript levels, impaired complex V activity, and a loss of mitochondrial membrane potential (Verma, 2016). Because cybrids isolate the mitochondrial genome’s influence, these findings provide direct evidence of intrinsic mitochondrial bioenergetic failure in ADHD phenotypes (Verma, 2016).
Theoretical Basis for SS-31 (Elamipretide) in the Treatment of ADHD
Currently, there is no direct scientific research, clinical trial data, or specific in vivo animal modeling explicitly evaluating the peptide SS-31 (elamipretide) for the treatment of Attention-Deficit/Hyperactivity Disorder (ADHD).
However, there is a highly robust theoretical basis for its potential efficacy. This rationale is constructed by mapping the well-documented molecular mechanisms of SS-31 onto the established pathophysiological mitochondrial deficits observed in ADHD.
1. Mechanistic Overlap: Cardiolipin Stabilization
The core theoretical argument for SS-31 in ADHD rests on its highly specific mechanism of action. SS-31 is a cell-permeable, mitochondria-targeted tetrapeptide that selectively binds to cardiolipin , a unique phospholipid expressed almost exclusively on the inner mitochondrial membrane.
- The ADHD Deficit: As established by cybrid cell models of ADHD, patients exhibit impaired electron transport chain (ETC) function (specifically complex V), loss of mitochondrial membrane potential, and excessive reactive oxygen species (ROS) leakage.
- The SS-31 Mechanism: By binding to cardiolipin, SS-31 stabilizes the architecture of the inner mitochondrial membrane and the ETC complexes (particularly cytochrome c). This interaction prevents electron leakage, thereby reducing the generation of ROS at the source while simultaneously restoring ATP synthesis. This directly antagonizes the bioenergetic failure and redox imbalance hypothesized to drive ADHD neurobiology.
2. Evidence from Analogous Neurological Models
While unstudied in ADHD, SS-31 has demonstrated significant efficacy in preclinical models of cognitive impairment that share downstream pathologies with ADHD (neuroinflammation, oxidative stress, and synaptic dysfunction).
- Protection Against Neuroinflammation-Induced Cognitive Deficits: In mouse models injected with lipopolysaccharide (LPS) to induce severe neuroinflammation and oxidative stress, pretreatment with SS-31 prevented mitochondrial dysfunction, reversed the loss of dendritic spines, and preserved hippocampus-related learning and memory. It also facilitated the regulation of brain-derived neurotrophic factor (BDNF), a critical protein for synaptic plasticity that is frequently dysregulated in neurodevelopmental disorders.
- Reversal of Sleep Deprivation Deficits: Short-term sleep deprivation rapidly induces oxidative stress and cognitive/attention deficits. In aged mice, administration of SS-31 prevented sleep-deprivation-induced learning impairments, restored brain ATP levels, and decreased inflammatory cytokines. Given the high comorbidity of sleep disturbances and ADHD, this neuroprotective effect on executive function is highly relevant.
- Dopaminergic Protection: Preclinical studies in Parkinson’s disease models demonstrate that SS-31 protects dopaminergic neurons from oxidative damage. Because dopaminergic pathways in the prefrontal cortex and striatum are structurally energy-demanding and highly susceptible to oxidative stress, preserving their mitochondrial efficiency is theoretically beneficial for the dopamine dysregulation seen in ADHD.
3 Likes
That is interesting. It’s worth nothing I know it’s not placebo because I didn’t google until after I noticed my newly found consistent focus and mental clarity.
On that note… when I first started rapa and commented how my lifelong insomnia vanished (not that every night was perfect), @John_Hemming said rapa can fix mitochondria, so it made sense it could therefore fix my insomnia (of course he said it in a more scientific way!).
If I recall correctly, today I also noticed him say in another thread that spectrum conditions might be related to mitochondria.
(I’m tagging you John incase I’m saying of this incorrectly).
@fasterfour last night I was just addressing your question in another thread… here is a cut and paste…
I didn’t know I had ADD until I was aprox 40 (almost 20 years ago). My sister in law had a hunch and handed me an adderall. The clouds parted and the angels sang. Everything became crystal clear (focus, no fog) and I could get things done.
I was on it for probably 60-90 days, an incredible 60-90 days. Then, at a cardiologist appointment, he said ‘do you know it’s speed and causes vasoconstriction and will increase your risk for a heart attack?’… I said, nope, no one told me. I never took it again.
Those glorious 60-90 days… that is exactly how I feel now.
I’d procrastinate and could never get myself do anything I didn’t want to (mostly admin things), but I could hyper focus on things that were in my wheelhouse.
I’m getting tons of things done all the time now. Nothing super human, but I’m just ‘normal’. I also notice it a lot here too. The health/science topic has never come easily for me, not that it’s easy now, but I used to torture myself trying read one of these threads in order to get it to register (and often would fail), but now I can focus on things and my mind won’t wander.
Speaking of feeling great, I had a long meeting with my doc today to go over everything I’ve been doing and to discuss my results… everything is so different now that we decided to do a trial of going off my T3 (staying on T4). I was always sluggish and foggy, but now that I’m not, we are seeing if I still need it (can be a net negative for bones and heart rate, so I thought I’d see).
It didn’t seem like this could be real, but it made sense after hearing @John_Hemming say ADD might be a mitochondrial issue… TA DA!
I’ve never tried anything else for my ADD.
4 Likes
I thought that just the muscle heads had residual creatinine, but after abstaining from sprinting for three days, I checked my GFR again and it went up by a third. I expect I’ll see another jump when I try Cystatin C. I’ve also learned that intervals will spike my PSA, alarming my urologist.
2 Likes
I’m stopping SS-31 and changing to ergothioneine (EGT) after learning more about EGT and running a comparison through Gemini. SS-31 seems more potent for repairing damage, but in the absence of a specific disease state, EGT seems much more appropriate for long-term protection against mitochondrial damage. The fact that we have specific transporter proteins for absorption of EGT from the gut and other transporters for uptake into the mitochondria says to me that we’re pre-programmed to use this compound and that we actually need it for optimal health. The fact that it’s highly orally bioavailable and not made in an underground Chinese lab requiring injection helps, too:
"While both Ergothioneine (EGT) and the peptide SS-31 (also known as Elamipretide) are elite mitochondrial protectors, they operate through fundamentally different biological “blueprints.”
Think of EGT as a long-term shield that prevents damage, while SS-31 is a precision structural engineer that repairs the mitochondrial machinery itself.
- Mechanism of Action
- EGT (The Shield): EGT is unique because it is highly stable. Unlike other antioxidants (like Vitamin C) that can become pro-oxidants under stress, EGT remains neutral. It specifically accumulates in the mitochondria to neutralize Reactive Oxygen Species (ROS) and singlet oxygen. It acts as a specialized “sink” for the metabolic “exhaust” produced during energy creation.
- SS-31 (The Architect): SS-31 doesn’t just “soak up” stress; it targets cardiolipin, a phospholipid essential for the structure of the inner mitochondrial membrane. When cardiolipin is damaged, the mitochondria “leak” energy and stop producing ATP efficiently. SS-31 binds to cardiolipin, prevents its oxidation, and physically reshapes the mitochondrial cristae to jumpstart energy production.
- Bioavailability and “Staying Power”
- EGT: Your body has evolved a specific transporter (OCTN1) just to pull EGT into cells and mitochondria. Because of this, EGT has a very long half-life (around 30 days in humans). It is a “slow and steady” protector that builds up in your tissues over time.
- SS-31: As a peptide, SS-31 is typically administered via injection (though some nasal/topical forms exist). It works rapidly to restore function in acutely damaged tissue but does not stay in the system nearly as long as EGT.
- Therapeutic Application
- EGT is generally viewed through the lens of longevity and prevention. It protects the mitochondrial genome (mtDNA) from the “slow burn” of aging, which is likely why researchers are interested in its role in preventing the neurodegeneration seen in MS or depression.
- SS-31 is being trialed for acute or severe dysfunction, such as heart failure, primary mitochondrial diseases, or severe kidney injury. It is a “rescue” molecule intended to fix a system that is already failing.
Summary for Longevity Context
- EGT is the daily maintenance that keeps the “cellular rust” from forming.
- SS-31 is the high-intervention mechanic you call in when the engine is already misfiring."
6 Likes
Any noticeable or measurable (good or bad) results from your trial of SS-31? What dose, and for how long have you tried it?
1 Like
No, zero noticeable effects at 1mg, 2mg or 5mg/day for months. Annoying side effect is an injection site reaction every single time (swollen lump that lasts for hours, yet another reason for the switch ![]() ).
).
4 Likes
Which brand/dose of Ergothioneine are you planning to use?
Real Mushrooms brand is what I ordered (10mg EGT per capsule, will take 2 caps/day), but I’ll probably switch to the Life Extension brand when I’m done with this bottle since it’s 25mg per 1 capsule and less expensive for the month’s supply, just doesn’t have the beta-glucan that’s in the Real Mushroom brand.
3 Likes
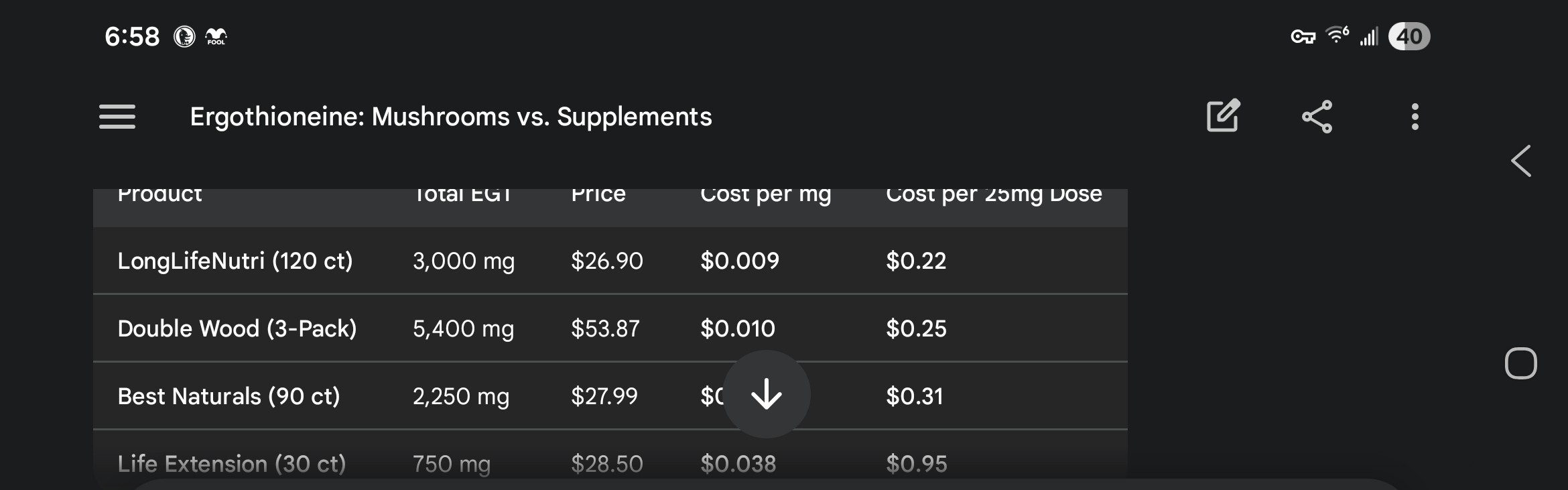
That price is so low for LongLifeNutri that I’m suspicious of its quality.
Finally, I found some information (not sure how good it is) on the top manufacturers of Peptides in China:
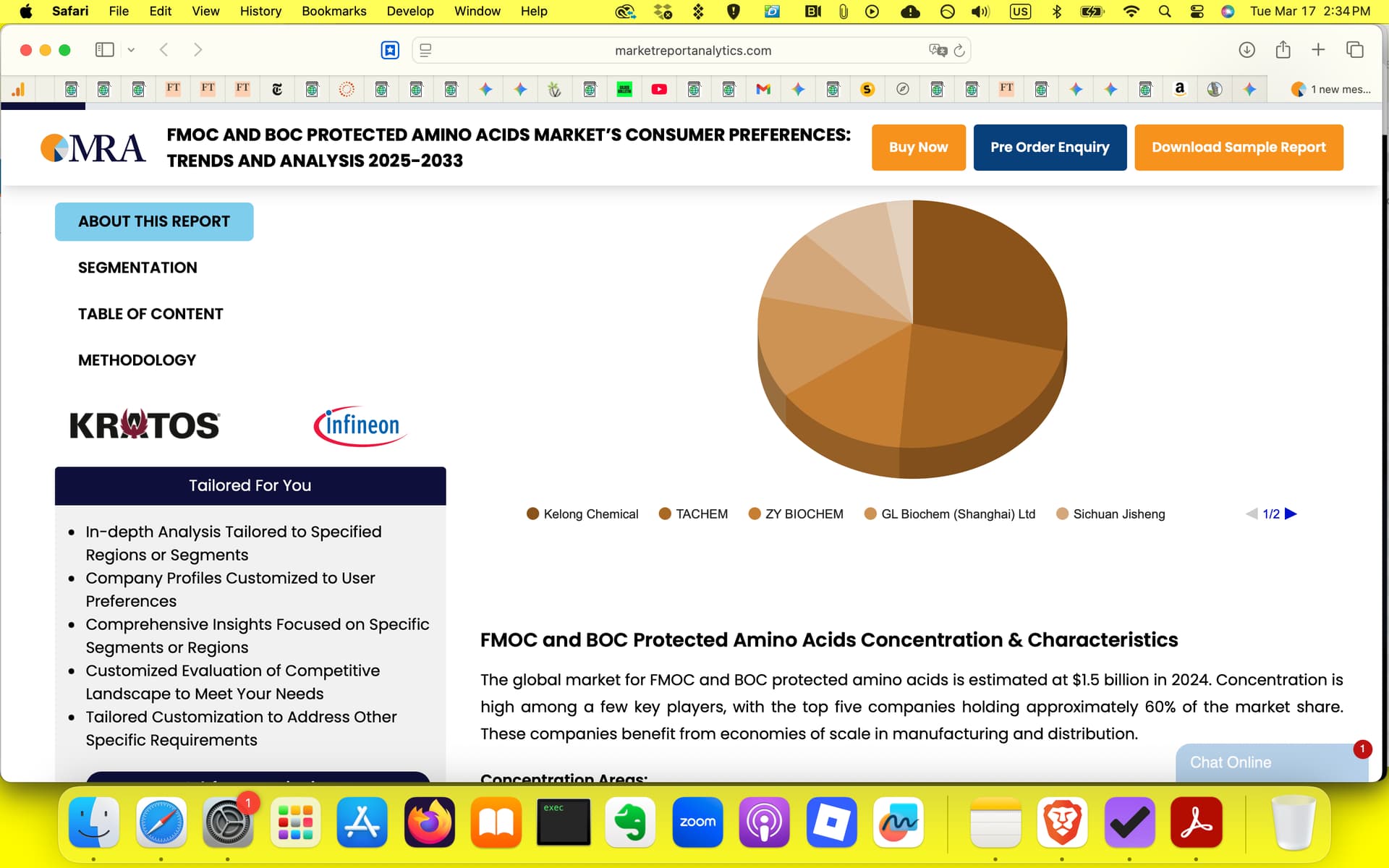
Source: FMOC and BOC Protected Amino Acids Market’s Consumer Preferences: Trends and Analysis 2025-2033
Prices of the “raw” peptide seem to reflect that these guys are the real deal from a manufacturing standpoint:
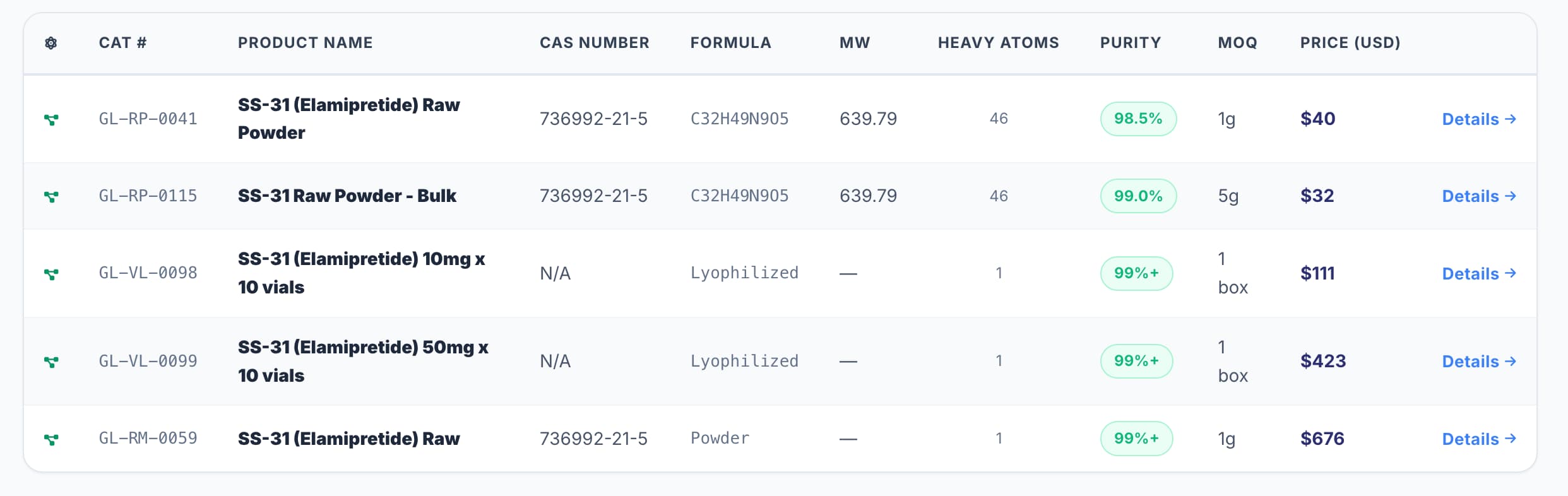
Source: Product Catalog — GL Biochem | Amino Acids, Peptides, Reagents & Resins
3 Likes