I understand what you’re saying. And I have no problem with your questions.
I just see it differently.
“First, do no harm” is replaced with “aging does harm.” Inaction (and action) both have consequences.
I agree with @desertshores on both points - the testing suggestion you’re offering isn’t practical, and senolytics should be taken intermittently. I consider my “once every two month” an appropriate intermittent protocol given the research. Fully agreed on both counts.
Yes, I’m making assumptions. We both are. They’re just different.
Yes, there’s uncertainty in every decision I’m making. But I’ve done the research and I’m comfortable with the decisions… for now. I’m not winging it. All decisions are based on known research and followed up with biomarker testing. Each medication has different effects. The interrelationship are complicated. Fully agreed.
So yes, there’s uncertainty and risk. But that risk is being managed to the best of my ability. “First do no harm” is being replaced with a minimalist approach of intelligent risk-managed decisions. My stack is tiny compared to many people because I believe far more is unknown about human biology than known. I say “no” to new ideas/supplements far more often than “yes” to respect the inherent systemic elegance and beauty of human biology.
But aging is inherently risky. And enough is known to take intelligent, risk-managed action to improve outcomes. First do no harm no longer makes sense as offering the best risk/reward outcome.
I fully expect to change this protocol going forward, but not in the way you’re suggesting. I fully expect game-changing discoveries in the field of senolytics and rapalogs that will be vastly superior to what I’m doing now. I’m guessing my current treatment protocol will look laughably crude 20 years from now, but 20 years is too late. Time is of the essence.
I’m guessing from your statement that you’re not understanding the role of senescent cell population growth in aging and how senolytics and senomorphics interact to affect the aging process.
The net compound growth of your senescent cell population only becomes meaningful when measured over many years (a couple decades by age 63, in my case), or 4 decades for @desertshores), and it only becomes symptomatic to how you feel when that burden exceeds certain thresholds of concentration in specific tissues.
You can think of it like a compound return equation in wealth building. When you start at $100, you hardly notice the first few doubles in your wealth (same with senscent cells after age 40). The accumulation remains relatively meaningless. But when you hit 2 million dollars (think age 55-65) and then double again, that sudden accumulation has life-changing implications. The same is true with the senescent burden in your tissues as you compound them during aging.
The chance that I’ll feel any different after a few months of stopping D&Q is unlikely, not to mention that that subjective changed “feeling” could be due to any number of confounding life factors that have nothing to do with cessation of D+Q. It’s simply not a valid test.
Additionally, any subjective change in experience of life with and without D+Q already occurs between every dose since I only take it once every two months. That means my system already spends the vast bulk of it’s time without any D+Q. Taking an extended break would change only one thing - the compound growth of the underlying senescent cell population.
Finally, a few months of change would be similarly meaningless because the existing dosing regimen would mean I would only miss a handful (or less) samples. That’s also not going to be meaningful in this compound growth equation given my current position in that equation.
My suggestion is to study senolytics with a special emphasis on the work by Dr. James Kirkland. He’s a leading researcher in this field providing unusual insights on this topic.
So, can you then stop the Rapamycin?
I’ll have to look into senolytics again, but I just haven’t seen much that convinces me that they offer much beyond what Rapa is doing.
@John_Hemming what are your thoughts on dasatinib and other drugs of this class?
My main concern is the adverse events:
Common adverse effects include low white blood cells, low blood platelets, anemia, swelling, rash, and diarrhea. Severe adverse effects may include bleeding, pulmonary edema, heart failure, and prolonged QT syndrome.
I have not spent a lot of time looking at dasatinib. It strikes me, however, that it is not targeting the generic issue of gene expression and/or mitochondrial efficiency. I tend to be interested in things that improve the mitochondria or gene expression more generally.
When it comes to senescent cells
a) I think a lot of them are stem cells that have got stuck in the process of differentiation because of low power levels.
b) My objective would be (is) to make them function rather than kill them.
I think there are dangers potentially in some circumstances (like in the walls of arteries) with just killing off senescent cells. Also this will act to deplete stem cell availability.
@Todd are you using a particular form or brand of quercetin? I know some people use a quercetin phytosome or quercetin with other things to enhance absorbtion.
With that said, I can’t claim to be an expert in selecting the best Quercetin product. There are others on this forum that probably have that decision optimized. My decision was a best-guess, but my research was far from exhaustive.
This, of course, is one of the dangers of polypharmacy. FOMO as a result of the theory “If we wait, it may be too late.” As I have posted before in various threads, young people need to be more cautious. If you are young, you probably don’t need it.
As an 85-year-old, and you may not fathom this way of thinking: I have lived a good life, and if I accidentally off myself tomorrow, it is no big deal. I have already lived past my life expectancy for people born in 1941. My main concern is to prolong my healthspan and keep my mind functioning properly until the end, lest I become a burden to others.
I don’t know what the cause of Chuck Norris’ death was, but he appeared normal in a recent social media post. Going that way is okay by me. Live long and fall off a cliff.
This is a small study, but it involves humans, not mice. Oddly, it appears that if you were taking fisetin along with D+Q, you did no harm.
Didn’t we already know this? @Rob Tuck posted this in March of '24
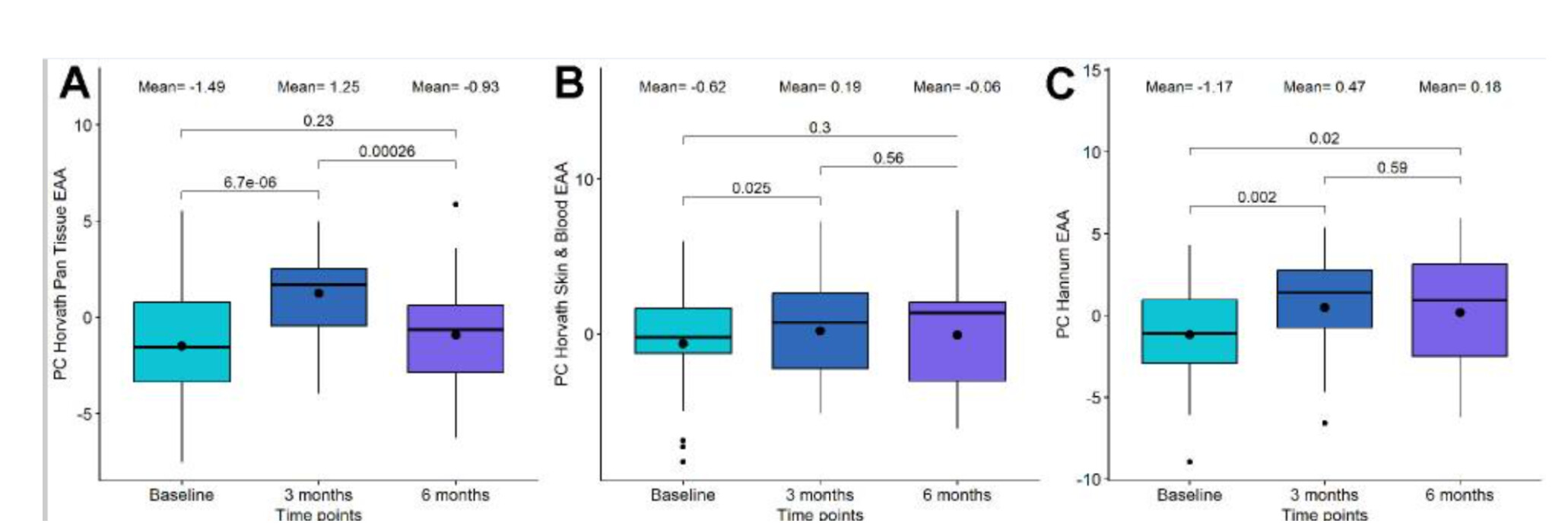
Exploring the effects of Dasatinib, Quercetin, and Fisetin on DNA methylation clocks: a longitudinal study on senolytic interventions
“In the context of our study, the administration of senolytic drugs Dasatinib and Quercitin significantly increases biological age measured by first-generation clocks, with DNAmPhenoAge being the only second-generation clock showing an increase. Notably, there is a lack of significant changes in second and third-generation clocks such as GrimAge and DunedinPACE”
Boxplot showing the evolution of epigenetic age acceleration (EAA) first-generation clocks in the Dasatinib and Quercetin (DQ) study.