Just want to make sure this video from @DrFraser gets the audience it deserves. Very important information.
Let’s hit the like button to give his channel more reach.

Just want to make sure this video from @DrFraser gets the audience it deserves. Very important information.
Let’s hit the like button to give his channel more reach.
You are too kind - I’m trying to get the one up of the panel discussion I did with the other 2 physicians on Rapamycin - that was a great talk. Just trying to get the source video from Vitalist Bay.
The video I think is useful in giving the construct to how to approach longevity medicine. We see so many people focusing on the minutia while missing the elephant in the room.
I’ve had a number of patients on rapamycin come to join my practice, who have had domains 1/2/3 completely unevaluated, and several have critical disease, completely undiagnosed, while pursuing all the clever things.
It isn’t clever to be on sirolimus and dasatinib/quercetin while having severe coronary artery disease, lots of white matter change in one’s brain, and a malignancy undiagnosed. I’ve seen this multiple times. People have to properly evaluate the things that are most likely to kill or disable them and manage those … THEN have a go at all the clever stuff.
Great talk! I think it would be better if we could see more of the slides and less of the couch though. Just an idea for the next time you do this!
I don’t think that’s how the YouTube algorithm works.
Primarily I think it’s
(1) CTR, click through rate.
If you don’t cover topics that people click on then people won’t watch the video. So the title and thumbnail needs to be accurate and interesting, and topics need to be designed with that in mind “What topic do people want to click on?” Clickbait doesn’t work because of
(2) Watch time
If people stop watching in the beginning of the video, then YouTube won’t recommend it to others as people want to watch something else. If they don’t stop watching in the beginning naturally more people will continue to watch.
(3) Continuing watching on YouTube
If people quit watching YouTube after they’ve seen your video maybe they weren’t satisfied with youtube, the last moments of the video if they keep watching need to keep them on youtube.
(4) Long term watching
If people don’t come back for the long term and want to watch your videos over time maybe they weren’t as satisfied they could be, more creators for long term watching keep more people on youtube.
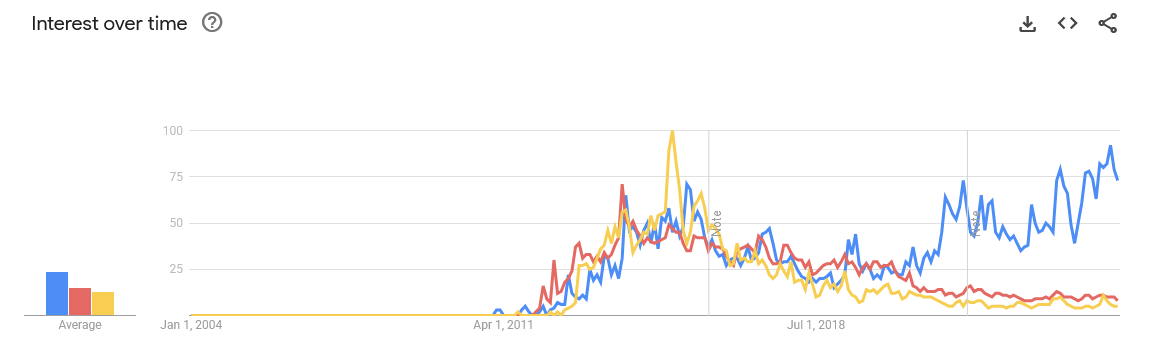
Veritasium changed his approach and explicitly looked at similar youtubers when he did so after tips from MrBeast, categorized with the two videos(https://www.youtube.com/watch?v=fHsa9DqmId8 / https://www.youtube.com/watch?v=S2xHZPH5Sng). There’s a PDF by MrBeast used in his production companies (leaked?) that bring up many of these things: How To Succeed In Mr Beast Production : MrBeast : Free Download, Borrow, and Streaming : Internet Archive
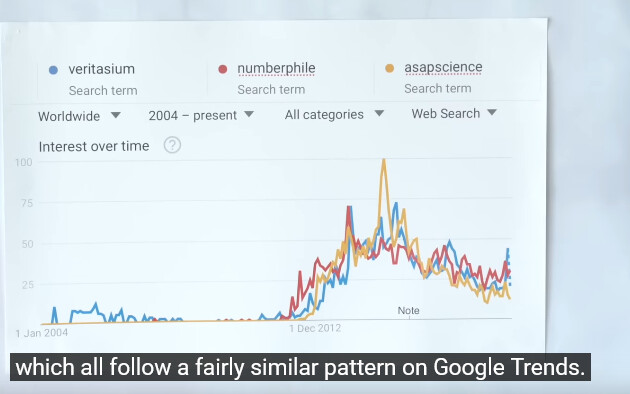
If you look at the same google trend now after his change the effect is clear:
Some speculative non-expert feedback if I’m going to guess for the algorithm: There’s plenty of ways of grabbing attention in the beginning of a video. I don’t think the title or the disclaimer at the beginning of this one helps, it’s better to get straight to the talk, for example, I’m not a lawyer but maybe the disclaimer can be somewhere else, how do other medical info youtubers do it?
Maybe it’s important to be aligned with other aspects of work. How would a personalized medicine business for example reflect that personal nature? What type of videos and in what way, how are they filmed (scripted, if at all), for example? It’s probably important to not overthink it but still align with the overall principles in the two veritasium above and the MrBeast document would be my best bet, and it looks like it works, but I’m not an expert and I don’t personally know if it works. It’s hard and takes a long time regardless even with “best practices”, if there is such a thing.
But if someone else has a good idea. RapAdmin is the king of SEO it seems which is kind of like YouTube but for text and they probably have similar principles.
I agree. The disclaimer should be buried at least a minute into the video, not at the beginning. Probably include a few key clips at the beginning. Similar to how ModernHealthspan and Optispan produce their videos.
I would also cut that carbon monoxide audience question part out. It detracts from the value of the video (and makes it needlessly longer).
Overall, I enjoyed watching the video! It reminded me to get a CAC test for my wife in a couple weeks!
The word Vitalism has a somewhat checkered history. Maybe it is due for a reboot.
Nice to see a nod to Numberphile, one of my favorite YouTube sites.
Beautiful talk. A little fast for me, I would’ve liked more detail on some parts (neurological health!), but within a limited time frame a lot of territory was covered. One of those videos one should watch more than once.
I wish I had a local doctor this informed. Good job Dr Fraser.
O3:
| Section | Details |
|---|---|
| Current Roles | • Founder & Chief Physician, Grant E Fraser MD, PLLC – tele‑medicine longevity & regenerative‑medicine practice (AZ, CA, FL, KY, PA, TN, TX, WA, WI) (grantfrasermd.com) • Emergency‑Medicine Staff Physician, multiple hospitals in the Chattanooga–Nashville corridor (per‑diem) (doximity.com) |
| Clinical Interests | Longevity medicine • Preventive cardiometabolic care • Neuro‑cognitive risk modification (APOE ε4 focus) • Hormone optimisation • Point‑of‑care ultrasound • Acute & rural emergency care |
| Education | MD, University of California San Diego School of Medicine, 1994 (doximity.com) Residency (Family Medicine), Kaiser Permanente Southern California, 1994‑1997 (doximity.com) Advanced Specialty Training, Generalist Emergency Medicine (GEM), Australian College of Rural & Remote Medicine, 2011‑2016 (doximity.com) |
| Board Certifications & Fellowships | • American Board of Family Medicine (ABFM) (doximity.com) • American Board of Anti‑Aging & Regenerative Medicine (ABAARM) (a4m.com) • Fellow, Royal Australian College of General Practitioners (FRACGP) (doximity.com) • Fellow, Australian College of Rural & Remote Medicine (FACRRM) (a4m.com) • Generalist Emergency Medicine (post‑fellowship credential, ACRRM) (doximity.com) |
| Licensure (active) | CA (1995‑2027) • TX (1997‑2026) • TN (2016‑2026) • KY (2019‑2026) • AZ, AL, FL, WA, WI, PA (varying expiry) (doximity.com) |
| Awards | • Emergency Department Director of the Year – American Physician Partners, 2018 (doximity.com) • Critical‑Care Faculty of the Year – University of Queensland (visiting faculty), 2014 (doximity.com) |
| Media & Outreach | Creator, DrApoE4 YouTube channel – short evidence‑based briefings on APOE4 and brain health; >50 episodes planned (Rapamycin News) Author, longevity‑medicine blog posts and patient newsletters (grantfrasermd.com) |
| Professional Memberships | American Academy of Anti‑Aging Medicine (A4M) • American College of Lifestyle Medicine • Australian Medical Association |
Note: Filler words have been removed, and sentences have been punctuated for clarity. Time‑stamps are approximate anchors.
00:11 – 00:55
“Good morning. It’s my first time lecturing in this hall, so let’s see how it goes. We have an overwhelming amount of longevity data; the challenge is to compress it into a practical initial consultation. Weird and wonderful interventions can come later, but first we need a structured approach.
A quick reminder about me: I’ve spent decades in acute care and now focus primarily on longevity medicine.”
00:55 – 02:35
“My consultation starts with a morbid question: What will kill or disable this patient? Leading causes of death: vascular disease, cancer, accidents, infection, stroke, lung disease, Alzheimer’s, diabetes, renal and hepatic failure. Leading causes of disability mirror that list. Our job is to mitigate these predictable risks and extend both health‑span and life‑span.”
02:35 – 05:00
“I collapse three big domains—vascular events, metabolism, and malignancy—into one prevention bundle because the interventions overlap: optimise lipids, homocysteine, omega‑3 index, blood pressure, insulin sensitivity, diet, exercise, visceral fat, and keep the patient away from cigarettes.
Genetics matter, but they explain only ~15 % of outcomes, so we check them without being distracted. For example, 9p21 basically guarantees symptomatic coronary disease by age 50 in men and 60 in women. If the family history is strong, I image early.”
05:00 – 06:10
“Screening reality check: only 30 % of cancers even have a screening test, and those tests catch just a fraction of cases. Mammography modestly reduces breast‑cancer mortality; colonoscopy is better but still misses plenty. Hence I use CT coronary angiography and, for cancer, a 3‑tesla whole‑body MRI (SimonONE is US $1,250 for head‑to‑toe with MRA). If we find coronary plaque or white‑matter disease, patients suddenly care about treating their lipids.”
06:10 – 08:05
“Infection kills more older adults than most realise; frailty is the amplifier. Maintain muscle. Same logic with trauma: sarcopenia plus osteoporosis turns a ladder fall into the beginning of the end.
Neuro‑cognitive decline is a personal interest—my YouTube channel is ‘Dr ApoE4’. I run inexpensive online neuro‑psych testing (CNS Vital Signs, about $50) and aim to start interventions 20 years before expected symptom onset. Forty‑two percent of today’s over‑55s are projected to develop dementia.”
08:05 – 09:45
“I normalise hormones lifelong unless a clear contraindication exists—sex steroids, thyroid, adrenal, sometimes GH analogues when IGF‑1 is low. Lifestyle pillars—exercise, sleep, stress, community—still underpin everything. Environmental exposures (moulds, metals, plastics) and chronic infections are routinely screened. Periodontal disease strongly correlates with dementia and coronary disease; we treat it aggressively.”
09:45 – 11:05
“We tune nitric‑oxide pathways for cardiovascular and men’s‑health benefits, address mitochondrial health (methylene blue, NAC‑glycine, etc.), and use senolytics judiciously—I’m not sold on dasatinib + quercetin for every patient. Supplement lists are kept tight; a hundred pills can cancel each other out.”
11:05 – 12:05
“Pharma corner: SGLT‑2 inhibitors plus GLP‑1 agonists show roughly a 70 % lower incidence of dementia in community datasets. Telmisartan is my first‑line antihypertensive and the only one I push to max dose because of PPAR‑γ effects. Rapamycin plus acarbose appears synergistic in animal work. Metformin’s pros are tempered by possible sarcopenia.”
12:05 – 14:00
“In a typical 60‑minute new‑patient consult I get through about 70 % of that list and mop up the rest in follow‑ups.”
(Q&A excerpt)
Q: Routine screenings rarely cut mortality—why would a full‑body MRI be different?
A: Stage‑4 cancers are lethal; stage‑1 are almost always curable. MRI picks things up small. We lack outcome trials, but waiting for RCTs means we’re both dead before publication.
Q: How often should scans be repeated?
A: If we see an abnormality, that region gets rescanned in a year. For low‑risk patients with clean scans: whole‑body annually and head‑and‑neck every 3 years between 50‑60, every 2 years after 60.
(Minor discussion on carbon‑monoxide and radon monitoring concludes the session.)
Dr Fraser outlines a risk‑first framework for longevity consultations:
Strengths
Limitations & Caveats
| Issue | Commentary |
|---|---|
| Evidence gap for routine whole‑body MRI. Early‑stage detection logic is compelling, but outcome data are absent; professional societies currently discourage screening MRIs outside research because of cost, incidentalomas, and unclear mortality benefit (ClearHealthCosts, Agency One). | |
| Radiation trade‑offs. CT coronary angiography delivers non‑trivial radiation; repeated scans may negate benefit in low‑risk patients. Risk‑stratified intervals are mentioned but not quantified. | |
| Over‑extension of pharmacology. Citing observational dementia reductions with GLP‑1 + SGLT‑2 combo risks post hoc fallacy; RCT confirmation is pending. | |
| Patient‑centred economics. Annual MRI plus genomics and advanced panels can run >US $3k/year—unaffordable for many. Cost‑effectiveness is not addressed. | |
| Generalisability. The framework is rooted in a North‑American private‑pay context; applicability to population health or publicly funded systems is limited. |
Overall Verdict
Dr Fraser delivers an engaging, clinically grounded blueprint that bridges emergency‑medicine scepticism (“avoid medical misadventure”) with proactive longevity care. The strategy excels at identifying actionable risks and motivating patient engagement. Its weak point is reliance on screening technologies whose net‑harm vs net‑benefit balance remains unproven. Clinicians adopting this model should incorporate shared decision‑making, disclose uncertainties, and stay alert to forthcoming evidence—especially around advanced imaging and pharmaceutical geroprotectors.
Is this using ChatGPT? Prompt?
That question was truly not that relevant nor useful …so tiny amounts of CO are good and come from heme breakdown which happens via heme oxidase, which is optimized by curcumin, sulforaphane and other other items.
This is nothing I plan to spend any time on, or add to my protocols - I already recommend people do the things that optimize this pathway, and yes tiny amounts of CO are needed - but the clinical utility of this being compared to the items we were discussing on the day seems minuscule.
A question on Klotho or Gamma PPAR or IGF-1 would seem much more relevant.
Hi
Really concise and helpful. I have a question- the advice to avoid PPIs is something my partner can’t do as he has Barrett’s Esophagus so is on them for life - can anyone advise of any strategies to offset the potential damage from these drugs?
Morgan
In regard to this question - if unavoidable - then mitigation includes measuring Vitamin B12, supplementing magnesium and using a calcium absorbed better in a low acid environment (such as calcium citrate).
Monitor bone density, Vitamin D measured and optimized, add Vitamin K2, wt bearing exercise, etc.
A broad spectrum probiotic is sensible.
Those would be the main items to mitigate long term use of a PPI.
Much appreciated- thank you!
Thank you Dr. Fraser for your discussion of 9p21. You said that if a woman has the risk allele she is just about guaranteed to have some cardiovascular disease by age 60.
I am 76 and am homozygous for the risk allele at 9p21 and also have several other genetic risk alleles per Promethease. I have family history. I have the beginnings of plaque on the “widowmaker”, CAC sore of 0.96, some evidence of plaque in the abdomen per scan that was looking for gall stones.
I do all the right things. Could always be better. Repatha and ezitimibe have brought APOB to 49 and Lp(a) down from 40 to 27. HDL to trigs and total ratios are good as trigs and LDL are low and HDL is very high. I take the supplements that I have read might help – and also metformin since the Repatha has nudged the glucose higher into prediabetic territory.
Would so appreciate any thoughts you might have about my residual risk from the genetics, even though I am working all the aspects of lifestyle. Since about 25% of people have “the heart attack gene”, (though they may not know it) I am certainly not alone in needing more information on what else I can do. Thank you!
I think that genetics are interesting and give some indication of whether someone is more or less likely to develop disease. My practice has moved from the traditional approach of getting cheap blood tests and then guessing to actually looking at whether one actually has formed disease.
A CAC is sadly a useless test. In one review 31% of significant cardiac events occur in individuals with a CAC of zero, and on CCTA of older adults with a CAC of 0 ~45% have significant plaque - it’s just not calcified. It is important to note that calcified plaque is low risk - the high risk is non-calcified and worse yet low density non-calcified.
The ApoB in the 40’s with Lp(a) mid range - not negative - but in a non-high risk zone is right where I’d usually be targeting. Also optimizing insulin sensitivity, vitamin D (50-70 range), homocysteine, omega 3 index ~8-10%, blood pressure with central BP in the 95-112 mmHg range are all sensible targets to minimize vascular disease progression. Lifestyle and exercise are also a big factor - working on driving up VO2 max into 90%tile or higher for age/gender adds benefit.
I just happened to run into this clip now (had missed it for some reason) and it is by far the best and most comprehensive review/explanation of aging and the things one needs to do to maintain good health well into old age (that I have ever read or watched/listened to). Thank you for posting @LukeMV and thank you @DrFraser for such a simple, short but wholesome video.