@alexchamp and I had a discussion regarding oils and a great question Alex ask was like “What is it in fatty food or oil more specific that increases the effective dose of rapamycin? Is it for example the omega 3 content or something else?”
This is a very interesting question! Because if we understand better what specific things are triggering improved absorption than probably this can also increase the absorption of other supplements, drugs and even nutrition in our food which we eat.
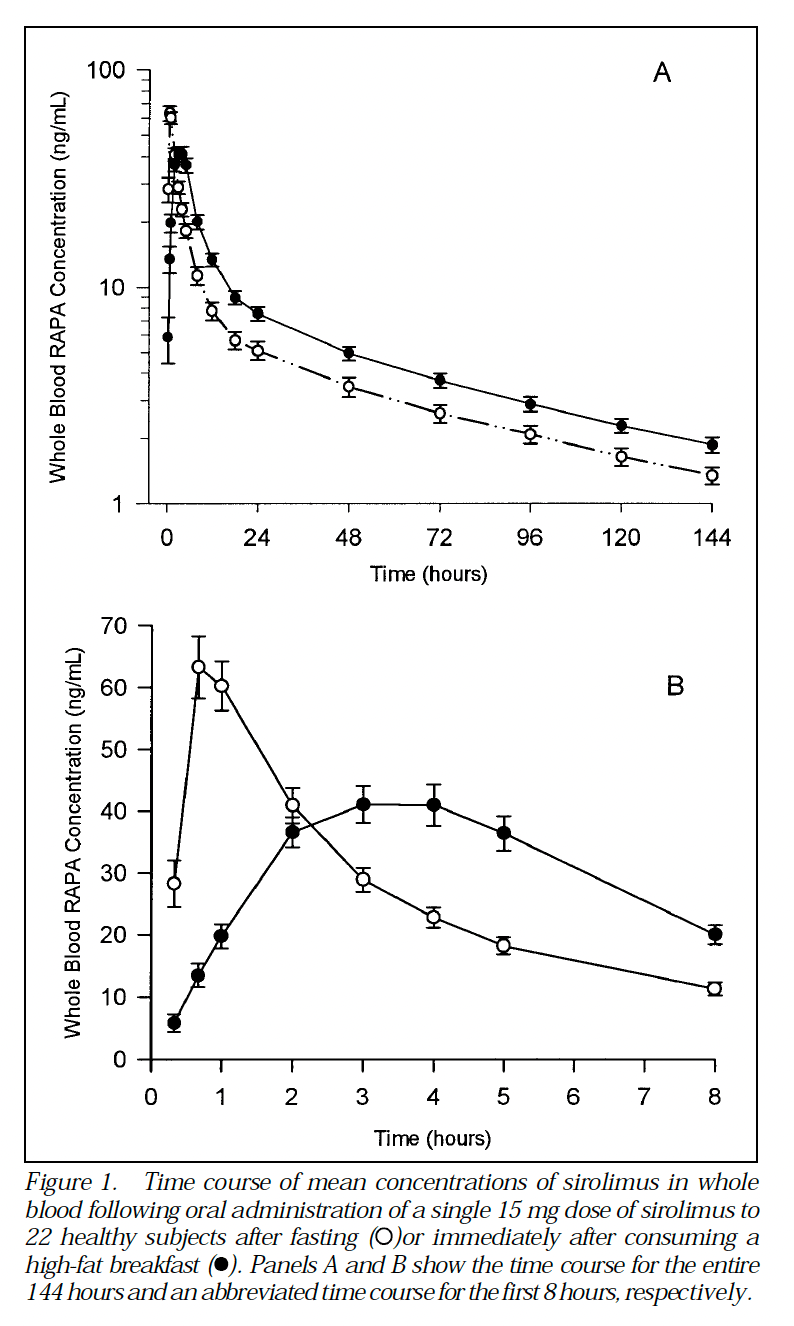
I know some rapamycin users take wild sardines to increase the absorption of rapamycin. Taking rapa with fatty food can increase the dose by 35% according to this study. The effect of a high-fat meal on the oral bioavailability of the immunosuppressant sirolimus (rapamycin) - PubMed
Do someone know if there are fats or oils that are better than other in increasing the absorption?
OBS! People like Alan Green and Mikhail Blagosklonny don’t recommend using fats or grapejuice for increasing the dose. One reason for this is that it’s hard to know what dose you get every time you take rapa. But my point with this discussion thread is more to understand the underlying mechanism behind why the absorption is increased by fatty food or oils. All feedback is welcome!