It might take you years but perhaps you’ll regrow some hair eventually ![]()
1 Like
Finasteride caused depression in me. Dutasteride doesn’t. So I’m using Dutasteride daily.
7 Likes
A single study. Multiple other studies show it is likely there.
I’ve seen no evidence on which you base this claim. There IS specific evidence in post-finasteride patients of persistent deficits in neurosteroids produced by 5ar type 1 in the central nervous system, which suggests that finasteride can in fact block or impair 5-ar type 1 specifically in the human brain, at least in a subset of patients. Perhaps, for instance, those with impairments in blood brain barrier function allow more finasteride into the brain? Either way, there’s evidence it CAN happen but no specific evidence that it can’t.
For references on epigenetics and long-term potentiation, I’m sure you can do a web search or two to read about them if interested.
2 Likes
MR studies are above observational trials in the pyramide of evidence.
I’ve seen no evidence on which you base this claim.
Did you somehow ignore the studies above? Sure I’ll post it again.
Only 5α-reductase 1 mRNA was expressed in human temporal lobe tissue; 5α-reductase 2 mRNA was not expressed. 5α-Reductase 1 mRNA concentrations did not differ significantly in the cerebral cortex of women [25.9 ± 7.9 arbitrary units (aU); mean ± sem] and men (20.4 ± 2.8 aU) or in the cerebral cortex (23.3 ± 4.4 aU) and the subcortical white matter of adults (32.6 ± 5.6 aU), but they were significantly higher in the cerebral cortex of adults than in that of children (6.4 ± 2.3 aU; P < 0.005).
There IS specific evidence in post-finasteride patients of persistent deficits in neurosteroids produced by 5ar type 1 in the central nervous system
No, you have people (recruited straight from the PFS forums) with preexisting conditions (depression amongst others) who supposedly have different values in the CFS than the normal population. Nowhere does that point to causality. And I doubt there are any studies showing downregulation of the 5ar type 1 pathway. But as I pointed out above, finasteride, in humans, may even upregulate the 5ar type 1 pathway.
which suggests that finasteride can in fact block or impair 5-ar type 1 specifically in the human brain
Or we take all the evidence from mechanistic studies, MR studies and clinical trials which strongly suggests that finasteride does not, in fact, affect the 5ar type 1 enzyme.
Perhaps, for instance, those with impairments in blood brain barrier function allow more finasteride into the brain?
Which then still does nothing. And especially does nothing after the two weeks it takes to leave the system.
Either way, there’s evidence it CAN happen but no specific evidence that it can’t.
No, the evidence suggests that PFS is not real. This is not even my own opinion but that of the Biden era FDA
According to the FDA statement, the PFS petition “does not provide reasonable evidence” of a causal link between finasteride and persistent SD, depression, or suicide. However, on the basis of reports from patients using the 1-mg dose for AGA, the FDA is “requiring the addition of SI and behaviour” to the listed AEs.
For references on epigenetics and long-term potentiation, I’m sure you can do a web search or two to read about them if interested.
I don’t think the bruden of proof falls on me when you’re the one inversing the pyramide of evidence.
This doesn’t bolster your claim that finasteride has no effect on 5-ar type 1 in the human brain. There is no way to know this other than doing a prospective clinical trial involving spinal taps. We have some observational evidence that it does, at least in a subset of patients.
Again I repeat, just because a drug is out of of the system doesn’t mean it necessarily has no lasting effect on neural pathways and neurohormones. I suggested reading about epigenetics and long-term potentiation in neurophysiology so that you’d be able to understand this.
There are no mechanistic studies in humans, just animal studies which show the opposite of what you’re claiming.
The one published MR study is encouraging, but there’s still more than enough uncertainty for me to continue warning patients before just handing it out like candy. But, you do you.
1 Like
As per your own AI, finasteride binds to 5ar type 2 100x stronger than to 5ar type 1. That explains why there is barely a difference in serum DHT suppression and hair growth with 1mg and 5mg finasteride.
I even found one of the original studies looking at the differences between finasteride’s effect on 5ar type 1 in rats and humans.
The 4-azasteroid 17~-(N-t-butyl)carbamoyl-4-aza-
Sa-androst-1-en-3-one (finasteride) is 100-fold more
potent as a competitive inhibitor of the rat NADPH:A4-
3-oxosteroid-Sa-oxidoreductase (steroid 5a-reductase)
type 1 enzyme (Ki = 3-5 nM) than of the human type 1
enzyme (Ki 2 300 nM). In this study, we exploit this
differential sensitivity to map a major determinant of
finasteride sensitivity in steroid 50-reductase.
There is no way to know this other than doing a prospective clinical trial involving spinal taps.
We don’t actually need to do that. We’ve established that a) finasteride is a selective 5ar type 2 inhibitor with its effects on 5ar type 2 being very, very weak to negligible, b) the human brain predominantly, if not exclusively, contains 5ar type 1, c) 5ar type 2 inhibition can potentially increase 5ar type 1 expression, and d) the use of finasteride is not causally connected to depression or neurological problems in both intervention studies as well as MR studies.
Again I repeat, just because a drug is out of of the system doesn’t mean it necessarily has no lasting effect on neural pathways and neurohormones.
There is no permanent downregulation of the 5ar type 1 enzyme. All studies have shown serum DHT levels going back to baseline. The few case reports on fertility also show male patients recovering within 3 months of ceasing treatment.
I suggested reading about epigenetics and long-term potentiation in neurophysiology so that you’d be able to understand this.
It’s your task to provide proof of persistent downregulation of 5ar type 1 with any 5ar inhibitor. I’m not aware of any study showing that effect.
There are no mechanistic studies in humans, just animal studies which show the opposite of what you’re claiming.
As we’ve established, finasteride in rats is a strong inhibitor of the 5ar type 1 enzyme. In humans it is NOT.
Data obtained after finasteride treatment showed that 186 genes (i.e., 171 up- and 15 downregulated) and 19 (i.e., 17 up- and 2 downregulated) were differentially expressed in the hypothalamus and hippocampus, respectively.
Were those changes associated with any kind of neurological effect? Also, why was there no control group in this study? Without a control group we can’t even establish causality for the changes in genes. Nor was the number of mice or their species given.
but there’s still more than enough uncertainty for me to continue warning patients before just handing it out like candy.
We have 30 years of clinical use in humans and the best thing the finasteride haters can come up with are animal studies at giga-doses that are proven to not even work the same mechanistically in humans. I think finasteride should be given to any man who wants it because the alternative is becoming bald and getting prostate cancer.
[quote=“DeStrider, post:182, topic:10688”]
Finasteride caused depression in me. Dutasteride
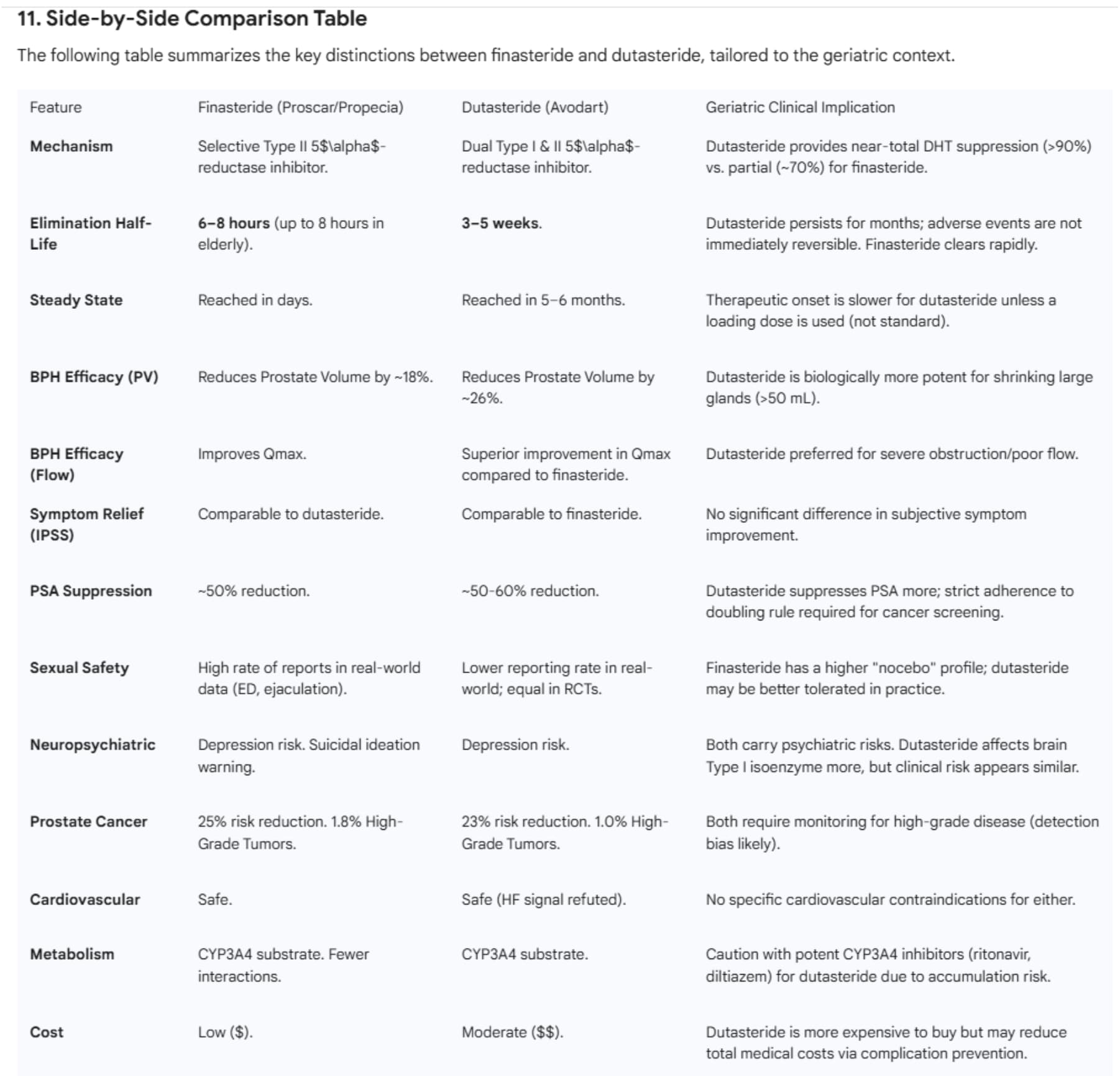
[/quote] Side-by-side comparison of finasteride and dutasteride with a focus on older men. Gemini Pro & ChatGPT 5.
I used finasteride for several years and was happy with the results. I switched to dutasteride about a year ago because it is somewhat superior to finasteride.
One difference is the superior urine flow produced by dutasteride.
“A meta-analysis of 8 randomized controlled trials demonstrated dutasteride’s statistically significant superiority over finasteride in improving maximum urine flow.” [ref]
How this usually plays out for an older man
- Either drug is reasonable for BPH when the prostate is enlarged and the goal is shrinking the gland / reducing progression risk over time. FDA Access Data+1
- Dutasteride tends to produce greater DHT/PSA/prostate-volume suppression on average, but symptom differences are often small. PMC+1
- The main tradeoff is side effects vs benefit, especially sexual and quality-of-life effects, which matter a lot in older men with baseline ED or low libido. PubMed+2FDA Access Data+2
- Because both lower PSA and may affect detection patterns of prostate cancer, it’s important that PSA is interpreted in the context of 5-ARI use (don’t “DIY” interpret PSA changes). FDA Access Data+1
5 Likes
I’ve got better things to do with my time than continue going round and round about this. Good luck on your crusade.
1 Like
On thing I’ll concede to you is that male mice should probably not take finasteride ![]()
3 Likes
@Virilius, @Davin8r, @Shady, thank you for your opinion. Let me try to summarize:
- Finasteride is clearly type-2 selective, but type-1 inhibition is not “zero,” just weaker, and species differences make rodent brain data easy to misapply to humans. (PubMed)
- The CSF neurosteroid studies show real differences in a tiny, selected symptomatic group, but are not strong enough to prove causality or prevalence. (Pubmed)
- Large-scale epidemiology is mixed-to-null on average (meta-analyses/MR/cohorts generally don’t show a big causal effect), but pharmacovigilance and regulators support that psychiatric adverse effects can occur, especially signals in younger alopecia users. (Pubmed, Reuters)
- The most defensible position is: most users won’t have severe psychiatric effects, but a small vulnerable minority may, and the mechanism is not conclusively proven.
4 Likes
What does it mean for those, who want to minimize possible side effects? Finasteride is far more selective for 5α-reductase type 2 than type 1, but at typical exposure it may still cause small, partial 5AR1 inhibition.
Hypothesis 1: in a susceptible minority, even mild 5AR1 “throttling” could reduce 5α-reduced neurosteroids (ALLO requires the 5α step), consistent with small CSF studies showing lower downstream 5α-reduced steroids with altered upstream profiles in symptomatic post-finasteride cohorts.
Hypothesis 2: If 5AR1 isn’t fully blocked, adjuncts might help by driving flux through remaining capacity:
- PEA (PPAR-α) can stimulate ALLO synthesis in preclinical models and its effect is blunted - not abolished - by finasteride, matching a “residual-enzyme amplification” model;
- pregnenolone may help only if substrate is limiting, but can also accumulate upstream when the 5α step is rate-limiting.
Any objections?
3 Likes
There is no controversy over the assertion that finasteride reduces the rate of low grade cancers. Is dutasteride better? It has a longer half life, so it could be taken weekly or bi weekly. The only question is regarding high Gleason cancers, and that may simply be the result of increased detection rate for those on the drug. Is that a fair summary of where we stand?
3 Likes
For those who have no issues with depression or ED on finasteride/proscar… it is a great molecule for reduced prostate size, protection from prostate cancer, clears cholesterol from the blood and my original reason to start at age 33… keeps your hair. On 5mg daily for 3 decades.
If it works with your phenotype - fantastic stuff. ![]()
Almost 68 years old… enjoying that prostate the size of a walnut… like a guy in his 20’s. I wish everyone could have that kind of benefit.
7 Likes
I think PFS is another topic altogether because persistent downregulation of the 5ar type 1 enzyme hasn’t been shown yet in studies. The mice study regarding methylation patterns can be discarded because it lacked a control group so any methylation pattern changes could be attributed to anything (not that methylation changes have clear outcome data to begin with).
- PEA (PPAR-α) can stimulate ALLO synthesis in preclinical models and its effect is blunted - not abolished - by finasteride, matching a “residual-enzyme amplification” model;
- pregnenolone may help only if substrate is limiting, but can also accumulate upstream when the 5α step is rate-limiting.
Do those even make it into the human brain?
1 Like
I will wade in here with my own personal expieriences. My bias is that everyone who can take dutasteride should, it will lower your rate of prostate cancer and defend your hair. However I’ve had pretty awful experiences with both Finasteride and Dutasteride. Both make me feel really down, emotional and lacking motivation (sitting in the gym thinking “why do I have to lift this heavy thing again”). The brain fog was horrific, especially on Finasteride. In theory Dutasteride should have stronger side effects as it inhibits all the enzymes but in my experience Finasteride was much worse. It might be that “unbalanced” inhibition causes some imbalance in the brain, or the short half life causes issues with hormones bouncing up and down, or perhaps it’s because I took lower doses with Dutasteride as I knew I could get away with much less since it has full inhibition and a much much longer half life.
Anyway all emotion aside I can only say that as someone who is “pro” these drugs in the sense that I would absolutely take them if I could deal with the side effects, I am 100% certain it is damaging to the brain and libido and general mental health. I don’t think it’s reasonable to claim they don’t cause side effects. Side effects are always under reported and most of the users in the studies are old guys who can’t tell the difference between almost zero libido and zero libido ![]()
I do wish the people who can tolerate them well, and as I said I would love to be taking them too. My dad got prostate cancer a few years ago, luckily he got it early and is still in good health, so I have a stronger incentive than most to take them.
7 Likes
Short answers from Perplexity Pro, ChatGPT 5.2, and Gemini Pro.
Perplexity Pro:
“Yes. Dutasteride, like finasteride, reduces the incidence of mainly low‑grade (Gleason ≤6) prostate cancers, with little or no benefit for high‑grade disease and a small signal for more Gleason 8–10 tumors in some analyses.” ref1, ref2, ref3.
Ref3 indicates a small increased risk in more aggressive forms of prostate cancer.
Link to full report: link1
ChatGPT 5.2:
"Yes—dutasteride shows the same general pattern as finasteride in the big prevention-style trials: it reduces the diagnosis/detection of lower-grade (low-risk) prostate cancers, while raising concern (at least on paper) about a small increase in high-grade cancers. ref4
Important nuance: (applies to both drugs) The FDA’s summary of the finasteride (PCPT) and dutasteride (REDUCE) data is essentially:
- Fewer overall prostate cancers, driven by fewer low-risk cancers
- But an observed increased incidence of high-grade prostate cancer in both trials, which is why neither drug is FDA-approved “to prevent prostate cancer.”
Link to full report: Link2
Gemini Pro:
"Primary Endpoint: Overall Cancer Reduction
Dutasteride treatment resulted in a statistically significant reduction in the incidence of biopsy-detectable prostate cancer.
Relative Risk Reduction (RRR): The relative risk of a prostate cancer diagnosis was reduced by 22.8% in the dutasteride arm compared to the placebo arm (p < 0.001) over the 4-year study period.
Absolute Incidence: Cancer was detected in 19.9% (659 of 3,305) of men in the dutasteride group versus 25.1% (857 of 3,424) of men in the placebo group.
Absolute Risk Reduction (ARR): The absolute risk reduction was approximately 5.1%. This implies a Number Needed to Treat (NNT) of roughly 20 to prevent one case of prostate cancer over 4 years."
PSA Performance: Dutasteride improves the performance of PSA. A rise in PSA in a man taking dutasteride is highly specific for cancer (often high-grade), whereas a rise in a placebo patient is often just BPH. This leads to more “efficient” biopsies in the treatment arm."
Conclusion on Mortality: Dutasteride does not appear to reduce mortality from prostate cancer, nor does it increase it. The reduction in low-grade cancer incidence translates to a reduction in morbidity (fewer biopsies, fewer surgeries for indolent disease) rather than a survival benefit. ref4, ref5, ref6, I did not include all of the references. You can find them in the full report: Link3
Bottom line: There is no reason IMO to take finasteride or dutasteride for cancer reduction. What they do quite well is reduce the size of the prostate and allow you to pee better and reduce the number of times you have to get up in the night to pee. IMO, dutasteride does this better than finasteride. Personally, I have detected no side effects from either drug. Do they grow hair? That is a matter for another thread.
3 Likes
I am 100% certain it is damaging to the brain and libido and general mental health. I don’t think it’s reasonable to claim they don’t cause side effects. Side effects are always under reported and most of the users in the studies are old guys who can’t tell the difference between almost zero libido and zero libido
I get side effects from most statins. Yet I don’t go around claiming that all studies are fake and statins cause side effects in 100% of people because I know I’m just part of the ~5% whose biology doesn’t agree with them. Our individual experience is not universal truth. And anecdotes on the internet can’t be trusted in most cases for various reasons.
Besides, both the placebo and treatment group would over- and underreport side effects to the same degree so it evens out. Clinical trials don’t just ask “hey man you’re on finasteride do you feel side effects” (at least not the ones used for litigious causes). Finasteride causes side effects at 1-3% over placebo so while side effects are real, they tend to be overstated.
2 Likes
Bottom line : There is no reason IMO to take finasteride or dutasteride for cancer reduction
But your response was just for dutasteride. We do have studies looking at finasteride’s effect on prostate cancer rates and here it showed a statistically significant reduction.
The study’s primary end point — the prevalence of prostate cancer during the 7 years of the trial — was met: the relative risk of prostate cancer with finasteride was 24.8% lower than the risk with placebo.1 Paradoxically, the risk of high-grade cancer (Gleason score of 7 to 10) was higher with finasteride, a finding that led to recommendations against the use of finasteride for the prevention of prostate cancer. Subsequent trials showed that finasteride improved detection of prostate cancer and high-grade prostate cancer by improving the performance characteristics of the prostate-specific antigen (PSA) test, digital rectal examination, and the prostate biopsy. These biases could explain the paradox, but the questions of whether the greater number of high-grade prostate cancers could have led to diminished survival or to an increase in prostate cancer mortality persisted.
Long-Term Effects of Finasteride on Prostate Cancer Mortality | New England Journal of Medicine
It’s just that not enough men die of prostate cancer so those relative reductions don’t translate into a statistically significant mortality benefit overall.
With 296,842 person-years of follow-up and a median follow-up of 18.4 years, of 9423 men randomized to finasteride, there were 3048 deaths of which 42 were due to prostate cancer; of 9457 randomized to placebo, there were 2979 deaths, 56 due to prostate cancer. With the small number of deaths due to prostate cancer, the 25% lower risk of death from prostate cancer with finasteride was not statistically significant.
Yes, but the absolute risk reduction is 5%, or 1 person in 20. Yes, statistically significant but not a reason to take either one. There are a plethora of drugs and supplements that reduce cancer risk. I would not consider this to be the main reason for taking finasteride or dutasteride.
1 Like
Hello SilentWatcher,.
First of all, thanks for the info. I will look into M. oleifera, as I have not heard of it before. I was put on finasteride by my previous Dr. The main reason was to hopefully shrink my prostate. He also mentioned that it reduced cancer risk by 20+ %. I was on a high dose - 5 mg/day - so I discontinued it due to sex side effects. Not sure if a lower level would still have protective aspects. If so, I may go back on it. Both my Dad and his father had prostate cancer, so I likely have a significant genetic predisposition. I am also getting close to the age that my Dad’s cancer was discovered. My PSA jumped from 1.51 to 1.98 in a year. My current Dr. didn’t think it was a big deal, but I have subsequently read that a jump of 0.35 or more should be looked into.
Thanks again for the info, and please let me know anything else you may discover.
Best Regards
1 Like