Muscle loss from improper GLP1 usage is causing pharma companies to look for new drugs to help preserve and build muscle. Bodybuilders must be cheering lol.
6 Likes
Hi @Steve_Combi
I always find your posts very informative! I would rate the first 2 items the same as you. I don’t have experience with the growth hormone secretagogue peptides myself. I also tend to go with the Glow version on item (2) → BPC 157 + TB500 + GHK-cu (10+10+50).
On item (2) given continuous use do you worry about any cancer growth risks; specifically some worry about cancer with BPC under continuous use?
BCP+TB500+GHK-cu is amazing for recovery on a day to day basis imho but I currently cycle its use (2 weeks on - 4 weeks off) due to potential cancer worry.
1 Like
That is a good question and the way you have phrased it is interesting, “growth risk” being the key aspect of the question.
My take away from the available studies is that it may or may not enable growth of existing cancers. I don’t see any papers suggesting it would initiate new cancer. It, BPC, and other peptides that promote angiogenesis would all have the same concern, as that is where the “influencer” speculation lies.
There is no proof that BPC would support cancer growth that I know of. In fact, just the opposite is what appears in a few papers.
1 Like
I have posted my thoughts on non-GLP1 peptides in this thread Peptides / Bioregulators - #763 by Steve_Combi
@Steve_Combi how is your soreness level on this protocol? Have you noticed any difference in terms of recovery when on vs off protocol? As I’ve progressed in my weight lifting, I’ve gotten more and more soreness (DOMS), even with proper recovery.
Somewhat unrelated: Have you looked into GHK-cu as a possible intervention to retain muscle? It’s considered mainly a cosmetic peptide, but I think its benefits may go beyond being the maiin ingredient of GLOW. I’ve come across this interesting paper on its use for skeletton muscle dysfunction in rats:
https://onlinelibrary.wiley.com/doi/full/10.1002/jcsm.13213
Mechanistically, GHK-Cu directly binds and activates SIRT1(the binding energy was −6.1 kcal/mol). Through activating SIRT1 deacetylation, GHK-Cu inhibits FoxO3a transcriptional activity to reduce protein degradation, deacetylates Nrf2 and contribute to its action of reducing oxidative stress by generation of anti-oxidant enzymes, increases PGC-1α expression to promote mitochondrial function. Finally, GHK-Cu could protect mice against CS-induced skeletal muscle dysfunction via SIRT1.
Conclusions
Plasma glycyl-l-histidyl-l-lysine level in patients with chronic obstructive pulmonary disease was significantly decreased and was significantly associated with skeletal muscle mass. Exogenous administration of glycyl-l-histidyl-l-lysine-Cu2+ could protect against cigarette smoking-induced skeletal muscle dysfunction via sirtuin 1.
Big difference. I think that because we’ve been doing the BPC+TB500 stack almost every day for 20 months, with several 1 week breaks, we are primed to heal.
I’ve posted on this before, I recover from hard work overnight.
I have several gym rats, including our 41 y/o son who also experiences rapid recovery and healing and misses that benefit when we have an off week. He has gained about 8lbs of muscle since this photo and lost 5lbs of fat. He’s around 185lb. All while on a weekly dose of 1.5mg Reta
I have not tried GHK-cu as an injectable but I’ve been making a skin care product with that peptide for over 3 years and have a lot of local repeat customers. It works!!
I do take other peptides that support mitochondria.
This thread has a lot more info on a wider range of peptides.

2 Likes
We established a theoretical model for how the modulation of GLP-1 agonists via increased serotonergic activity at the 5-HT2C receptor may have an associated negative effect on sexual desire. We then applied a biopsychosocial framework to highlight why this effect may be overlooked by both GLP-1-treated patients and clinicians. Although the serotonergic pathway may create a physiological decrease in sexual desire for patients taking GLP-1 agonists, the biopsychosocial factors discussed propose a potential mechanism by which these adverse effects are masked. In other words, we postulate that the negative influence of GLP-1 agonism on sexual desire, mediated by serotonergic pathways, as well as undesirable facial effects (“Ozempic Face”) and increased SHBG, etc., are offset by the positive influences on sexual desire such as increased total testosterone, improved vascular reactivity, and a more positive mood.
FWIW…
2 Likes
https://www.nejm.org/doi/full/10.1056/NEJMoa2413258
Resolution of steatohepatitis without worsening of fibrosis occurred in 62.9% of the 534 patients in the semaglutide group and in 34.3% of the 266 patients in the placebo group (estimated difference, 28.7 percentage points; 95% confidence interval [CI], 21.1 to 36.2; P<0.001). A reduction in liver fibrosis without worsening of steatohepatitis was reported in 36.8% of the patients in the semaglutide group and in 22.4% of those in the placebo group
Old semaglutide still has some tricks up its sleeves
1 Like
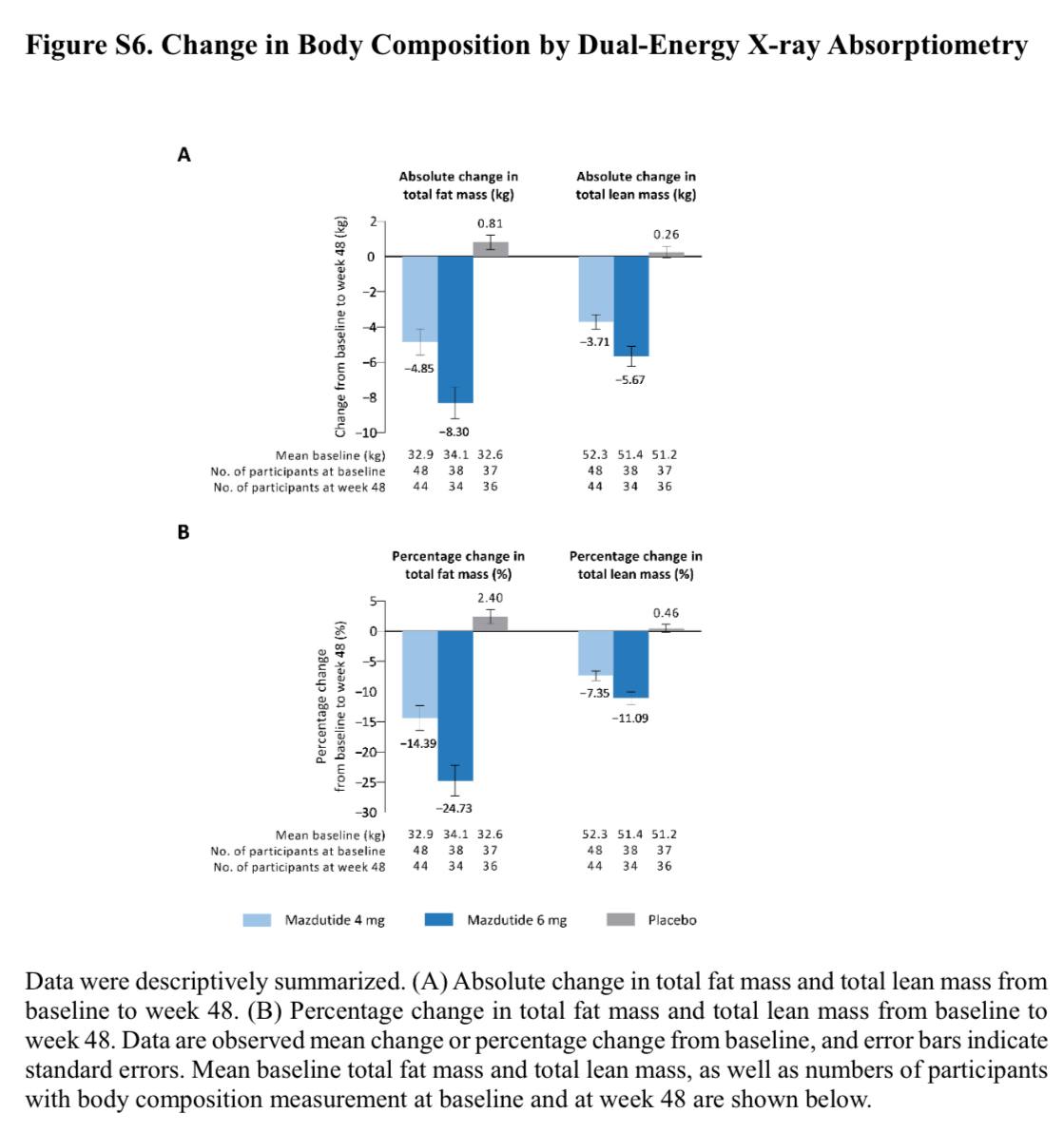
Phase 3 trial data is now available for mazdutide, a GLP1, GCGR (glucagon receptor) agonist :
https://www.nejm.org/doi/full/10.1056/NEJMoa2411528
One concerning data point is that 41% of weight loss seems to come from lean mass, according to dexa scans.
2 Likes
I think there is a general issue with the loss of lean weight mass with fat going. It needs a proper resolution rather than ending up with lots of thin really frail older people.
2 Likes
This is phase 3 trial for maz, not phase 2.
1 Like
Mazdutide is a product of China, and the focus of this GLP1 RA has been tailored to the challenges of obesity and cardiometabolic disease in the Chinese population
Our trial participants were relatively young with a high prevalence of weight-
related cardiometabolic diseases, most notably dyslipidemia (in 62.3%), MAFLD (in 48.9%), hyper-
uricemia (in 40.2%), and hypertension (in 22.8%). Our results are consistent with results of a re-
cent study involving young Chinese adults, which showed an alarmingly high prevalence of the
same weight-related cardiometabolic conditions.
Our trial population differs from that of other trials to date. China adopted lower BMI cutoffs
for overweight and obesity than those used by the World Health Organization.
Some nice results:
In participants with liver steatosis, mazdutide treatment for 48 weeks appeared to be associ-
ated with a greater reduction in liver-fat content than placebo, and more participants who received
mazdutide had relative reductions of 30% and 50% in liver-fat content and a liver-fat content of
less than 5% at week 48 than those who received placebo
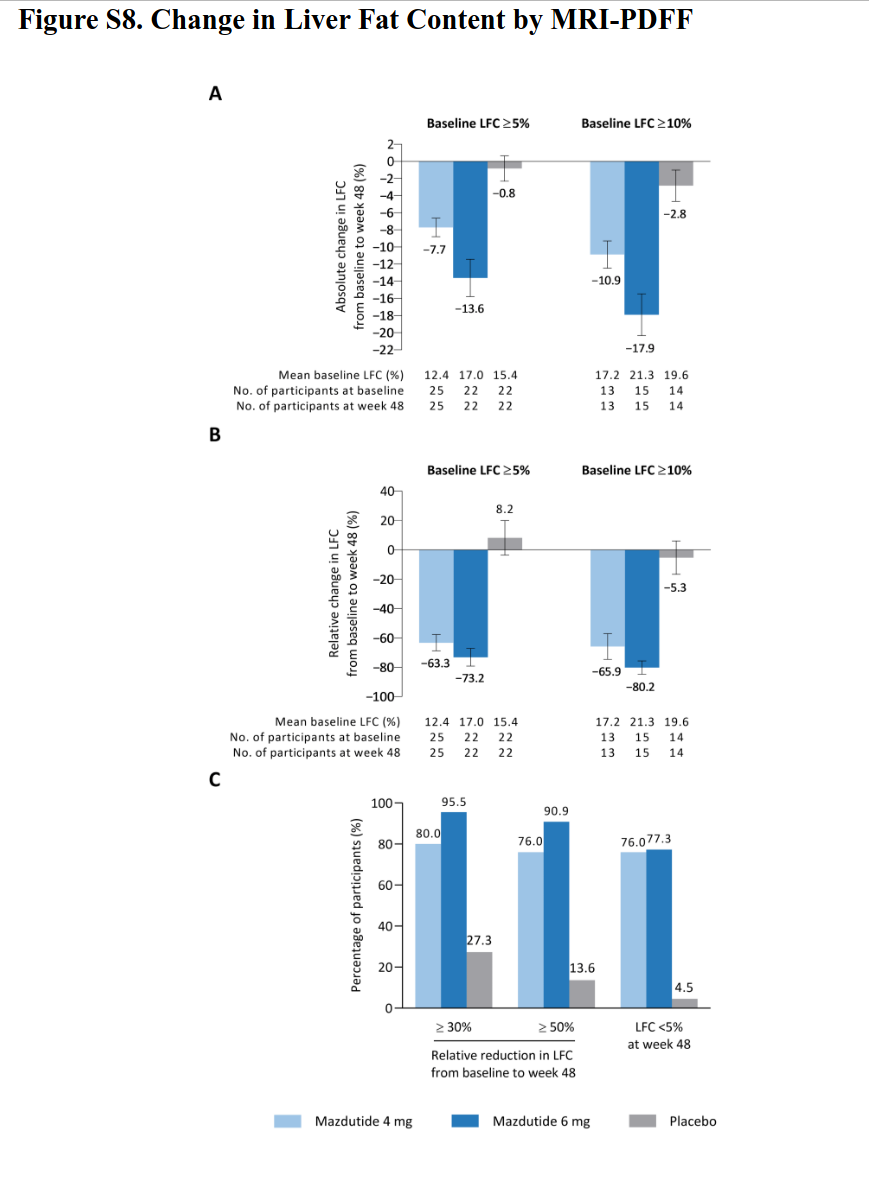
This reduction in liver fat content is probably due to GCGR
The potential and unique metabolic effects of mazdutide that differentiate it from GLP-1 recep-
tor agonists and other GLP-1–based dual agonists appear to stem from glucagon agonism. Al-
though a head-to-head comparison of mazdutide with GLP-1 receptor agonists is important for a
firm conclusion, we speculate that the seemingly more-pronounced overall improvements in lipid
metabolism, such as reductions in triglyceride and alanine aminotransferase levels and most
notably in liver-fat content, may be attributable to glucagon-driven lipid oxidation in the liver
and in adipose tissue.12 These observations may be important, given the high prevalence of fatty
liver and dyslipidemia among Chinese adults with obesity or overweight.
Not disagreeing, but this is not an issue specific to GLP1 medication, and the solution is simple: resistance training 2-3 times a week. But we all know simple doesn’t mean easy.
2 Likes
DEXA scans themselves has limitations to keep in mind:
- cannot distinguish between different muscle groups (e.g., deep vs. superficial muscles) or identify intramuscular fat
- DEXA relies on tissue density, so changes in hydration can artificially alter lean mass readings.
- In some cases, it classifies water or glycogen stores as lean mass. It’s important to keep in mind that some percentage of weight loss is water weight loss, which impacts lean mass readings negatively. So your muscle tissues has less water in them, but you haven’t actually lost muscle weight
- DEXA only tells you about lean mass, not actual muscle mass. Lean mass includes water, tendons, bones.
The gold standard is MRI, and hopefully there will be studies where we can get more precise readings on fat vs muscle mass loss.
1 Like
That’s true. The solution is exercise related, but it is a real issue. I think there is also a satellite cell issue.
1 Like
Hey Steve! I saw a couple of posts where you commented about peptides. I’m really interested in your journey and learning more about your suppliers. Do you think we can connect?
A study recently published in Frontiers of Nutrition found that individuals on GLP-1 therapy had insufficient intakes of key nutrients like fiber, calcium, iron, magnesium, potassium and vitamins A, C, D and E.
Most patients who are prescribed GLP-1 receptor agonists do not receive appropriate nutritional counseling, despite the known benefits, so the advisory “seeks to fill that gap with practical, interdisciplinary guidance for implementation in clinical practice,” according to a press release.
The advisory stresses the importance of:
- careful baseline nutritional assessment;
- maximizing weight reduction with a good diet;
- patient-centered initiation of therapy;
- personalized diets that are minimally processed and nutrient-dense;
- lean mass preservation via strength training and adequate protein intake;
- gastrointestinal adverse effect management;
- micronutrient deficiency prevention; and
- promoting other positive lifestyle changes in several areas — like sleep, exercise, substance use, mental stress and social connections — to ensure long-term success.
4 Likes
This is not rocket science thankfully, and it’s been done before. Before GLP1 therapy, people used to lose massive amounts of weight through bariatric surgery. The after care program, and concerns from those surgeries look very similar to what’s been proposed here for GLP1 therapies. It’s well-known that these patients have to be on multivitamins, multiminerals, and in some cases add extra iron, calcium, magnesium, zinc, etc.
2 Likes
Confirmation of the suicide ideation risk with semaglutide: Depression and suicide/self-injury signals for weight loss medications: A disproportionality analysis of semaglutide, liraglutide, and tirzepatide in FAERS database 2025
Analysis included 8284 reports for liraglutide (n = 3022), 14,435 for semaglutide (n = 4233), and 15,597 for tirzepatide (n = 5722). Significant signals were identified only for semaglutide in both depression (ROR, 1.87; 95 % CI, 1.60–2.20) and suicide/self-injury events (ROR, 1.73; 95 % CI, 1.46–2.04). Effects were consistent across sex groups but most pronounced in ages 18–64. Post-weight management approval saw increased reporting, particularly in European and North American regions. Tirzepatide showed significantly lower mortality rates (0.26 %) compared to other agents.
Findings identified significant depression and suicidality signals with semaglutide in weight management. For patients requiring weight reduction therapy, particularly those with psychiatric comorbidities, tirzepatide may represent a more appropriate choice based on its superior safety profile.
7 Likes
Sadly, the large majority of people on GLP1’s are too lazy to work out and still eat junk. They just eat much less junk as a result of their appetites being suppressed, hence the weight loss. So given the fact they’re not eating much but are still eating junk whenever they do, they’re more likely to be deficient in just about everything. These people need a quality multivitamin more than anyone, but few are taking one.
On the other hand, if someone uses a GLP1 in addition to a healthy diet and good exercise program, they should be able to avoid deficiencies.
4 Likes