I guess chewing and swishing results in something like a sublingual administration which may be the reason for the quick effects. But yeah, i don’t know what happens in the stomach.
1 Like
Did you ever contact them? What did they say?
1 Like
I have not yet ordered any everolimus or spoken to Life Extension about the potential for a lower cost version of the everolimus blood test.
Last year when I emailed them about the sirolimus blood test I just contacted them as a concerned customer… so if anyone is interested in a lower cost everolimus blood test i encourage you to contact them and tell them there is a growing interest and demand in this test, just like the blood sirolimus test. Here was my original contact effort towards their lab customer support: How to get a Rapamycin (sirolimus) Blood Level Test
2 Likes
Oh — really? You were indicating you would do so back last summer. What changed your mind or caused you to delay commencement?
1 Like
I ended up getting into the plasmapheresis clinical trial which lasts until this month - so I’ve paused my rapamycin / everolimus during the trial. will restart next month.
3 Likes
It’s true that the great majority of lifespan studies used continuous dosing. However, there is exactly one mouse study with a protocol similar to the once-weekly-type protocol used in the Lamming 2014 glucose tolerance study (which you quoted from above) and also used in the Mannick everolimus human trial (which is the best available evidence for a potential anti-aging effect in humans):
Intermittent Administration of Rapamycin Extends the Life Span of Female C57BL/6J Mice
Sebastian I. Arriola Apelo, Cassidy P. Pumper, Emma L. Baar, Nicole E. Cummings, Dudley W. Lamming
The Journals of Gerontology: Series A, Volume 71, Issue 7, July 2016, Pages 876–881,
We recently identified an intermittent rapamycin treatment regimen—2mg/kg administered every 5 days—with a reduced impact on glucose homeostasis and the immune system as compared with chronic treatment; however, the ability of this regimen to extend life span has not been determined.
Here, we report for the first time that an intermittent rapamycin treatment regimen starting as late as 20 months of age can extend the life span of female C57BL/6J mice.
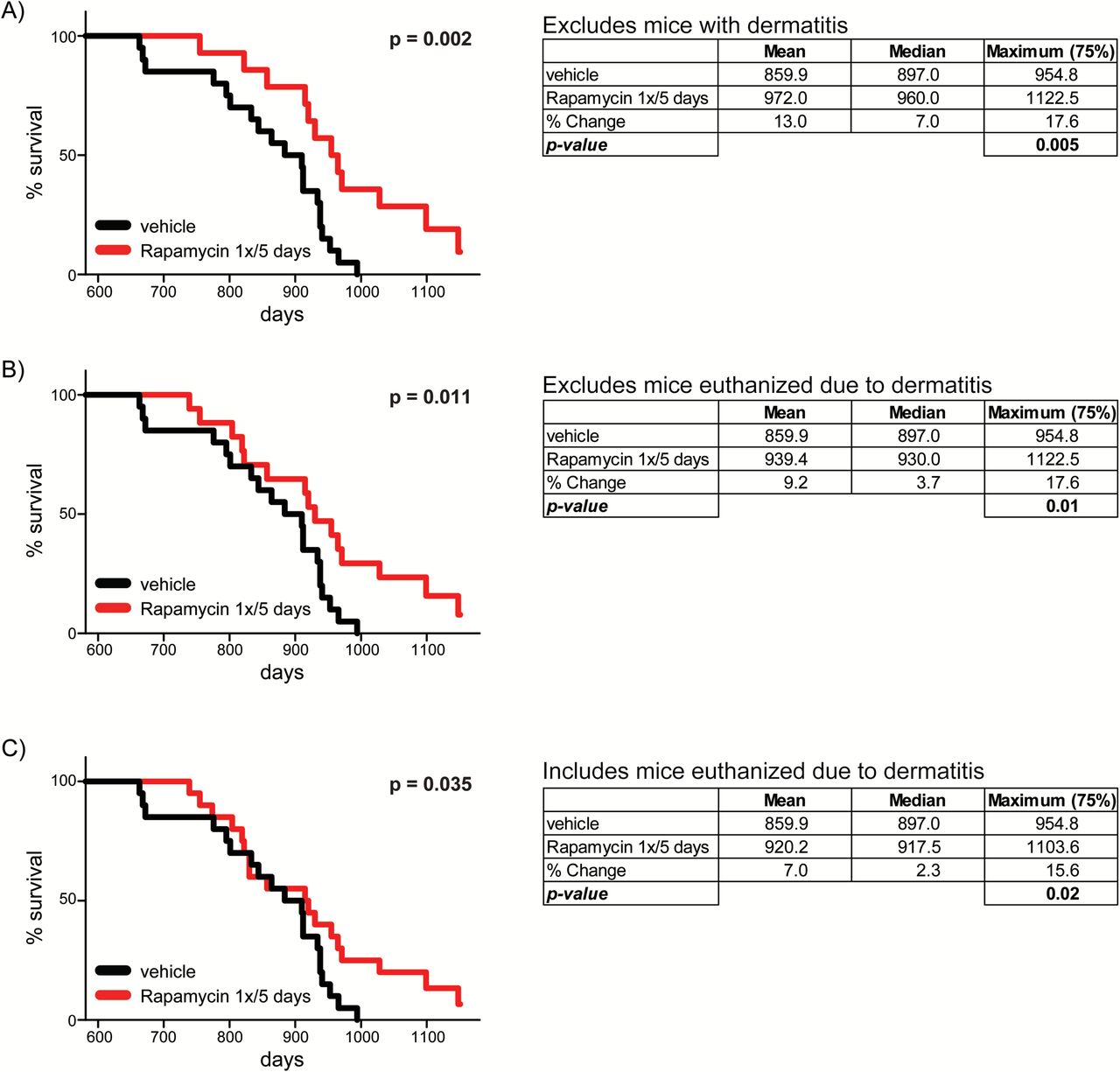
A lot of caveats come with that result, the most important of which are:
- these are all female mice (lady-mice do better on rapa than boy-mice), so it might overstate what you would see in males; and
- There were only 20 mice in the vehicle-treated and no more than 20 rapamycin-treated mice (up to 6 rapa mice were excluded in (a) and (b)), which is not nearly enough to give a reliable lifespan result.
5 Likes
Yes - Jane Mannick has said that they just used this protocol and study as a basis for their own human clinical study.
1 Like
You mean the just-cited lamming study? The first Mannick trial was in 2014, and this study was in 2016. The earlier glucose study by Lamming was in 2014, but it doesn’t seem plausible that they would have turned their doses for a clinical trial around that quickly.
1 Like
Yes, you caught that critically important distinction: “we report for the first time that an intermittent rapamycin treatment regimen starting as late as 20 months of age can extend the life span of female C57BL/6J mice”. The study makes no reference to male mice.
Chronic rapamycin treatment extends lifespan of both male and female mice. But clearly, from this study, and others, there is sexual dimorphism in some longevity interventions, likely connected to hormonal biology (eg.17α-Estradiol)
1 Like
That seems an oversimplistic way to do a dose-conversion: they were just measuring how much drug it took to get the same trough blood concentration of either drug. But each drug has different pharmacokiinetics beyond the trough concentration, and also different pharmacodynamics (e.g., differences in mTORC1 vs. mTORC2 inhibition at a given concentration and a given time of exposure) and tissue selectivity (e.g. everolimus has greater access to the brain). So just saying how much of either drug you have to take to get steady-state 12-15ng/mL of each is not likely very meaningful.
3 Likes
Agreed. As the “Everolimus and Sirolimus in Transplantation-Related but Different” paper from 2015 said:
Although binding of everolimus to FKBP-12 is approximately 3-fold weaker than that of sirolimus [19], everolimus blood trough concentrations targeted in transplant patients are typically lower than for sirolimus (3–8 ng/mL versus 4–20 ng/mL [24–26]).
2 Likes
According to Joan Mannick (25:31), everolimus is equivalent to rapamycin.
And that you actually can take a lower dose of everolimus to get the same treatment effect as rapamycin. Meaning you get higher levels at the same dosage.

@RapAdmin what if people have taken twice the dosage of everolimus thinking it’s half as effective but it is actually more potent ![]()
5 Likes
Everolimus seems to be used as a cancer drug rather than for immunosuppression and for organ transplants. Rapamycin doesn’t seem to be used for that, at least much. It can stop the growth of certain cancers.
Brand name Afinitor.
I’m thinking another positive with everolimus, is that the scientists behind it spent a lot of money, effort, and time, to create a rapamycin alternative. That process might’ve been intended to make a better alternative, and thus there is the chance they’ve succeeded.
2 Likes
I would think that the uncertainty with Everolimus is greater than Rapamycin.
2 Likes
Why do you think that? Everolimus has been used in the only clinical trial to show weekly dosing being safe / improving aging (possibly reversing immunosenescence)? It was developed in the 90’s, a looot of clinical trials has used it.
1 Like
Well… there have been many dozens of lifespan tests done with rapamycin, and few if any with everolimus. So just from that data, we have more confidence that it produces favorable longevity results.
I tend to think that the molecule is so close to rapamycin that effective differences in results will be minimal. But - we don’t know for certain until testing is done. But - given the opinion of Richard Miller and other experts who don’t think its worth even testing everolimus for longevity (because they feel its likely to be identical (or very close) results to rapamycin and thus wasted time and money - I tend to go with the opinions of the experts.
7 Likes
I think there is a lots more data on Rapamycin. In some senses once a lot of people are taking something if it causes any problems then we are more likely to know.
However, I have not tried to do a complete summary of who has taken what.
1 Like
Good morning, questions for the this great group of very intelligent people. I have a very small 6 pound 12 year dog… he is currently on the smallest dose of Rapamycin .5 mg available Dr Kevin has me dosing 1x per week because of his weight. He is doing well at this dose but I really haven’t seen many benefits. I was hoping to dose more frequently so was looking into Everolimus. Which is available in .25mg I understand that that is less of a dose than .25 rapa would be. I also remember reading that unlike Rapa the Everolimus an be split?
What would you do if this was your baby? Leave him on the once per week Rapa? Switch to Everolimus dose more often? The .5 Everolimus is cheaper if I buy and split.
Suggestions please
1 Like
I’m assuming you are treating for longevity and not cardiomyopathy. Since we really have minimal longevity data in dogs on rapamycin, I’d try to mimic Kaeberlein’s TRIAD trial and dose at 0.15 mg / kg (2.2 lbs/kg so 6 pounds = ~2.7 kg). Your dog’s dose would be 0.4 mg so the 0.5 mg dose he is getting is close enough. I’m not sure what benefits you are looking for as the effect will be to slow the aging process and the benefit will be slower aging and prolonged health rather than a dramatic reinstatement of youthfulness. At this point that’s probably the best you can do as there is some evidence that too high a dose can cause toxicity. More isn’t always better. Wait for the results of the TRIAD trial and adjust at that point if there is reason to.
2 Likes
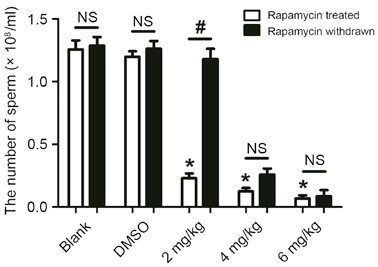
I wanted to soften the blow here with some details from the paper. They injected Sprague‑Dawley rats daily with 2, 4 and 6 mg/kg of rapamycin for four weeks. First, intraperitoneal injection has a much larger effect than the same dose taken orally. See, for example:
Second, daily injection would result in significantly higher levels of everolimus.
Third, for a 0.200 kg Sprague‑Dawley rat, rough allometric scaling to a human dose looks like this:
- 2 mg/kg = 0.4 mg ≈ 34 mg @ 75 kg
- 4 mg/kg = 0.8 mg ≈ 68 mg @ 75 kg
- 6 mg/kg = 1.2 mg ≈ 102 mg @ 75 kg
My takeaway: you would need to consume extremely large doses of oral everolimus every day (or two) for weeks to match the experimental design of this study. Since the rats in the 2 mg/kg group regained the usual number of sperm after a 24 week recovery, I suspect the long-term consequences of lower and intermittent dosing are minimal.
That being said, a 2015 paper from the Lamming lab showed reduced testicular weight from both the 1x/daily and 1x/5-day dosage schedules.
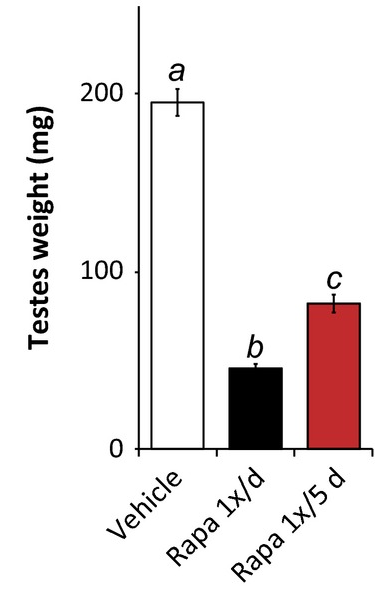
Still—my read on the literature so far suggests that these changes are temporary and revert to baseline after ceasing rapamycin (or everolimus in this case).
3 Likes