Some of the longevity drugs that work in mice probably help humans delay cancer.
2 Likes
Right. These however are not mutually exclusive. Even if longevity drugs don’t prevent modern lifestyle death and disease causes, they still work. Btw., true longevity drugs are supposed to work by slowing ageing, which delays these diseases, and there seems to be evidence that at least in animal models rapamycin does so. To me, rather than dropping longevity drugs, this is a reason to escalate the use of drugs that prevent or ameliorate these diseases, like statins and the like.
Rapamycin - or longevity drugs - are like a healthy diet, we know that a healthy diet leads to a longer life. But what if you live in an unsafe neighborhood, and there are regular shootings? Would you say “gee, I’m not going to bother with a healthy diet, because a healthy diet does not prevent my being shot”. The solution is to keep the diet and move your place of residence. Same here, just because rapamycin does not prevent modern lifestyle diseases (and I’d dispute that, at least in animals), doesn’t mean it makes sense to drop it. Dropping rapamycin will do nothing to cure heart disease, cancer or T2DM.
However, there is a much more interesting argument, brought up by Matt Kaeberlein. What if rapamycin both slowed down aging and killed you prematurely? That might very likely be the case. Now you truly have a dilemma… except the solution is very simple.
How can rapamycin delay aging and yet kill you way ahead of your natural time? Because while rapamycin slows down your aging, it also, especially at higher doses, might depress your immune system and you might die of an opportunistic infection. In lab animals you don’t see that, because labs take pains to shield animals from pathogens. So what’s the solution? Drop rapamycin? No, the solution is the same as with the diseases above. Retain rapamycin (although you might want to mitigate the danger with dosage), but get all the vaccinations you can for pathogens you might be exposed to, and minimize unnecessary exposure to such pathogens in the first place. Win-win.
Same with the diseases you mentioned. To me that’s a compelling argument for carefully curated polypharmacy. I take rapamycin, but I also take a bunch of drugs to ameliorate the chances of my getting these diseases: lipid lowering therapies (statin, bempedoic acid, ezetimibe etc.), blood sugar control (SGLT2i, soon pioglitazone, perhaps acarbose), blood pressure control (telmisartan down the line). Exercise and a good diet are a given - I’d do that regardless. It’s not an either or. I want maximum impact on healthspan and if lucky maybe even lifespan, and the first step is diet, exercise, stress and lifestyle adjustments. But that only takes me so far. The next tranch is taking medications proven to enhance healthspan or lower health risks: lipid control, blood glucose control, BP control and vaccintions. And then I roll the dice with a cherry on top: longevity drugs - thus far rapamycin, but we’ll see what science brings us in the future. I’m not dropping the longevity drugs just because other risks exist, I lower the other risks instead. Furthermore, we have evidence from the ITP that many of these work synergistically: rapamycin works even better with for example an SGLT2i, acarbose, metformin etc.
These lifestyle drugs (statin etc.), get me into the door of the casino. Rapamycin gets me some chips I can place on the roulette table. I for one am not going to reject the rapamycin gambling chips. I am gambling that I’ll come out ahead instead of going bankrupt, but that’s the nature of the game. YMMV.
EDIT: incidentally Matt Kaeberlein published a short on yt. contrasting short term vs long term effects of rapamycin in mice. Short term, there were metabolic derangements of glucose control, but longer term there was an improvement in these parameters compared to the baseline. A nice illustration of why it is important to focus on long term outcomes and not short term mechanistic perturbations in evaluating these drugs:
5 Likes
I go off and on but this is gonna make me resume taking estradiol
CCTA came back about as expected — stenosis under 70%. Not great, but not immediately critical. Triple lipid therapy might be the ticket.
I’ve got an appointment with an InstaLab cardiologist (Dr. S. Winiarski). He looks solid — apparently into longevity, so I can come clean and get his take on the whole medicine chest.
After the triple whammy — AK, CAC, and a pulmonary nodule — I paused E3 for a bit. Starting it back up this weekend. The nodule’s still lingering, so I’m holding off on rapa for now (not keen on immunosuppression until that’s resolved).
E3 isn’t noted for oncogenesis — didn’t hurt the ITP mice, even though they’re cancer-prone. But caution’s warranted. We’re still in early days here. Heck, E3’s umbilical cord hasn’t even been cut yet (pun very much intended; raw placenta anyone?
).
I’m liking the looks of InstaLabs — might spring for their monthly concierge plan.
2 Likes
Quick follow-up to my placenta quip (yeah, that one).
Turns out it’s not just a weird hormone joke — it’s a real thing. Hospitals often sell placentas to biotech and cosmetics companies. They’re rich in stem cells, collagen, and growth factors, so there’s real demand.
What’s messed up is that this often happens without the mother’s full understanding — just a vague “medical waste” form slipped in during a chaotic, vulnerable moment. No clear disclosure. No compensation. Just standard operating procedure.
So yeah — this isn’t just quirky biology trivia. It’s capitalism extracting value from mothers and newborns, at one of life’s most sacred and exposed moments.
Joke withdrawn. Eyes open. E3Male:HumanNof1 still learning, E3Male:HumanNof1 apologizies
3 Likes
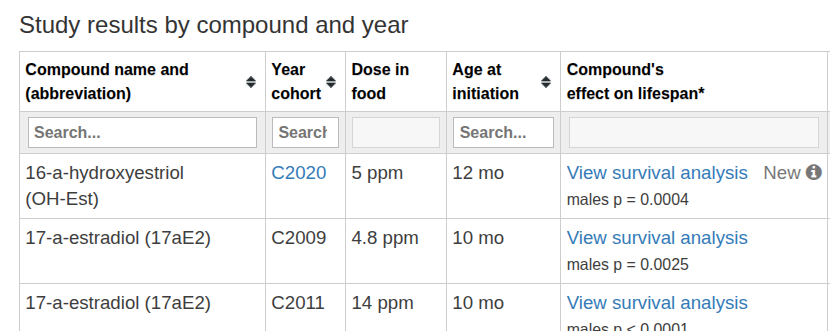
Estriol update + ITP paper correction
A quick note on the (yes, seminal—first-of-its-kind) ITP paper: GeroScience issued a correction—what the paper first called “16-hydroxyestriol” in multiple spots is correctly “16-hydroxyestradiol” (i.e., estriol, E3). The journal lists five fixes (title, abstract, intro, discussion, Table 1). SpringerLinkScholars @ UT Health San Antonio And I can’t be too harsh on them as in this thread I found several places where I used the term E2 instead of E3, which I have corrected. So it happens to the best of us:)
I’d paused most supplements to get my lipids in line (ugly CAC score), but I’m restarting with a test run of topical E3. About three days in, I noticed the usual appetite effect—little interest in dessert/candy/cookies after dinner. N=1, subjective, but that’s my repeat experience.
Sharing personal experience, not medical advice. Also, I’d skip E3 in younger men—possible testosterone/fertility impacts—so if you’re still building a family, this is a hard no-go. imho
3 Likes
This is a link to the original ITP paper with the mis-information/labeling/naming. which annoyed me no end.
Lifespan effects in male UM‑HET3 mice treated with sodium thiosulfate, 16‑hydroxyestriol, and late‑start canagliflozin
Obviously I’ve embraced E3 and I’ve bumped up dapagliflozin to be on the essential medicines list for me. I took a hard pass on thiosulfate, the required dosing level didn’t seem feasible…
3 Likes
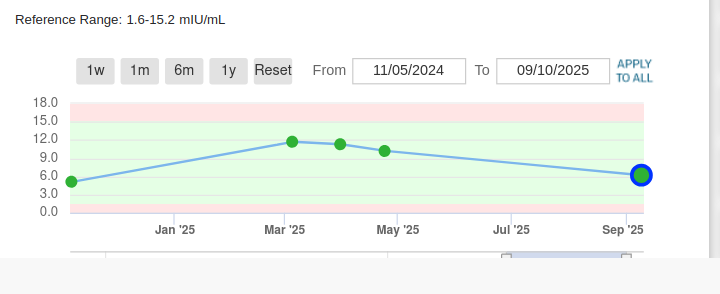
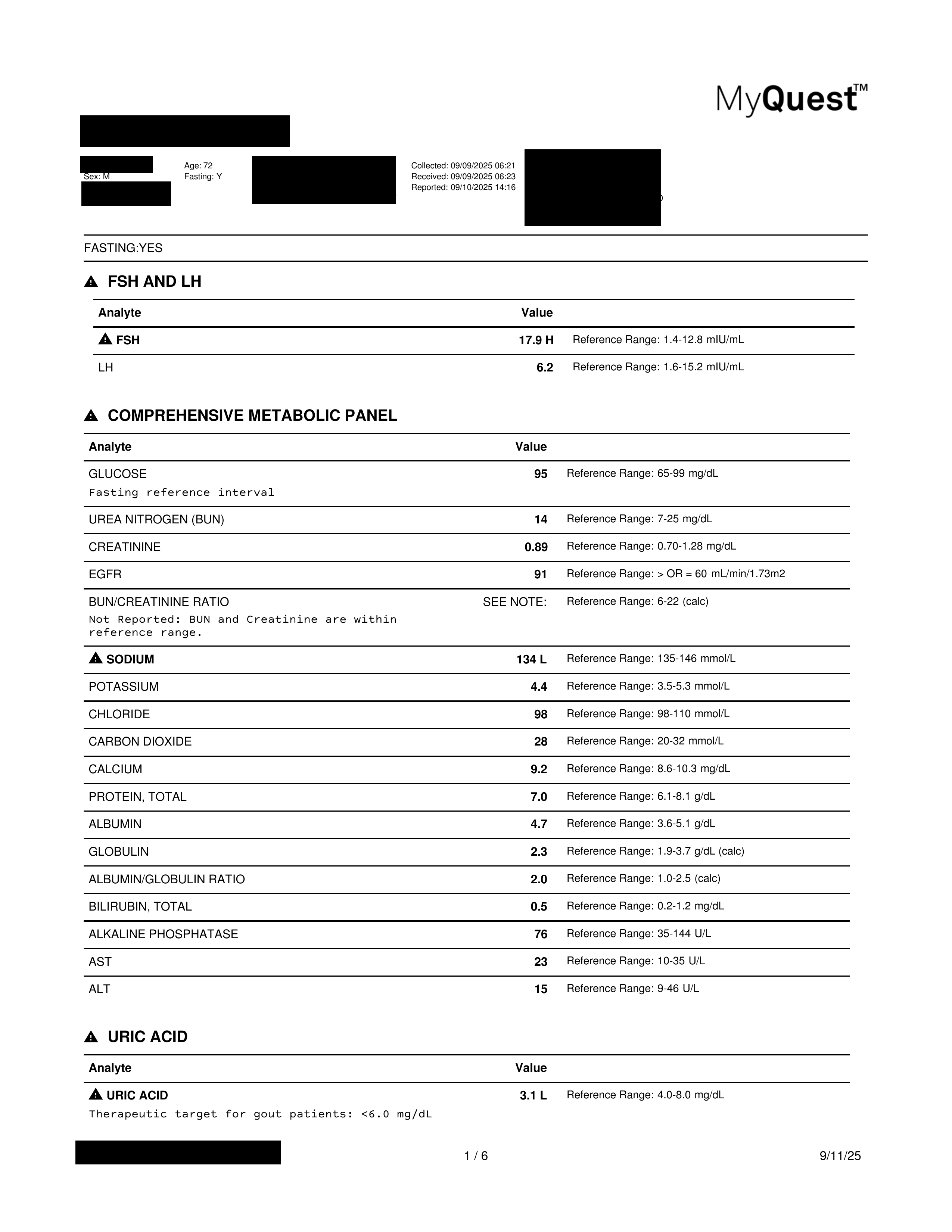
Coming up on the one-year mark as E3-N1-Male, so time for a recap. I’ve attached my latest labs and screenshots of the markers I watch most closely, and at the end I have my full lab results.
My E3 use has been a bit uneven. After the high CAC scare I hit pause for about 10 weeks to get my lipids in order. Since then I’ve restarted: 3 mg Fri/Sat/Sun every other weekend, alternating with rapamycin weekends. I’ve also picked up some E3 cream that I use here and there when the mood strikes. All told, between the pill cycles and the cream a few times a week, I figure I’m getting roughly 30 mg of estriol systemically each month.
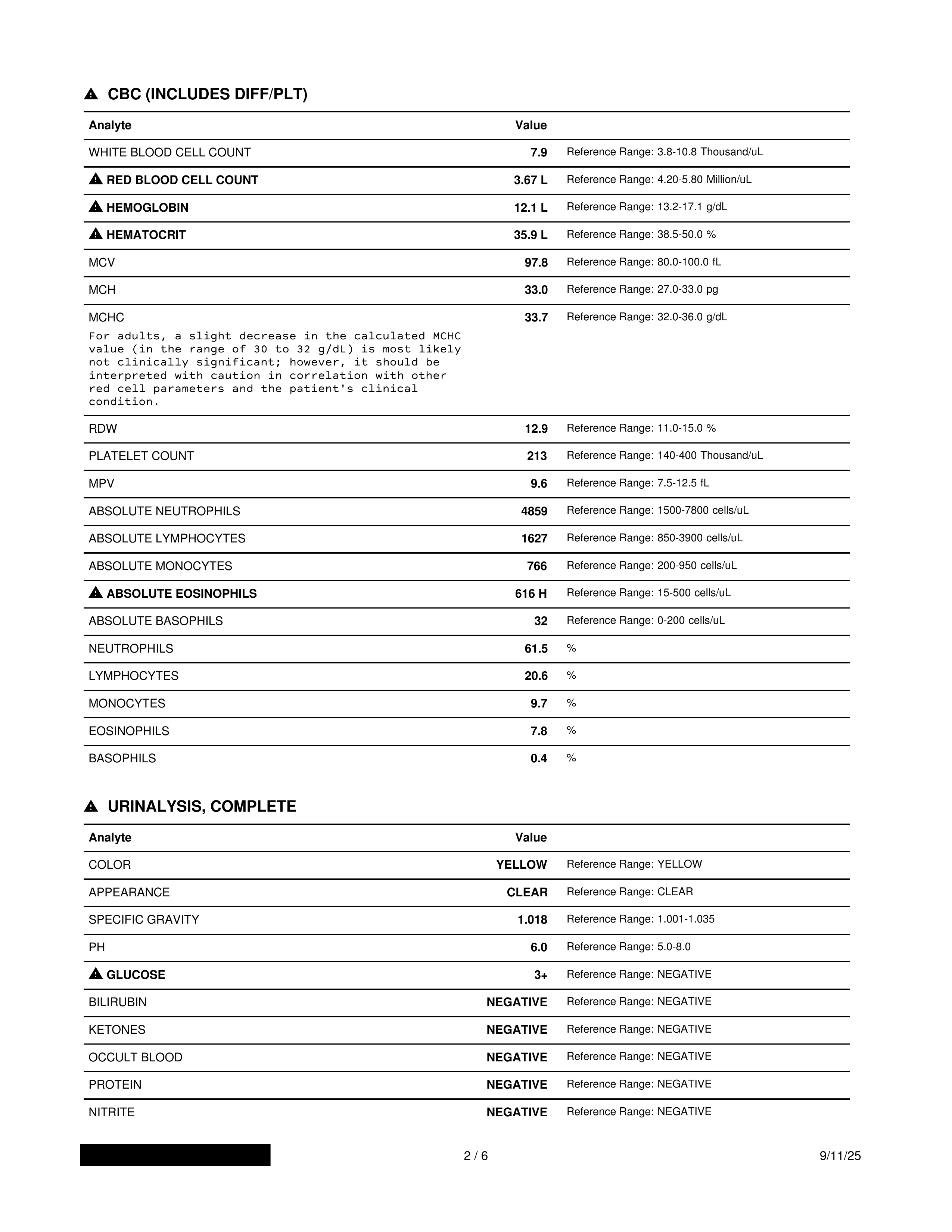
In the full panel there are a couple of odd readings, though unrelated to E3. I’ve had what looks like mild anemia for years — those low blood markers showed up well before I ever started E3. My PCP hasn’t been concerned, and I’ve had no symptoms. I even tried iron and B-vitamin supplements, but the numbers never really changed, so I’ve come to accept them as my “normal.” The labs also show elevated urine glucose, which is expected since I take dapagliflozin.
The main red flag is that my Levine score has taken a noticeable turn for the worse. Earlier I was showing more than a decade younger; now it reads a pheno age of 65 against my chrono age of 72. I don’t know why, but it’s clearly a “worsening” of a recognized metric, and that can’t be good. That said, I don’t see any obvious way the Levine markers would tie directly to E3’s known effects.
So I plan on continuing my current regime. If the Levine pheno age keeps worsening, I’ll change course. Until then its straight sailing for me.
1 Like
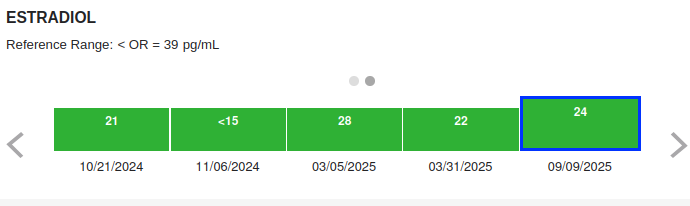
Estradiol has trended up as might be expected.
1 Like
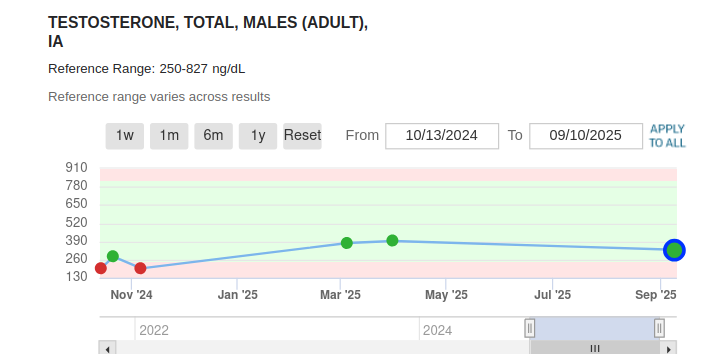
My basic T is up from the baseline pre-dosing 200ng level. I have no “symptoms” to complain about. My libido is fine. I do PDE5’s, tadalafil every other day and sildenafil occasionally, and those greatly help expand blood flow. So yes, the T numbers don’t look too beefy, but I’m feeling fit and firm, so these relatively low numbers don’t bring me down.
2 Likes
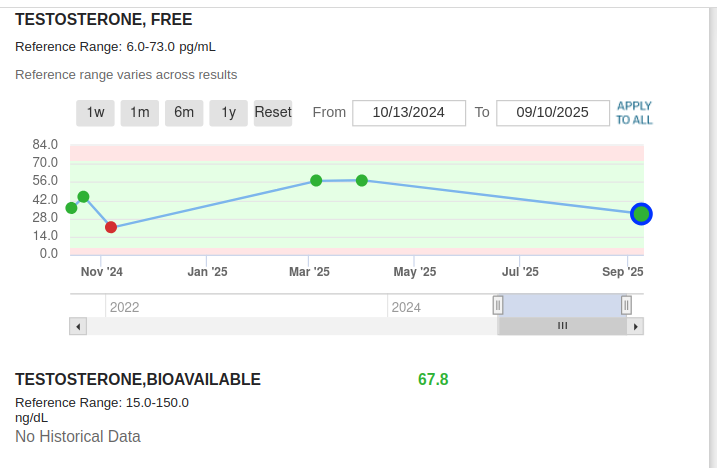
And these free testosterone levels don’t bother me either. Some might scoff at the 67 bioavavalilbe testosterone, but I actually feel pretty good about it. It’s 4x above the lower RR limit.
1 Like
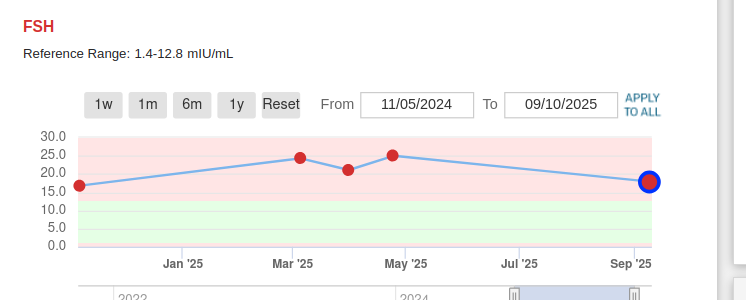
FSH and LH weren’t taken at baseline. I took my first blood test of these AFTER starting E3. And the FSH has been over RR the whole time. While the LH has been well within. I don’t know why. I think someone mentioned that it is an “adaptation” to keep sperm production up.
2 Likes
Very interesting results. Thanks for posting!
1 Like
Tom_Clark, the blood work looks pretty good to me and definitely better than mine. By the way, are you hypothyroid?
Correction: There never was an E3 trial starting from weaning. The only trial started at 12 months. Makes sense, E3 for a young person/animal still developing would be awful/bad not a good idea at all.
Newest ITP Link
1 Like
Would be curious to hear updates on this as it goes on.
1 Like