October 27th 2024
Increasing to 6mg bolus dose
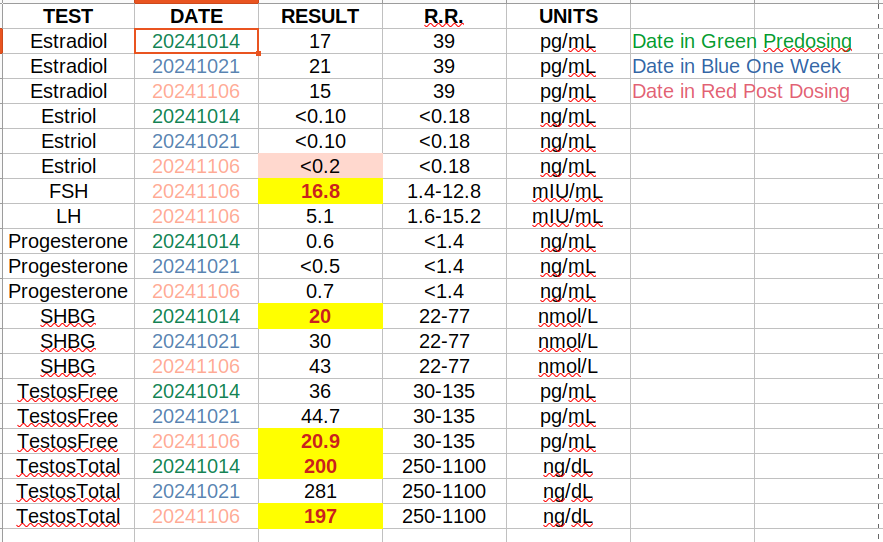
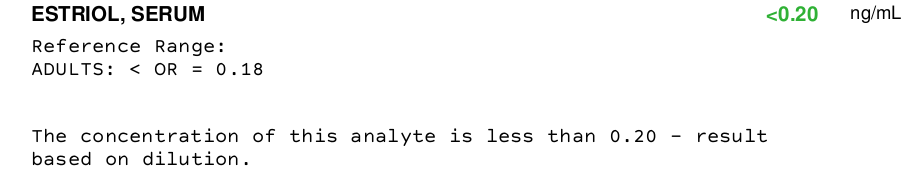
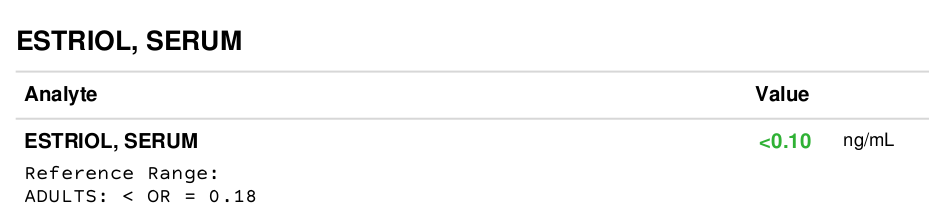
Sensitivity of the common Estriol Test
0.2ng/mL or 200pg/mL, i.e. it only reads values above 200pg/mL
From “https://en.wikipedia.org/wiki/Estriol_(medication)”
“Estriol levels at term are normally between 5,000 and 20,000/pg/mL”
From: “Pharmacokinetics and pharmacodynamics of three dosages of oestriol after continuous vaginal ring administration for 21 days in healthy, postmenopausal women - PMC”
"The oestriol plasma concentrations is about 7.9 pg/ml in days 5–7 and 11.1 pg/m ln days 20–22 of the regular female cycle.”
Comment: Makes clear the test I’m using is only designed for pregnant women. And for wiki, it looks like a decent entry.
From: "Efficacy and safety of oral estriol for managing postmenopausal symptoms. By Kentaro Takahashi”
“investigators have been able to initiate very little carcinogenesis in animal studies unless large doses (200 –500 mcg/kg per day) were used on a continuous basis”
Comment: For me 200mcgx70kg==14000mcg==14mg, so not that much headroom
From: “Estriol: Safety and Efficacy by Kathleen A. Head, N.D.”
It may be that estriol’s effect on the endometrium has less to do with the dose and more to do with the frequency of administration, with more frequent dosages being more likely to contribute to endometrial hyperplasia.
Comment: This suggests a bolus dose, which I’ve also seen suggested other papers.
From wiki: Estriol (medication) - Wikipedia**
Comment: This indicates 2hr post dose while fasting will be the max. But it still won’t register on the crude common test that just says less than 0.2ng/mL
All of which begs the question “What’s u gonna do sailor-boy?”
6mg bolus dose now through next test.
But I won’t get my results until the day before the following and final test.
So if the 6mg doesn’t get above the test minimum, I’ll do 9mg bolus on the last day of the test to try to get some reading from which I can extrapolate downward.


#/media/File:Levels_of_estriol_with_administration_of_8_mg_oral_estriol_or_0.5_mg_vaginal_estriol_in_women.png){kind=link}