I didn’t know, so why do you take rosuvastatin then?
I see no reason to switch right now to atorvastatin unless there is a large RCT that has showed benefit in all cause mortality like rosuvastatin.
1 Like
Better question: If you were being prescribed statins for the first time and were given your choice of the two, which would you pick?
1 Like
I wrote more on rosuvastatin over atorvastatin here:
Add in detected benefit for ACM for rosuvastatin. That’s much better. This is an association study. 10 mg atorvastatin had null effect in it.
I am thinking actually about skipping ezetimibe and going to high dose statins, because 20 mgs showed benefit in ACM in JUPITER.
1 Like
Another thing I wonder.
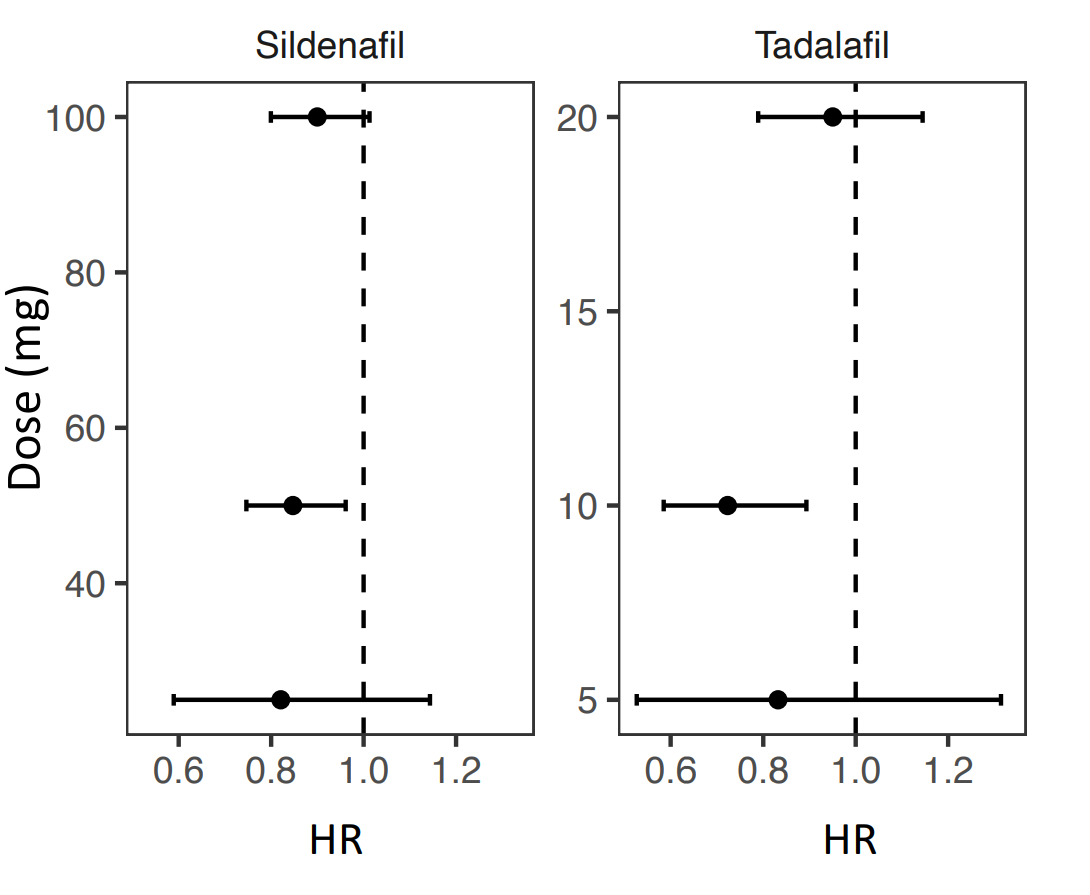
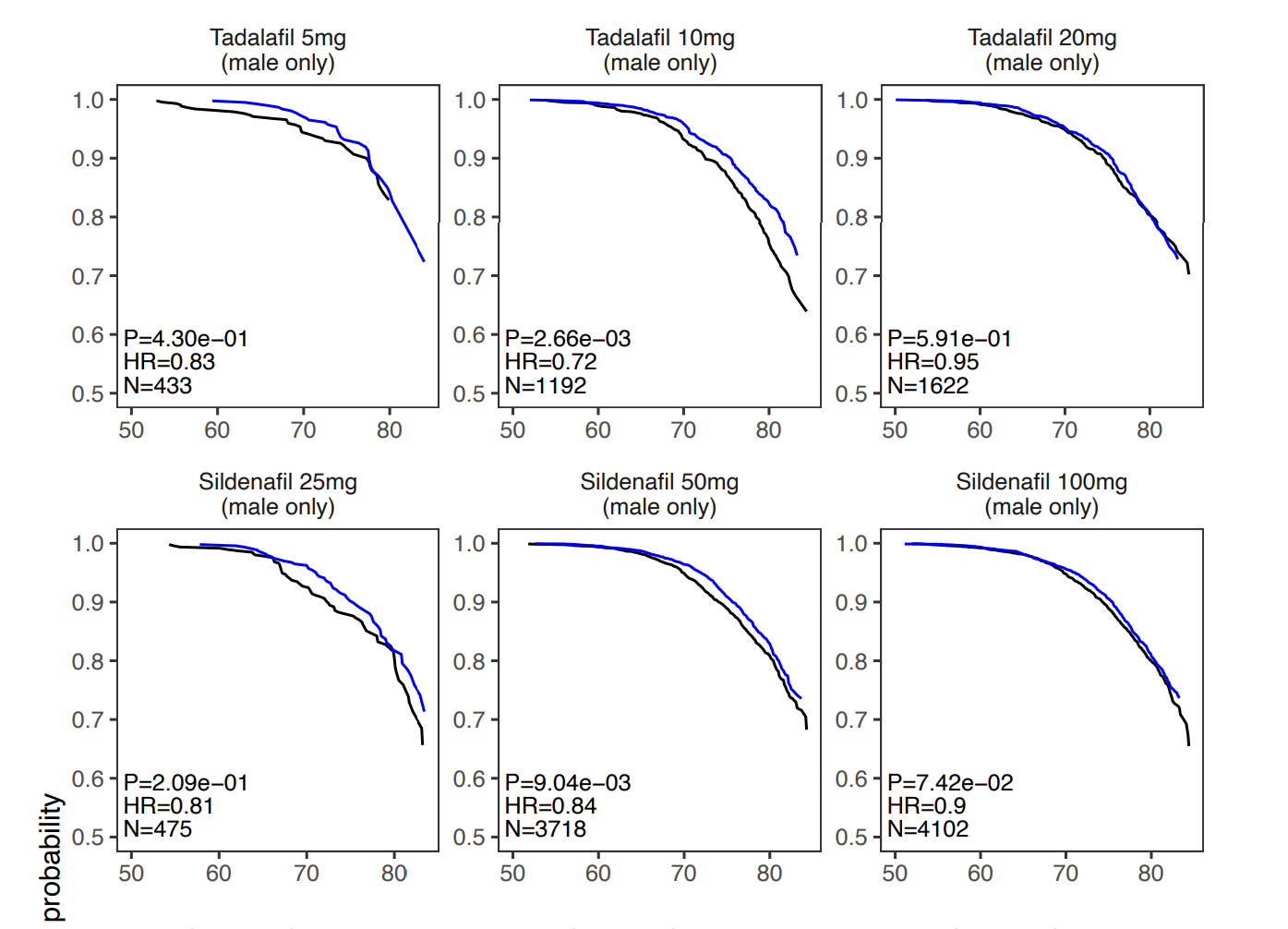
I don’t see Tadalafil mentioned anywhere so I wonder if the mortality benefits were only seen with Sildenafil.
It’s in the supplementary material: https://www.medrxiv.org/content/10.1101/2024.03.08.24303967v1.supplementary-material
The problem is that they didn’t do the disambiguation between generic names and brand names correctly, so for instance the dataset lists:
- FENBID and IBUPROFEN
- Tadalafil (HR 0.86 CI 0.75–0.99) and Cialis (HR 0.77 CI 0.60–0.99)
- IMIGRAN and Sumatriptan.
If done correctly, this might change the results.
Something else that I don’t understand: Telmisartan HR in males = 0.76 but HR for telmisartan 40 mg = 0.80 and HR for telmisartan 80 mg = 0.82. How can the HR for telmisartan be lower than the one for each telmisartan dose?! I would expect HR (A+B) < min(HR(A), HR(B)).
Also, in drugs, there is “FREESTYLE TESTING STRIPS”…
Not reassuring on the quality of the paper…
5 Likes
Yea this is extremely interesting but there still seems to be so many flaws here. I also can’t for the life of me understand how viagra could have more health benefits than cialis when it’s so much shorter acting.
3 Likes
I contacted the author (turns out we went to the same high school…): they’ll try to fix the various mistakes in the upcoming revision before final publication.
6 Likes
Atorvastatin is the most commonly prescribed statin.
The statin data is really interesting. I think a lot of folks here have a preference for less lipophilic statins, on the theory that these will cross BBB the least and affect muscle the least. However, those statins also have the longest half lives, which could result in the statin building up in your system. I had a theory that it might actually be the more lipophilic, lower half life statins that are safer. Atorvastatin sits in the middle, moderately lipophilic, moderate half life. Maybe it’s a kind of sweet spot, though the half life doesn’t seem so much shorter than rosuvastatin.
I can’t find a good primary source right now, here are lipophilicity rankings from GPT-4:
- Lovastatin - Highly lipophilic; easily crosses cell membranes and is metabolized by the liver.
- Simvastatin - Similar to lovastatin in lipophilicity and is also a prodrug, activated in the liver.
- Atorvastatin - Less lipophilic compared to lovastatin and simvastatin but still relatively lipophilic.
- Fluvastatin - Intermediate; less lipophilic than the first three.
- Pitavastatin - Has both lipophilic and hydrophilic properties.
- Rosuvastatin - More hydrophilic than the previous statins, which may contribute to its lower rate of certain side effects.
- Pravastatin - The most hydrophilic statin, which means it’s less likely to penetrate cell membranes and may have fewer side effects related to muscle tissue.
And half lives, also from GPT-4:
- Simvastatin - Approximately 2 to 3 hours.
- Lovastatin - Around 3 hours.
- Fluvastatin - Approximately 3 hours.
- Atorvastatin - About 14 hours.
- Pitavastatin - Roughly 11 to 12 hours.
- Pravastatin - Around 19 hours.
- Rosuvastatin - Approximately 19 to 20 hours.
2 Likes
This provides another reason to add a flozin like empagliflozin to my stack. Thanks for this!
1 Like
Not in the UK:
The 3 most prescribed drugs in the dataset were amoxicillin (N=73371), simvastatin (N=45776), and omeprazole (N=44100).
There are weird findings in the paper, for instance, for sartans:

The results are only statistically significant for candesartan (and in a bad way…), but what could explain the positive trend for telmisartan and the neutral one for losartan?
Many people consider (and I think they’re wrong) that candesartan is as good as telmisartan. Candesartan failed the ITP and the ITP is now testing telmisartan.
Same for what they found regarding statins (atorvastatin better than simvastatin): simvastatin failed the ITP and atorvastatin is now tested (combined with telmisartan).
So either this paper is crap (it’s possible, most papers are crap, and there are many mistakes in this one), or they really found something interesting…
4 Likes
I jumped on the Empagliflozin train a couple years ago.
Also, this doesn’t get enough attention but it’s the only drug class to show potential benefits for diastolic heart failure. No other drug has succeeded in doing so.
Empagliflozin for Heart Failure With Preserved Left Ventricular Ejection Fraction With and Without Diabetes
Conclusions:
In patients with heart failure and a preserved ejection fraction enrolled in the EMPEROR-Preserved (Empagliflozin Outcome Trial in Patients With Chronic Heart Failure With Preserved Ejection Fraction), empagliflozin significantly reduced the risk of heart failure outcomes irrespective of diabetes status at baseline.
https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.122.059785
3 Likes
Yeah pretty much in two clinical trials for primary prevention (one in hypertension, one in diabetes):
3 Likes
Lifespan IO write up on this paper
2 Likes
I am still thinking about that Naproxen result. I am wondering if the people took it daily or only as needed. I’ve always tried to only use it if sick but I have to say, the feeling of having minor joint pains go away on it is very appealing if it’s also going to extend lifespan.
Interesting paper.
It has been discussed in other threads whether or not tadalafil would be as effective as sildenafil because it would perhaps be more convenient to take tadalafil because of its longer half-life.
The possible confounders regarding dosing are not discussed.
2 Likes
I’m curious about the confounders here as well. Tadalafil is typically prescribed at a once daily dose of 5mg (for BPH and maintenance treatment for ED), whereas 10mg and 20mg are typically only prescribed to be taken prior to sexual activity. This could indicate that 10mg/daily is not the same as the dose used by participants in the database (possibly 10mg/sexual activity). Personally, I’m giving 10mg/day a try to see if I notice anything subjectively different (eg more muscle pump in gym). I can’t say I’ve really noticed anything from 5mg though.
2 Likes

The 14 drugs that increased lifespan:
Cardiovascular / metabolic
- Atorvastatin (statin)
PDE5 inhibitor
- Sildenafil (Viagra)
Anti-inflammatory
- Naproxen
Estrogen / hormone-related (multiple hits)
- Estradiol
- Estriol
- Estraderm
- Vagifem
- Marvelon (ethinylestradiol + desogestrel contraceptive)
Other pharmaceuticals
- Lymecycline (antibiotic)
- Otomize (ear drop: steroid + antibiotic combo)
Vaccines
- Avaxim (hepatitis A vaccine)
- Revaxis (diphtheria, tetanus, polio booster)
ChatGPT summary:
Study Overview
- Researchers analyzed ~500,000 participants from the UK Biobank with up to ~20 years of follow-up.
- Looked at 400+ medications and compared users vs matched controls.
- Adjusted for confounders: age, sex, disease status, BMI, smoking, socioeconomic status.
- Goal: identify drugs associated with lower all-cause mortality (proxy for lifespan extension).
Core Finding
- The majority of drugs were linked to higher mortality.
- This is expected due to confounding by indication (people taking meds are often already sicker).
- After filtering for strong statistical signals → only 14 drugs showed lifespan-associated benefits.
Top Longevity-Associated Drug Classes
-
Statins (e.g., atorvastatin)
→ Likely via cardiovascular risk reduction over decades -
PDE5 inhibitors (e.g., sildenafil/tadalafil)
→ Possible mechanisms:- Improved vascular function
- Lower blood pressure
- Potential neuroprotective effects
- Or indirect: higher sexual activity / overall health marker
-
Hormone Replacement Therapy (HRT) (estrogen/estradiol)
→ Strong signal in women
→ Supported by known sex differences in lifespan -
SGLT2 inhibitors (newer diabetes drugs)
→ Among the strongest signals observed
→ Effects likely go beyond glucose control (multi-organ benefits)
Metformin Reality Check
- Despite its reputation, Metformin did NOT show a lifespan benefit in this dataset.
- Earlier studies suggesting benefit (even vs non-diabetics) have not consistently replicated.
- Mechanism still unclear and possibly too “broad/dirty” compared to newer drugs.
Important Nuance
- Not all “beneficial” drugs are overcoming disease risk.
- Some (like HRT or PDE5 inhibitors) are not strictly disease-driven, which reduces confounding.
- Socioeconomic factors were controlled for, but never perfectly.
Mechanistic Themes Emerging
Across both human data + animal work:
- Insulin sensitivity / glucose handling (SGLT2, diabetes pathways)
- Growth signaling (PI3K, mTOR, IGF-1)
- Cardiovascular function
- Hormonal environment
- Systemic damage response
Animal + Translational Work
-
Follow-up studies are testing these drugs in:
- Worms (C. elegans)
- Flies
- Fish
- Mice
- Goal: find conserved lifespan effects across species → higher chance of human relevance.
Biomarkers Angle
- Shift from just lifespan → biological age + mortality prediction
- Proteomics emerging as key tool
- One standout marker: GDF15
- Strongly correlated with age and mortality
- Possibly reflects damage or senescence burden
- Role (causal vs protective) still unclear
Limitations
- Observational study → cannot prove causation
- Confounding still present (even after adjustments)
- Only includes prescription drugs (no supplements, diet, etc.)
- Newer drugs (like SGLT2 inhibitors) have shorter follow-up
Big Picture Takeaways
- True human longevity signals are rare when rigorously analyzed
-
Some drug classes consistently stand out:
- SGLT2 inhibitors
- PDE5 inhibitors
- Estrogen therapies
- Statins (context-dependent)
- Metformin is not as strong as often claimed
-
Future direction:
- Cross-species validation
- Mechanism-first targeting (PI3K > mTOR may be underappreciated)
- Better biomarkers tied directly to mortality
Bottom Line
We’re moving from hype to signal. Out of 400+ drugs, only a handful show real-world associations with longer life. The next step is figuring out which of these actually cause the effect and why.
8 Likes