Ostarine, also known as Enobosarm, GTx-024, and MK-2866, is a selective androgen receptor modulator (SARM) that has gained significant attention in both clinical research and the bodybuilding community. SARMs like Ostarine are designed to stimulate androgen receptors selectively, offering a higher anabolic activity (muscle and bone growth) relative to androgenic activity (development of male characteristics). This selectivity makes Ostarine a potential candidate for treating muscle and bone wasting diseases while minimizing the side effects associated with traditional anabolic steroids.
Mechanism of Action
Ostarine works by selectively binding to androgen receptors, primarily in muscle and bone tissues. This selective binding allows for significant anabolic effects with reduced androgenic side effects compared to testosterone and other steroids. The ideal anabolic agent should be selective for muscle and bone, orally bioavailable, and avoid converting to DHT or estrogen, which are associated with side effects like prostate issues and gynecomastia. Ostarine aims to meet these criteria, making it a promising alternative to traditional anabolic steroids.
Clinical Trials and Findings
Ostarine has been extensively studied in clinical trials, with over 1500 subjects treated in 27 completed or ongoing trials. Dosages in these trials have ranged from 0.1 mg to 100 mg per day. Notably, Ostarine was the first drug to be placed on the FDA’s fast-track development program for the prevention and treatment of muscle wasting in cancer patients.
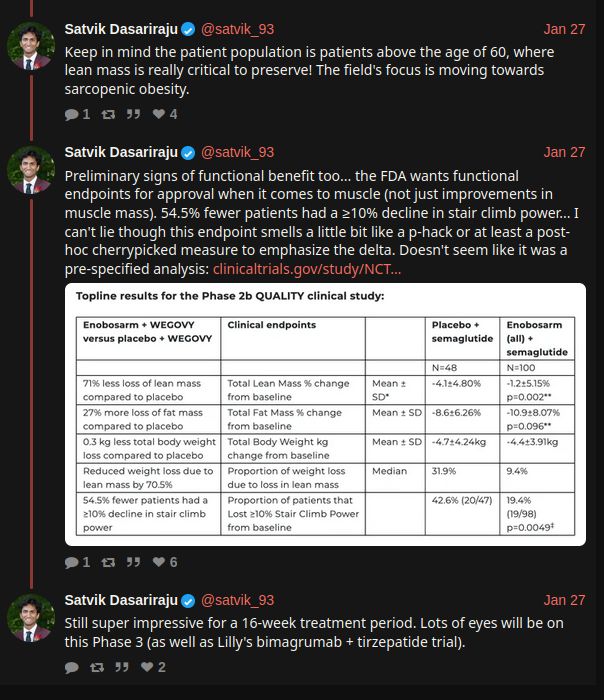
In a significant Phase III trial, 325 lung cancer patients were given either 3 mg of Ostarine per day or a placebo. While the trial did not meet its primary endpoints for preventing muscle loss in the overall population, it did show that Ostarine significantly increased or maintained lean body mass (LBM) compared to the placebo. This finding highlighted Ostarine’s potential anabolic effects, even at low doses.
Another Phase II trial focused on Ostarine as a treatment for stress urinary incontinence in women, but the results did not achieve statistical significance. However, a different Phase II trial evaluated Ostarine as a form of hormonal therapy for women with estrogen receptor-positive (ER+) and androgen receptor-positive (AR+) breast cancer. This trial, using dosages of 9 mg and 18 mg daily, met its primary efficacy endpoint, demonstrating clinical benefit response (CBR).
Dosage and Usage
In clinical trials, dosages ranged from 0.1 mg to 100 mg per day. In the bodybuilding community, dosages typically range from 10 to 25 mg per day. Anecdotal reports suggest gains of 5-10 pounds of lean mass are common with these dosages.
Side Effects
Decreased HDL Cholesterol:
Ostarine has been shown to reduce HDL cholesterol levels, a common side effect with anabolic steroids and other SARMs.
Testosterone Suppression:
Ostarine suppresses LH and FSH, leading to decreased testosterone levels in a dose-dependent manner. It also lowers SHBG levels. While suppression is less than that of traditional steroids, it is still significant.
Estrogen Imbalance:
Ostarine does not aromatize into estrogen but can create an imbalance by suppressing natural testosterone and occupying androgen receptors, potentially leading to elevated or decreased estrogen levels. Symptoms of high estrogen include acne, erectile dysfunction, low libido, lethargy, and gynecomastia. Symptoms of low estrogen include dull orgasms, dry skin, dehydration, and mood swings.
Androgenic Activity:
Ostarine exhibits a dose-dependent increase in androgen activity, although to a lesser extent than traditional steroids. This can still lead to androgen-related side effects, albeit reduced.
Hair Loss:
While Ostarine generally does not cause significant androgenic alopecia at common dosages, hormonal fluctuations can lead to temporary shedding.
Liver Toxicity:
Clinical trials showed short-lived increases in ALT levels in some subjects, but these resolved while continuing the dosage. At higher recreational dosages, some liver enzyme elevation is possible but likely resolves after discontinuation.
Lack of Aromatization and 5-Alpha Reduction:
Ostarine does not aromatize or undergo 5-alpha reduction, which contributes to its muscle-selective profile and lack of water retention, reducing cardiovascular stress compared to steroids like Anadrol.
Half-Life and PCT
Ostarine has a half-life of 23.8 hours, allowing for once-daily dosing. Post-cycle therapy (PCT) is recommended after an Ostarine cycle to restore natural testosterone levels. PCT should start the day after the last Ostarine dose due to its half-life.
Conclusion
Ostarine is a promising SARM with significant potential for treating muscle and bone wasting diseases due to its selective anabolic activity and reduced androgenic side effects. While it has shown positive results in increasing lean body mass in clinical trials, more research is needed to determine its long-term safety and efficacy. In the bodybuilding community, Ostarine is valued for its ability to enhance muscle growth and strength with fewer side effects than traditional steroids. However, users should be aware of potential side effects such as HDL cholesterol reduction, testosterone suppression, and estrogen imbalance. Proper PCT is crucial to mitigate these effects and maintain health.