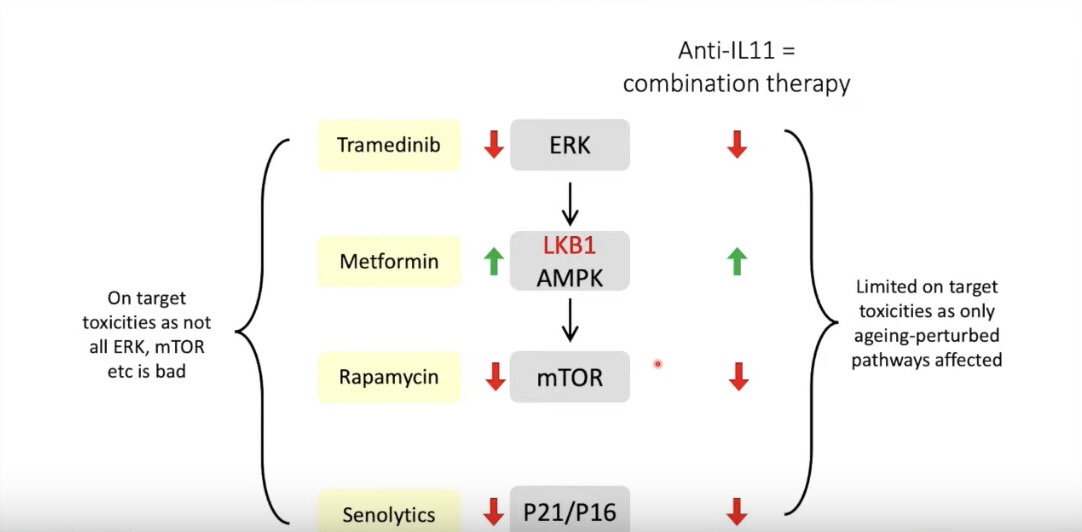
The diagram above suggests it’s possible at some level to emulate the mechanism of IL-11 inhibition utilising a number of readily available compounds all be it that trametinib is on a different level of cost to the remaining three compounds ( including Senolytics).
I would be very interested to know if anybody has the knowledge and experience to translate this diagram into a dosing schedule in both quantum and timing?
For the record I take 10mg of Rapamycin as a single weekly dose, 500mg Metformin daily, and dose with 100mg Dasatinib plus 2000mg Fisetin as a Senolytic on the two days prior to taking Rapamycin.
How would one consider modifying this approach to include Trametinib?
It would appear on the face of it that this would deliver against the reported benefits of IL-11 inhibitors
Do we now take lithium, trametinib, and rapamycin together?
As
FWIW in the US a prescription of 2mg of Trametinib {Mekinist] 30 tablet is around $13,050.00 with a discount coupon {17% off the average retail price of $15,826.00
The India version is only ₹72,000 around $870.00 USD
Maybe this is a little off topic but am I reading this correctly? You are taking the senolytic cocktail D&F for two days every week? Is there a special situation where such a high frequency is warranted?
When I started out a few years back I had an in person consultation with Dr Green ( caught COVID on the plane on the way home - early adopter ) with the intention of becoming a patient.
At that time a Senolytics cycle was advocated every three months and since then the cycle has moved around but invariably shorter.
It’s difficult to work with doctors in the USA from the UK mainly relating to drug supply so now I work alone but equally attempt to follow Dr Green in my approach ( that is not to say he is advocating a weekly approach - it is my approach based on my best understanding of his current strategy - working alone!) and I believe he currently advocates regular and frequent Senolytics use.
I cannot say if this is optimal Senolytics strategy but I find it well tolerated and not arduous within my regime.
If you really want to target senescent cells, I think taurine works better. Mouse studies showed taurine supplemented mice had far fewer senescent cells than D+Q treated mice.
Add in Rapamycin and your senescent cells load should be minimal.
I tend to not put much value on Drosophila or C. Elegans results. It suggests that we should test in mice, but I wouldn’t start taking something solely because it extends lifespan in those models.
Trametinib (at 80kg human equivalent dose of 9.4mg) was also shown to increase median lifespan in mice: 7.2% increase in females and 10.2% in males. Also excitingly, combination of trametinib and rapamycin gave additive lifespan extension. Rapa extended median lifespan by 17.4% and 16.6% in females and males, respectively. Whereas trametinib+rapa extended it by 27.4% in males (the female group hadn’t yet reached 50% survival yet upon publishing).
The downside of this results is that the control mice didn’t live very long. Even the median lifetime of rapa+trametinib male mice was only 912 days, which is actually shorter than the reported median lifespan for that strain. On the bright side they did have a large sample size.
Inbred rodent strains vary a great deal in their longevities, aging patterns, and responses to caloric restriction. The median life span for ad lib-fed B6C3F1 hybrids (males and females combined) in the BAP study was 933 days, or about 11% longer than for ad lib-fed C57BL6, one of the parental strains. [ref]
Just trying to guess from the graph it looked like the female rapa+trametinib group median lifespan might end up being around 1,100 days, which would be more impressive. Perhaps the full results will be published in a journal at some point. Definitely seems a combo that should be urgently tested in ITP.
They identified two variants (one in a RAS GAP, the other in c-RAF) which inhibit ERK signaling. Also interesting: one of these variants inhibited mTORC1 when expressed in mouse ESCs, while the other actually activated it.
Trametinib is prescribed for certain cancers (as monotherapy, or in combination with b-RAF inhibitor for cancer with b-RAF mutations). See below clinical trials for dose and associated adverse effects.
We enrolled 206 patients (median age 58·5 years, range 19–92). Dose-limiting toxic effects included rash (n=2), diarrhoea (n=1), and central serous retinopathy (n=2). The most common treatment-related adverse events were rash or dermatitis acneiform (n=165; 80%) and diarrhoea (87; 42%), most of which were grade 1 and 2. The maximum tolerated dose was 3 mg once daily and the recommended phase 2 dose was 2 mg a day. The effective half-life of trametinib was about 4 days. At the recommended phase 2 dose, the exposure profile of the drug showed low interpatient variability and a small peak:trough ratio of 1·81. Furthermore, mean concentrations in plasma were greater than the preclinical target concentration throughout the dosing interval. Pathway inhibition and clinical activity were seen, with 21 (10%) objective responses recorded. [ref]
Thank you Destrider - Very interesting and helpful - just the sort of insight one is looking for through an interactive site like this.
To be fair Dr Green advocates Taurine (3mg per day if there is any further comment on dosing) and Taurine is in my daily schedule, what his comments did not relay was the link to Senolytic activity. However that may be a function of being on the outside of his treatment program!
Time for a review! Any reduction in dosing complexity is certainly welcome.
The dosing I have heard that best mimics the trials is your age/10 of grams of taurine daily rounded up. So for someone who is 51-59 you would take 6 grams of Taurine daily.
Since taurine increases MTOR, I start taking it 3 days after my Rapamycin dose.
When it comes to managing hungovers, it is DHM, dihydromyricetin that sometimes is used. @John_Hemming should be the expert in this field. I have only used DHM a few times.
I was a Dr. Green client for 4 years while he was alive. He was a good man and a trailblazer. I’m thankful for the experience of working with him. Your senolytics protocol is concerning given my experience working with him for years. He started me on Rapamycin and required 6 months on Rapa alone before allowing the introduction of Senolytics into the protocol. Once I was stable and seeing positive results (reduced gum inflammation during dental exam) on Rapa with no serious side effects, then we introduced Senolytics into the protocol. I had fairly severe osteoarthritis and several big athletic endurance events coming on the calendar, so we agreed to an intensive introduction to try and knock the senescent cell burden down. I did 3 rounds of D 100mg + Q 1200 mg on two consecutive days every two weeks, then moved it out to three rounds every three weeks, then 3 rounds monthly, then three rounds every two months, and I’ve been on quarterly maintenance intervals ever since (all were two consecutive days of D 100mg + Q 1200 mg). To the best of my knowledge, there is no research to support weekly dosing. It is far too extreme. He considered my protocol adoption quite extreme, but there was research to support this approach and I had specific needs we were trying to meet. In the final year before he passed, he added 6 grams of Taurine (I’m 64, so consistent with the above - age divided by 10) and GlyNAC. My point writing this is I was shocked that you had adopted a weekly protocol of D+Q senolytics. The research shows an 11 day tail effect after each dose, which would imply every two weeks would be the absolute minimum time interval and probably only at the beginning for loading. I would encourage you to read the supporting research and reassess what you are doing. Remember, Dasatnib is a cancer drug, so it’s not taken lightly. FWIW, the combination of these therapies completely cleared up my osteoarthritis symptoms. N=1. Hope that helps.