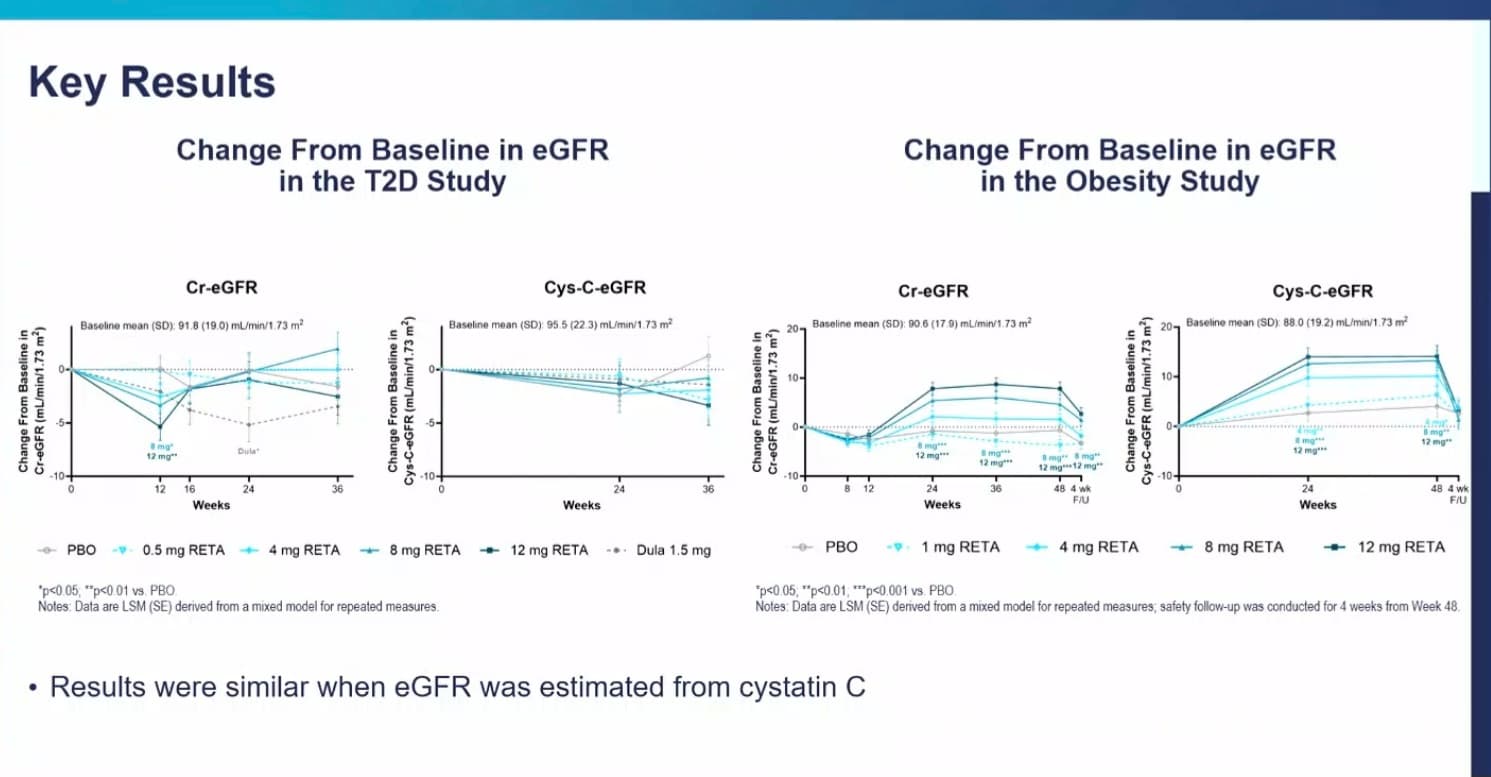
In short, egfr **increased ** while patients on treatment with retatrutide after 24 weeks or so. To my knowledge, there is currently is no drug that actually increases egfr, the current best in class ones only slow down the decrease.
Keep in mind that increasing GFR is not always a good thing. Depends on the mechanism. Hyperfiltration increases GFR but leads to long term nephron damage. Just an example.
Indeed, simply raising blood pressure will increase GFR, but lead to long term nephron damage. CKD naturally causes the kidney to emit Angiotensin II etc that raises blood pressure, to compensate for falling GFR. ARB and ACE class blood pressure medications were developed to block and reverse this natural effect, thus lowering GFR in the short term, to prevent long term damage from high blood pressure.
The important question is if Retatrutide improves GFR by a mechanism that does NOT lead to long term nephron damage.
As I understand it, high egfr with normal or falling uacr is good and doesn’t lead to nephron damage long term. The slides in the presentation above show that, although I didn’t link to them.
A low and slow approach may be enough to arrest a decline without leading to further damage. But low may do nothing. What are the advantages to deriving GFR from cystatin-c? Cost at Labcorp is $35 for a Cr-renal panel, $119 for cys-c.
The way I understand it is that the calculated one relies on creatinine levels which can be high after exercise, in athletes, and in people having a high protein diet.
The test relying on Cystatin c is a more direct measure of filtration function without the confounders that affect the one based on creatine.
Am I missing something? In T2D group, only one dose of reta results in improved Cr-eGFR, and the highest dose performs worse than placebo. For cys-eGFR, all doses are worse than placebo! And in the obesity study, improvements drop toward or below baseline 4 weeks after reta is stopped. So if you’re obese and stay on reta for the rest of your life, it may be helpful. Does that mean the effect is mediated by fat loss? I wonder what would happen if you’re not obese but want to lose a few pounds and are taking reta for its metabolic benefits, what would the impact be?
All of those changes were non-significant, so likely explained by natural variability. Still will be good to see some phase 3 data, though, which we will very soon.
Those few pounds are likely coming from visceral fat to a large extent, so I’d think it’s beneficial as well. Regarding staying on these meds for life, I think that’s generally the plan (or at least until the next iteration of a better and safer peptide/pharmaceutical becomes available).
I guess it depends on how well tirz is working for you and how well you’re tolerating it, as well as risk tolerance since we still don’t have granular phase 3 data on reta or FDA approval.
Tirz is ok. I went up to 7.5mg a while ago and got really lean but lowered the dose after reaching target weight for that cut. I did a bulk really aiming to gain a lot of muscle so I lowered the dose. I finished that bulk, and I’m back to 7.5mg and I’m just not feeling it as much as I did the first time. I might increase dose but I’ve also been curious to try reta.