Those were suggested to me as potential methylators bc my genotype suggested that folate was not enough
You can get a blood test called RBC Folate for a more accurate measurement of your folate levels and then base your decision to use Methylfolate/folinic acid on that
I take homocystex (which I noticed they have renamed homocysteine nutrients). I has methyltetrahydrofolate also methylcobalamin and also TMG trimethylglycine. It’s been so long since I did 23 and me and found out about mthfr etc… but this convinced me to try this and it has lowered my homocysteine so I keep taking it.
Great question!
A red flag on anyone’s lab work is a high folate and a high homocysteine. This means, in general, folate isn’t getting utilized, which also indicates poor DNA methylation. The common situation is the folate >upper limit of normal.
My wife is a great example of this, homocysteine almost 30 and Folate>24. B12 normal. Pyridoxine (B6) also plays into high homocysteine, but this wasn’t going to be deficient.
We went with folinic acid 800 mcg/day, a month later, homocysteine 9.
In this situation folinic acid requires no transport receptor to get into the cell, whereas MTHF does require a receptor. There can either be a defective receptor or an antibody to the receptor. Either way, bypassing this need for a specific way to transport folate into cells is the strategy with folinic acid.
It’s not even on the list of things to do for primary care physicians or cardiologists - yet, these patients have worse health outcomes. Here is what vera-health.ai says on health risks of high homocysteine:
Elevated homocysteine levels, known as hyperhomocysteinemia, are associated with several health risks, particularly affecting cardiovascular and renal health. High homocysteine is a recognized risk factor for cardiovascular diseases, including coronary artery disease, stroke, and acute coronary syndrome (ACS). Studies indicate that elevated homocysteine can lead to major adverse cardiovascular events (MACE) and increased all-cause mortality in ACS patients 1. This relationship may be due to homocysteine’s role in endothelial dysfunction, impairing nitric oxide production and contributing to coronary microvascular endothelial dysfunction (CMED) 2.
Elevated homocysteine levels are also linked to an increased risk of thrombus formation in patients with atrial fibrillation (AF), even among those with a low CHA2DS2-VASc score. Higher homocysteine levels correlate with a significantly increased prevalence of left atrial/left atrial appendage thrombus, suggesting a potential predictive role in thromboembolism 1.
In terms of renal health, homocysteine is associated with renal function decline, particularly in hypertensive patients. It correlates with decreased estimated glomerular filtration rate (eGFR), indicating its potential role in chronic kidney disease (CKD) progression 1. Elevated homocysteine is linked to metabolic syndrome and cardiovascular events in hypertensive patients, suggesting its contribution to cerebrovascular diseases 7.
Additionally, homocysteine may influence mental health, as elevated levels have been associated with major psychiatric disorders such as schizophrenia and bipolar disorder I, though not conclusively with depression 4.
Nutritional deficiencies, particularly in folic acid and vitamin B12, can exacerbate hyperhomocysteinemia. Supplementation with these vitamins can help reduce homocysteine levels, potentially mitigating some of the associated risks 5.
In summary, elevated homocysteine levels are associated with increased risks of cardiovascular diseases, thrombus formation, renal function decline, and certain psychiatric disorders. Addressing elevated homocysteine through lifestyle changes and appropriate supplementation may help reduce these health risks.
10 Likes
I went down the methylation road for a while.
Tried methylfolate and folic acid from 250mcg to 5mg at various times.
Sometimes together with vitamin b12 and b6.
Or various b complex.
Folic acid and methylfolate lowers my mood a large % of the time.
I’ve heard it can act as a dopamine reuptake enhancer (not inhibitor) so it seems to lower dopamine, and perhaps lowers other chemicals as well.
TMG does not boost my mood, which it does for many others.
citicoline(cdp choline) is the best out of the choline products for mood and also the most expensive.
I think it is raises a few other chemicals besides acetylcholine.
I don’t know what to think because I seem to have over and under methylation symptoms.
I’ve dropped my b complex and multivitamin/mineral recently to try to improve mood.
As I’ve been using them for a very long time, and could have over used them.
Blood work has been great, so that is a plus for various vitamins/minerals/supplements etc.
However, I do have to be careful driving dopamine up too high as that can have issues also.
A maddening balance.
I sometimes wonder if my mood issues might be gaba/glutamate related instead of the monoamines.
Or something else.
Cheers ![]()
2 Likes
I had the same experience as you are describing. Folinic acid is the only thing that can lower my MCV. My only problem is that my Hemoglobin (MCH and MCHC) and doesnt normilize and I have way higher numbers than reference. Does your wife have the same problem?
My doctor keep dismissing this info but as everyone in this forum, we want to optimize and understand what is happening.
So if macrocytosis is the issue - first, I’d not get too excited. It’s typically 1 of 5 things:
#1 Folate deficiency
#2 B12 deficiency
#3 Excessive alcohol intake
#4 Myelodysplasia (all cell lines low, often macrocytosis)
#5 In a condition where one is rapidly making and releasing RBC’s, sometimes can sway the MCV up a fair bit as reticulocytes tend to have an MCV of 140.
However, if you normalized with folinic acid, it essentially proves you are not getting/utilizing folate in your cells - and this should be given life long - generally 400 mcg/day long term is plenty, to normalize things I usually go with 800 mcg/day.
Anyway, and interesting area that very few doctors have a clue in. I just wonder how you found out about folinic acid as it requires a bit of digging in.
2 Likes
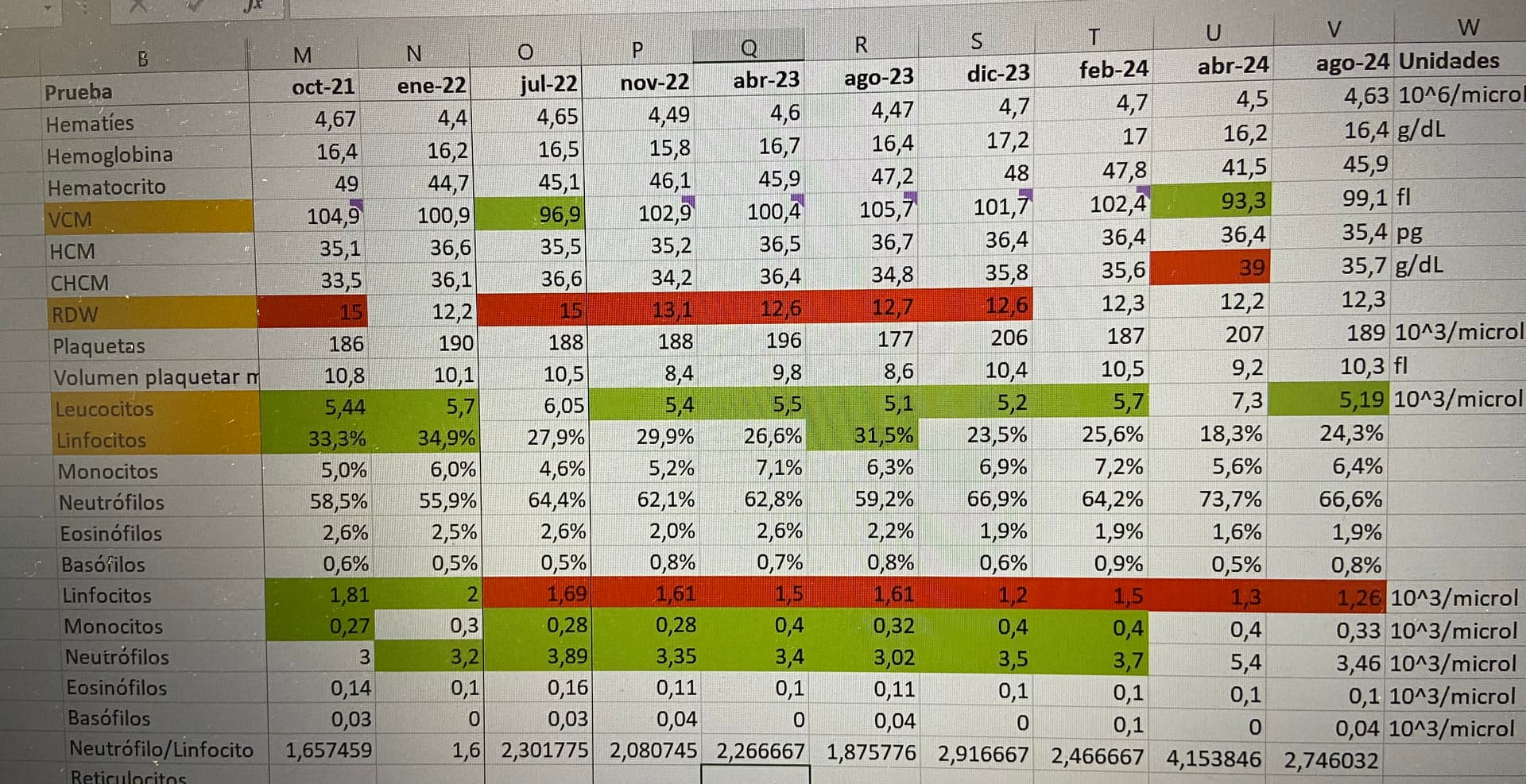
Basically after 5 years of listening to doctors advice I slowly realised that they don’t read the latest studies so I spent 4 years studying and trying different interventions. Folinic acid seemed to be at the heart of the problem so I gave it a try. My theory is that my problem it’s not solved and my super high CHCM and my Hba1c low is because a lot of red cells die. My latest interventions are trying to increase their survival.
If you are curious, here is my data. MCV of 93.3 is the folinic acid.
1 Like
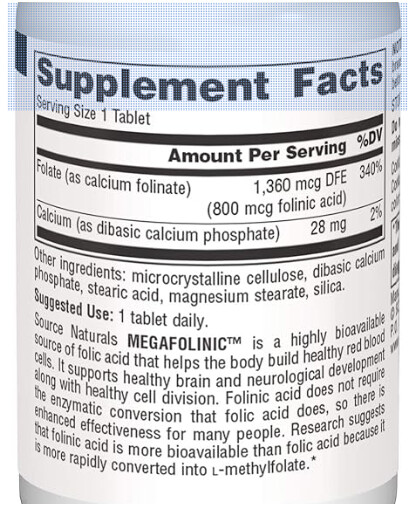
Can you recommend the brand of 800 mcg Folinic that your wife used please?
Source Naturals MegaFolinic Acid Amazon.com
Costs all of $12.84 for 3 months worth! Vitacost and iHerb also have this.
@Virachocha, In the U.S. the item labelled VCM is MCV, and the CHCM is interestingly MCHC.
The MCV and MCHC are linked and if MCV is up, pretty much your Mean Corpuscular Hemoglobin Concentration will go up as the MCV goes up (so long as you aren’t anemic).
So I’d ignore the MCHC and see how the numbers come out with at least 4 months of use of folinic acid. Remember it takes 100-120 days to have new RBC’s built and replace the existing ones, so one will know better how everything is settling with months of supplementation (and continuing this long term).
Most people in this situation (without folinic acid) also have high homocysteine which is a risk for neurocognition and vascular disease.
1 Like
Thanks for this information. My Homocyst(e)ine levels in September was 6.9 umol/L but has been up to 14 to 15 range. I take TMG and that has reduced it and I’m on L-Methylfolate (15mg) as well a a B-Complex. Do you think Folinic Acid would get my Homocysteine levels down further? If so, should I stop the Methylfolate and/or B Complex? Thoughts?
Difficult to know, I think if your homocysteine is good now, that is an indication things are doing well, it is a U shaped benefit, so go too low and you worsen health outcomes. A sweet spot 6-8 is where I’d like to be. If you supplemented with methyfolate and it fixed the homocysteine, I’d think you don’t need folinic acid, it is the folks with high homocysteine and high serum folates that I recommend this for.
1 Like
Is there a risk of using such a high dose of methylfolate long term? I definitely see a use case for a deficiency but high folate isn’t exactly good either.
I mentioned the RBC Folate blood test at the beginning of the thread. It’s a pricier test but I would imagine it would be useful in trying to find a sweet spot. Mine was once low so I took extra metylfolate and then it was great, so I stopped. Re-chuckled again years later and it was still good.
Thank you for the suggestion. I will look into this test.
calcium folinate != folinic acid
1 Like
After taking heavy doses, my Hcy INCREASED. I’ll have to do a retest without it… It is very easy to overdo with these supplements.
[and load up again on creatine and TMG].
Hi again @DrFraser! It seems that no matter the dose, if I don’t supplement with exactly 800mcg of Folinic Acid, I won’t get a reduction in MCV. I was trying to not get such a big spike in MCHC when I take the full 800mcg but it seems it’s inevitable. Do you think it is indeed a problem of quantity? Thanks for the help ![]()
| Prueba | 01/06/2019 | 01/01/2022 | 01/11/2022 | 01/02/2024 | 05/04/2024 | 01/08/2024 | 11/03/2025 | 11/06/2025 | Units |
|---|---|---|---|---|---|---|---|---|---|
| Hemoglobin | 17,2 | 16,2 | 15,8 | 17 | 16,2 | 16,4 | 16,5 | 16,4 | g/dL |
| MCV | 98,3 | 100,9 | 102,9 | 102,4 | 93,3 | 99,1 | 110,9 | 103,2 | fl |
| MCH | 35,8 | 36,6 | 35,2 | 36,4 | 36,4 | 35,4 | 37,5 | 36,9 | pg |
| MCHC | 36,4 | 36,1 | 34,2 | 35,6 | 39 | 35,7 | 33,8 | 35,8 | g/dL |
| RDW | 11,8 | 12,2 | 13,1 | 12,3 | 12,2 | 12,3 | 11,4 | 12,8 | |
| Homocysteine | 12 | 15,71 | 8,2 | mcmol/L | |||||
| Erythropoietin | 17,2 | 18,8 | mUl/ml | ||||||
| B9 | 3,96 | 7 | 7,8 | 19,8 | 8,7 | 10,43 | mcg/mL | ||
| B9 erithro | 283 | 838 | ng/mL | ||||||
| B12 | 354,5 | 454,9 | 487 | 986 | 724 | 566 | 567 | mcg/L | |
| B12 active | 117,3 | pmol/L | |||||||
| Supplemented Folinic Acid | 0 | 0 | 0 | 0 | 800 | 200 | 100 | 400 | mcg |
| Supplemented B12 | 600 | 600 | 600 | 600 | 1000 | 600 | 600 | 600 | mcg |
1 Like
Your homocysteine went from 15.7 to 8 in 3 days just because of an extra 300 mcg of folinic acid. That’s crazy.
These are not american dates, we have dd/mm/yy so it would be 3 months instead of 3 days ![]()
4 Likes