Steve_Combi, I applaud you for doing the research and testing to find what works for you. I try to do the same. I read through most of your postings, but may have missed some details. So, did you dismiss the Dasatinib + Quercetin combination as a senolytic for what you feel were better options or did you try it and find it ineffective?
1 Like
Good question.
My objective was to develop a senolytic that I would be comfortable using and for my friends and family to use. At the time I was not interested in using a drug like Dasatinib personally
My search for a “natural” compound with similar functionality to Dasatinib, a chemo drug with protein kinase and P450 3A4 Inhibitor properties, lead me to EGCG. Dasatinib is used on specific types of leukemia. If you search on EGCG and leukemia you might be surprised ![]() EGCG is also a kinase, CYP3A4 and mTOR inhibitor.
EGCG is also a kinase, CYP3A4 and mTOR inhibitor.
So I used EGCG as a substitute for D in the DQ protocol.
Q is not the best natural senolytic, Fisetin is more effective. So I decided to use both. And that is where the name of the company came from a combi-nation of seno-lytics = Combilytics!!
As I started down this rabbit hole in 2018, I came to an understanding that combinations of compounds, drugs, etc that achieve a similar result through different pathways can be more effective overall. This methodology is often used in the pharma world.
The real trick was understanding the dosing of Q that was used in the 2 successful Phase 1 trials. It’s important to pay attention to the details ![]() as they reveal that the effective dose is closer to 12 grams of “normal” Q per daily dose. People using 500mg or even 2,000mg of regular Q are not using enough for senolytic activity. Due to the low bio-availability of all polyphenols.
as they reveal that the effective dose is closer to 12 grams of “normal” Q per daily dose. People using 500mg or even 2,000mg of regular Q are not using enough for senolytic activity. Due to the low bio-availability of all polyphenols.
The successful trials used a more bio-available liposomal Q from Thorne and even then at a high dose that is poorly understood by most. This why most trials run by others, since the 2 successful ones I’ve referenced, often miss the mark, they didn’t seem to understand nor duplicate the methods used in the successful trials.
3 Likes
Not only does it work for me but it worked for 4 random strangers who did a 7 month “evaluation” with before and after Trudiagnostic tests that showed every person experienced moving the needle back in 1 or more of the markers that test covers.
1 Like
Qualia’s stuff is shockingly expensive. I haven’t tried it but I’m tempted to try their nootropic since my Fullscript site provides a big discount.
4 Likes
EGCG is also an HDAC inhibitor.
1 Like
One issue is that no one really knows their senescent cell count. All we know for sure is they exist, they have an immortal quality, they accumulate because of that immortality, they emit both harmful and helpful SASP, they multiply because of SASP and clearing them has demonstrated a benefit in 2 disease conditions.
I do not have either of those diseases BUT I do have senescent cells.
And since we will have more senescence in one area than another (muscle vs skin will have different levels of senescence) the “may only benefit” approach, while a good caveat, does not fully address the opportunity.
The only “down side” is the cost to do it right.
Same for many longevity interventions, some who may be deficient will have a higher benefit ratio to those who aren’t deficient (in that “thing”).
Many on this forum take Rapamycin, I’m in that cohort, do I need it? am I doing it “right”? will there be a long term risk? or no risk? is there a real benefit in humans for health span?
This is the nature of self hacking ![]()
If the 12 Hallmarks of Aging have any meaning, addressing as many of the 12 as possible, at the root cause level, should help us at least extend health span. Senescence is a root cause.
Personally I’m not terribly concerned about longevity.
2 Likes
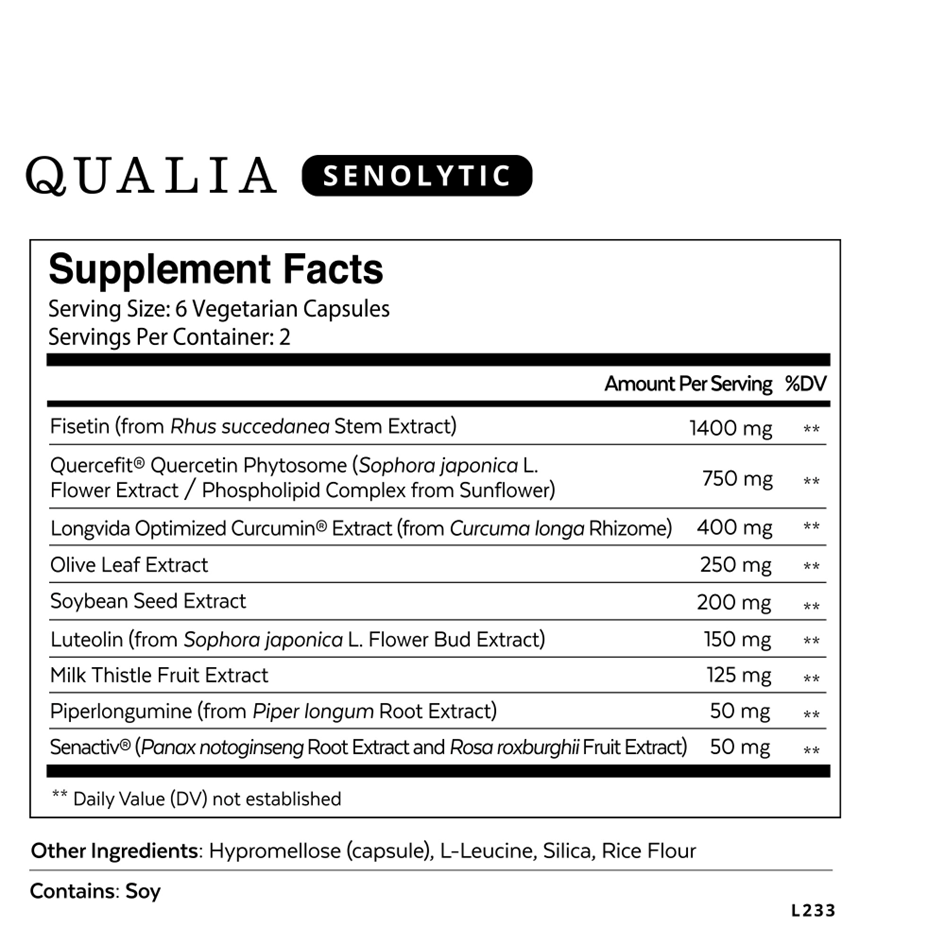
Several of the substances target a specific aspect of senescence, such as in muscle, intervertebral disks, chondrocytes or oxidation resistance. Besides the well known quercetin and fisetin, I checked each of them and the research backs up senolytic action. However most is in vitro, one or two on rats, but two with clinical trials in particular Senactiv on muscle senescence is notable.
Qualia appears to have taken care in its formulation. A trial shows the quercetin it uses has around 15 times higher bioavailability than unformulated quercetin.
But only action in humans counts. With the caveat that it was funded by the company behind it, I think there is merit to the double-blind, placebo-controlled human clinical trial on people aged 35-79 with moderate joint health/performance issues. The placebo response was large but the response from the senolytic formulation was significantly larger in the primary endpoint, joint health. Of eight other health aspects, there was no change between placebo and senolytic in four. The senolytic was non-significantly better in the other four, with two including energy trending toward significance p<0.10.
Qualia Senolytic Placebo-Controlled Clinical Study Results (qualialife.com)
1 Like