The characteristic enhancer usage and transcriptional landscape of high-passage senescent cells are sensitive to rapamycin treatment, discontinuation of which results in robust but selective senescent enhancer activation and exacerbation of the SASP
Damn… the great results of rapamycin tamping down senescent cells was undone after a few weeks of discontinued treatment.
Because rapamycin treatment seemed to prevent certain features of senescence even in proliferatively arrested cells, we investigated whether these changes were stable upon rapamycin withdrawal.
HPGA cells withdrawn from rapamycin treatment reverted to a senescent-like state just 2 wk after drug removal, with a dramatic onset of senescent morphology and increased SA-β-gal staining (Fig. 2C and SI Appendix, Fig. S2B). RNA-seq of HPGA cells withdrawn from rapamycin versus those maintained in rapamycin showed a clear correlation between the genes induced upon rapamycin withdrawl.
Wasn’t there some study reported widely on this site that even one dose (or short term use) of Rapamycin could possibly provide the maximal life extension benefits? I understand that lifespan extension is different than health span, so living with increased SASPs may contribute to a worse health span, while still conserving the increased lifespan. Nonetheless, I find this report confusing/ disappointing.
Not to add another topic, but I also heard something about plasma withdrawal or donation (I think without adding back albumin) was recently found to accelerate aging in some way, rather than reducing aging.
All to say, I am starting to wonder if a lot of the more cutting edge, aggressive stuff that I do is actually detracting from my health. This comes up for me when I hear about these negative studies or see people like Asprey (who IMO does not radiate a youthful or healthy appearance) despite unlimited access and focus on his health.
Of course, my pessimism only lasts until the next strong positive study sparks my interest and buoys my optimism. But for today, my resolve is to refocus on the basics.
Direct take-aways for a 6 mg-weekly rapamycin user who plans a 3-month drug holiday
Aspect
What the paper shows
What it probably means for your regimen
mTOR inhibition blunts both the “growth-arrest” and the “SASP” enhancer programs of senescent fibroblasts
Continuous 500 nM rapamycin for ≥2 weeks erased H3K27ac on both enhancer sets and kept SASP genes low.
While your 6 mg weekly pulse will not produce the same constant exposure, it almost certainly lowers mTOR signalling for part of each week. Expect some degree of SASP suppression during the months you stay on drug.
Withdrawal re-primes the enhancer landscape, with a disproportionate rebound of the SASP module
Two-week wash-out triggered a surge of p65 binding and H3K27ac on the SASP enhancers; inflammatory transcripts (IL-6, IL-8, etc.) jumped, whereas the cell-cycle-arrest program stayed locked-on.
After you stop rapamycin for 3 months, existing senescent cells could up-shift their inflammatory output while remaining growth-arrested. In practical terms, systemic low-grade inflammation might rise for a while—even though your tissues will not suddenly start proliferating abnormally.
Rapamycin does not delete senescent cells
It merely dampens their enhancer activity. Stopping the drug leaves the same number—or more—senescent cells in place, now free to make SASP factors.
If your aim is to reduce senescent-cell burden, rapamycin alone is insufficient; consider pairing with bona-fide senolytics or shorter holidays.
Ligand loops matter
Withdrawal boosts TGF-β2-driven, p65-dominated enhancers; Activin-A-driven arrest enhancers stay on.
Any systemic rise in TGF-β family ligands or NF-κB activation during your drug holiday could amplify SASP rebound. Lifestyle factors that quell NF-κB (exercise, weight control, omega-3, etc.) may buffer this.
Translation caveats
Findings are in vitro fibroblasts, continuous drug, supraphysiologic dose; human weekly pulses haven’t been mapped at enhancer level.
Magnitude of rebound in vivo is unknown; systemic biomarkers (CRP, IL-6) or “deep aging” panels might help you see if a flare actually occurs.
Practical implications (no spin)
During the on-phase (weekly 6 mg for several months)
Their SASP program may re-engage and even overshoot baseline for a time.
Clinical impact could range from trivial to a measurable uptick in inflammatory markers—data in humans are lacking (confidence: low-medium).
Mitigation strategies worth considering (evidence outside this paper)
Shorter holidays (e.g., 6–8 weeks) or alternating low-dose instead of a full stop.
Pairing the break with senolytics (dasatinib + quercetin, fisetin) or anti-inflammatories (low-dose NSAID, omega-3) if tolerated.
Tracking CRP, IL-6, or a commercial SASP panel before, during, and after the holiday to see if rebound is real for you.
Unknowns & limitations
Weekly pulses ≠ continuous exposure; the rebound could be muted—or already occurring between doses.
Only fibroblasts studied; other tissues may behave differently.
No clinical endpoints (frailty, cognition) tested.
Bottom line: The paper supports the idea that stopping rapamycin can let senescent cells crank up inflammatory SASP without re-entering the cell cycle. In a real-world weekly-pulse protocol, that rebound is plausible but unquantified. Continued biomarker monitoring is the only way to know if your planned 3-month holiday carries an inflammatory cost.
Because nobody knows for sure how to dose rapamycin, it’s all guesswork, and no data supports any of the regimens for longevity purposes.
I myself do not cycle as much other than low dose regularly. My biomarkers have either improved or stayed the same. Subjectively, I feel better. And with grey hair turned into black (not all but more than half).
I suspect it accelerated my facial fat loss, although not significantly; it was noticeable.
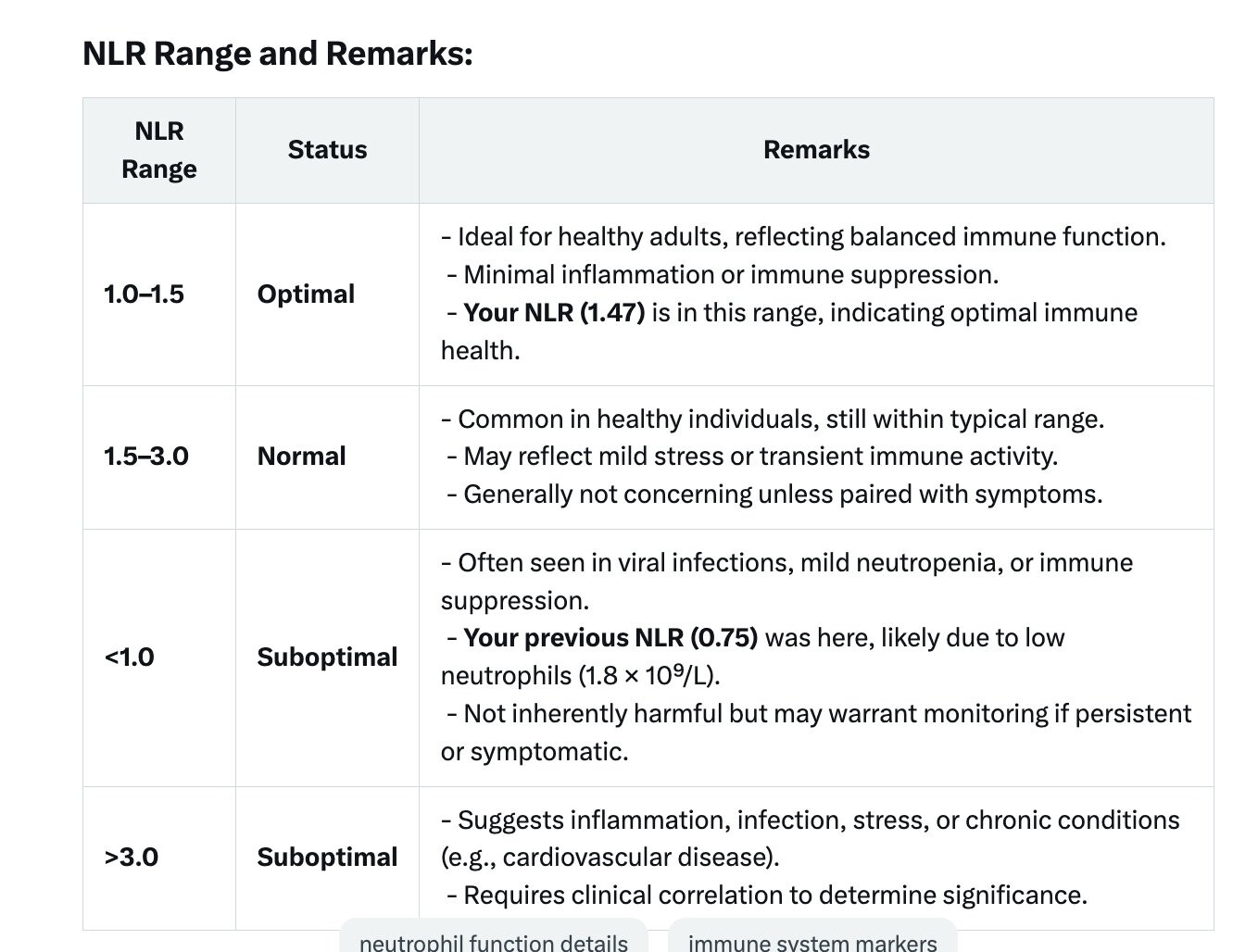
I monitor my NLR ratio to be close to 1 as a benchmark of my immune system’s balance.
Here’s where I read about it. It doesn’t negate benefits for folks paying for TPE protocols where they get replacement with albumin, but it certainly gives pause to the DIY’ers, like me, who thought they could get away with a freebie by donating plasma. We still might be reducing our forever chemicals, but at what cost to our anti-aging regimen.
Plasmapheresis is a medical procedure that separates plasma from blood cells, potentially removing pro-aging factors from circulation. Some studies suggest it may have rejuvenating effects by altering biomarkers of aging, but evidence on its impact on epigenetic aging in humans is limited. This study aimed to assess whether plasmapheresis without volume replacement with young plasma or albumin affects epigenetic age and other biomarkers in healthy adults. An automatic plasma collection system, the Haemonetics PCS2, was used for plasmapheresis. Healthy blood donors were divided into two groups using stratified randomization in a cross-over study with subjects undergoing either 8 plasmaphereses (8 pp) or 4 plasmaphereses (4 pp) for an 18-week period, with a minimum interval between plasmaphereses of 2 weeks (14 days). Samples were tested for biochemical, hematological analyses and epigenetic clocks. We documented the alteration in serum minerals, decreased serum lipids, mainly total cholesterol, non-HDL, triglycerides, apolipoprotein A levels, total proteins and albumin. Among hematologic parameters, we found an increase in Red Cell Distribution Width (RDW) and Mean Corpuscular Hemoglobin Concentration (MCHC). No significant epigenetic rejuvenation was observed based on epigenetic clock measurements. Instead, plasmapheresis was associated with increases in DNAmGrimAge, the Hannum clock, and the Dunedin Pace of Aging. Plasmapheresis can rapidly change the levels of pro-inflammatory and other pro-aging molecules in the circulation. However, the selected protocol has not provided conclusive data supporting benefits. Based on epigenetic clock parameters, it may accelerate epigenetic aging. More research into the long-term safety of this specific protocol is needed.
I think this paper makes a valid point for weekly or more frequent Rapamycin dosing. Remember that SASPs increase senescent cell proliferation which allows the faster creation of senescent cells.
Most probably, using Rapamycin retards senescent cell formation and gives your body more time to clear out senescent cells. I’ll make sure to stay on a weekly dosing of 3 mg + GFJ (10.5 mg equivalent).
It’s 2 mg every other day. Is it continuously or you have breaks? With such dose you must be pretty much immunosuppressed all the time like in transplant patients. Any sides?
I would like to know it myself. All other biomarkers are almost the same and in a normal range. Have nothing outstanding or abnormal. Same diet, same exercise, same sleep, same supplements. Excluded th
melatonin (couldn’t fall asleep with it), but don’t think it’s a factor.