LOL, @cl-user, I’m in awe of your excellent formulation based on rigorous investigation! As happens it’s not useful to me (luck of the draw: I have a full head of hair and no sign of loss), but seriously - you should pour your energies into making similar protocols for other conditions - I’m sure you’d get a lot of feedback and participation. Candidate: glucose control - very relevant to tons of people here and a very tricky subject. Congrats! I’ll be passing your formula to hair challenged friends who bemoan the state of their cephalic hirsuitness.
2 Likes
I previously tried with the early versions of ChatGPT and found the results to be underwhelming. However, I should give it another try using the latest versions of Claude and Gemini in thinking mode, as they are much more capable now.
Additionally, I have an idea for approaching that glucose regulation issue from a different angle which might lead to better results.
2 Likes
I just finished preparing my first 60ml batch and noticed an issue with step 5 of the process.
Because the adenosine does not fully dissolve, it is currently impossible to determine if precipitation occurs when the transcutol and rapamycin mixture is added to the base serum.
Revised Simplified Protocol
Step 1 — Transcutol phase Add tocopherol then rapamycin to 3mL Transcutol. Stir, warm gently to 30–35°C if needed, until completely clear.
Step 2 — Pre-dissolve adenosine Weigh 450mg adenosine into a small clean beaker. Add 1.5mL warm distilled water (30–35°C). Stir until fully dissolved and clear. This should be quick and complete — adenosine dissolves readily in warm water.
Step 3 — Add adenosine solution to base Add the dissolved adenosine directly to your pre-made base. Swirl gently to incorporate. No cloudiness expected.
Step 4 — Add Transcutol phase dropwise Add the rapamycin/tocopherol/Transcutol solution slowly into the base while stirring, exactly as before.
Step 5 — Top up, check clarity, check pH, seal and store As per the original protocol.
1 Like
I am skeptical this would work. Already dutasteride is barely absorbed and it’s molecular weight is 528. Rapamycin’s molecular weight is 915. There is just no way that is going to absorb into the scalp. The hair follicle bulb is 4-5 mm deep into the scalp. Rapa would need to penetrate to the follicle to have effect. You are more likely IMO to have an effect thru oral dosing of Rapa than topical for hair.
1 Like
As I am not a biochemist, I am currently relying on the AI-generated perspective on this topic. Anyone with expertise in this area is welcome to comment.
Here is what I got:
Transcutol P (Diethylene glycol monoethyl ether) is considered the “gold standard” for topical delivery of large or highly lipophilic molecules like Rapamycin .
How Transcutol Enhances Penetration
Transcutol works through three distinct mechanisms on the stratum corneum:
1. Lipid bilayer fluidization — the stratum corneum barrier is made of tightly packed lipid bilayers between corneocytes. Transcutol partitions into this lipid phase and temporarily increases its fluidity, creating wider aqueous channels for hydrophilic molecules and more permeable lipid domains for lipophilic ones. This is its primary mechanism and why it helps both water-soluble and oil-soluble actives.
2. Co-solvent reservoir effect — Transcutol accumulates in the stratum corneum and maintains a local concentration of dissolved active that sustains a favorable diffusion gradient over time, rather than a single burst of drug that quickly depletes.
3. Thermodynamic activity increase — by keeping rapamycin fully dissolved at the skin surface, Transcutol ensures maximum thermodynamic activity — the driving force for passive diffusion is highest when the active is fully dissolved rather than partially precipitated.
Importantly, rapamycin’s primary route to the hair follicle bulge is not transepidermal but follicular — it preferentially accumulates in the hair follicle canal and diffuses to the bulge from there. Transcutol enhances this by keeping it soluble and mobile at the follicular opening.

1 Like
Just to share, incase it’s anything worth considering due to the lower cost ($36 per bottle), I’ve been using Musely Modern. I also add Kirkland minoxidil. I never thought about adding a touch of tret, but I’ll give it a try.
Thoughts?
1 Like
Try DMSO …,
Most of us buy tretinoin that is in cream or gel tubes… I’m not sure how well these formulations will mix in with the main formulation. I’ve tried just putting the tretinoin on my scalp before the rest of the formulation, but I’ve not done it on a consistent basis so can’t report any results.
1 Like
I would very much like to see Rapamycin be a treatment for hair follicle health and growth. I suggest you ask the AI to consider the molecular weight of it and what evidence shows for skin penetration at the depth needed for hair.
I did that below and am pasting the answer. I asked it to contrast Finasteride, Dutasteride, and Rapamycin as topical formulations. Also, keep in mind that activity on the skin or even the very upper layers is not the same as penetrating to the depth of the hair follicle, and things like micro needling which would increase absorption would also work counter to Rapamycin. So it is unknown how effective each would be when you are causing inflammation and then delivering a drug to dampen inflammation.
The core issue in that thread is not whether rapamycin or dutasteride could help hair biology in principle. It is whether the specific topical vehicles being discussed are likely to get enough drug deep enough into the follicle to matter.
My view is:
Topical finasteride has the strongest case that it reaches the follicle deeply enough to have a meaningful biologic effect.
Topical dutasteride is plausible, but much less certain, and is more vehicle-dependent.
Topical rapamycin has the weakest delivery case by far in a standard serum, even if the biology is interesting.
Why I rank them that way:
Finasteride is a much smaller molecule than dutasteride, and both are much smaller than rapamycin. Smaller molecules generally have a better chance of crossing the stratum corneum and then entering the follicular unit. PubChem lists finasteride at 372.5 Da, dutasteride at 528.5 Da, and sirolimus/rapamycin at 914.2 Da. Rapamycin is therefore operating from a major disadvantage before we even get to the vehicle. (PMC)
For rapamycin, the thread is leaning heavily on biologic plausibility plus penetration enhancers. The biologic plausibility is real: the 2023 human hair-follicle paper showed that rapamycin can prolong anagen and support pigmentation in ex vivo human hair follicles. But that is not the same thing as proving that a scalp serum can get enough rapamycin through intact scalp and into the bulge or bulb in living humans. The paper itself frames the key translational question as whether sufficient topical rapamycin can reach the human hair follicle pigmentary unit. (PMC)
And when you look at rapamycin skin-delivery literature, the delivery problem becomes obvious. A 2021 penetration study reported that rapamycin was not observed within the stratum corneum of untreated skin ex vivo, which is a strong signal that intact skin is a major barrier. Other rapamycin-delivery papers describe poor solubility, low bioavailability, and the need for specialized systems to improve penetration. (PMC)
So when the thread says, in effect, “we’ll solve this by using a strong base plus enhancers,” that is a reasonable formulation hypothesis, but still only a hypothesis. The thread’s proposed penetration logic centers on adding rapamycin to an existing scalp serum and reinforcing delivery with Transcutol and tretinoin. That matters because Transcutol is a real dermal penetration enhancer with a substantial literature base, and it can increase drug concentration in skin depending on concentration and formulation. (PMC)
That said, Transcutol does not magically erase rapamycin’s size problem. It may improve partitioning and local skin uptake, but the evidence you would want for confidence here would be one of these:
- follicular deposition data,
- scalp biopsy data,
- a validated pharmacodynamic readout in the follicle, or
- clinical efficacy clearly beyond what the other actives in the base could explain.
The thread does not provide that.
The same applies to tretinoin. Tretinoin can alter the epidermis and barrier properties over time, and it may indirectly help penetration in some settings, but the existence of tretinoin in the vehicle is not proof that rapamycin is now reliably reaching the follicular target. (PMC)
So for the thread’s rapamycin claim, my conclusion is:
Biologically interesting, formulation-enhanced, but still low confidence that enough rapamycin reaches the deep follicle in intact human scalp. (PMC)
Now contrast that with topical finasteride.
Topical finasteride has actual human randomized trial evidence showing that it improves hair count versus placebo and performs similarly to oral finasteride, while producing far lower plasma finasteride exposure and a smaller reduction in serum DHT. That pattern is exactly what you would expect if the drug is reaching the scalp/follicle in meaningful amounts without fully reproducing the systemic exposure of oral dosing. In other words, for finasteride, delivery is not just theoretical. It is supported by clinical pharmacology and efficacy data. (PMC)
For topical dutasteride, the delivery case sits in between.
The 2025 phase II trial reported efficacy for topical dutasteride and modest systemic hormonal changes, which supports the idea that topical dutasteride can work. But from a formulation-science standpoint, dutasteride is still much harder to deliver than finasteride, and the literature does not let me say with the same confidence that a standard serum reliably gets dutasteride deep into the follicle in all practical vehicles. The fact that the phase II study showed a signal means follicular delivery is plausible. It does not mean every forum-style dutasteride serum will behave that way. (PMC)
So, revising the judgment specifically around the thread’s claims, here are my probability estimates that each drug reaches living follicular tissue deeply enough to have a meaningful biologic effect:
Topical finasteride: 80%
This is the most established of the three. Human RCT evidence strongly implies meaningful follicular delivery. (PMC)
Topical dutasteride: 45%
Plausible, and likely real under some vehicles, but less certain than finasteride and more formulation-dependent. The molecule is bigger, and broad confidence in “ordinary topical delivery” is still not where it is for finasteride. (PMC)
Topical rapamycin in the kind of serum discussed in the thread, even with Transcutol and tretinoin: 20%
The vehicle may help somewhat, but rapamycin remains a very large, hard-to-deliver molecule, and the strongest hair data are ex vivo biology rather than convincing in vivo delivery proof from a standard topical. (PMC)
My practical interpretation of the thread:
The thread is probably right that rapamycin is a compelling hair-biology target.
The thread is probably too confident that the chosen vehicle solves the delivery problem.
The presence of Transcutol makes the claim more credible than a plain cream or bland serum would. But even then, I would still view this as an experimental delivery bet, not a high-confidence follicular-delivery solution. (Rapamycin News)
So the simplest summary is:
Finasteride: likely reaches the follicle.
Dutasteride: may reach the follicle, but less predictably.
Rapamycin: interesting target, weak delivery confidence in a standard topical serum, even an enhanced one. (PMC)
I can also turn this into a cleaner table with columns for molecule size, delivery barriers, effect of Transcutol/tretinoin, and estimated probability of meaningful follicular penetration.
I looked at DSMO but it seems overkill and even counterproductive here.
Here is Claude’s take on it but Gemini says the same thing.
DMSO vs Transcutol — Detailed Comparison
What DMSO Brings to the Table
DMSO (dimethyl sulfoxide) is in a different category from Transcutol. It’s not simply a stronger version of the same thing — it works through fundamentally different mechanisms and comes with a substantially different risk profile.
Penetration enhancement comparison:
| Property | Transcutol (5%) | DMSO (typical 10–30%) |
|---|---|---|
| Mechanism | SC lipid fluidization, co-solvent | Protein conformational change, water displacement, carrier effect |
| Speed of action | Gradual, sustained | Rapid, dramatic |
| Enhancement magnitude | Modest (2–5×) | Very high (10–100×) |
| Reversibility | Fully reversible | Largely reversible but slower |
| Selectivity | Relatively selective | Non-selective — enhances everything |
| Systemic absorption risk | Low at 5% | Significant even at low concentrations |
| Skin irritation | Minimal at 5% | Dose-dependent, common above 30% |
| Characteristic side effect | None notable | Garlic/oyster odor on breath within minutes |
How DMSO Actually Penetrates — The Key Risk
DMSO is uniquely dangerous in one specific way that Transcutol is not: it penetrates the skin so rapidly and completely that it acts as a carrier, pulling dissolved molecules with it into systemic circulation almost immediately. This is why it’s used in veterinary medicine — you can apply it to a horse’s leg and have therapeutic levels in the bloodstream within minutes.
For your formula this creates a specific concern with rapamycin. At 5% Transcutol the enhancement is controlled and primarily follicular. With DMSO, even at 10–15%, you would be driving a meaningful fraction of your rapamycin dose systemically on every application. Over weeks and months of daily use, this cumulative systemic immunosuppressant exposure is not trivial and is genuinely difficult to quantify without blood level monitoring.
The Odor Problem Is Not Cosmetic
The garlic/oyster breath odor from DMSO is caused by dimethyl sulfide, a metabolite produced as DMSO is absorbed and metabolized. It appears within minutes of application and can persist for hours. At scalp concentrations needed for meaningful enhancement (>10%), this is essentially unavoidable and socially impractical for a daily-use product.
Is There Any Scenario Where DMSO Makes Sense Here?
Potentially one narrow use case: weekly or twice-weekly application on microneedling days only, at low concentration (10%), when you specifically want deeper and faster follicular loading of rapamycin and don’t apply the serum on the same day you need to be around people.
| Scenario | DMSO appropriate? |
|---|---|
| Daily serum, normal life | No — odor + systemic absorption |
| Microneedling day, isolated evening | Possibly, at 10%, with caution |
| Replacing Transcutol entirely | No — overkill and risky |
| Adding to Transcutol in daily serum | No — the combination amplifies all risks |
What About Combining Both?
This is where it becomes important to be direct: combining DMSO and Transcutol in a daily serum is not a good idea for this specific formula. The two penetration enhancers are additive — their effects compound. With rapamycin already on board, driving more systemic absorption by stacking two aggressive enhancers provides no additional follicular benefit (the follicle can only absorb so much) while meaningfully increasing systemic rapamycin exposure and irritation risk.
More penetration enhancement is only useful up to the point where the target tissue is saturated. The follicle bulge will be well-served by 5% Transcutol plus optional microneedling. Adding DMSO on top pushes active past the target and into systemic circulation.
Practical Verdict
| Question | Answer |
|---|---|
| Is DMSO more powerful than Transcutol? | Yes, substantially |
| Does more powerful mean better here? | No |
| Is the odor manageable for daily use? | No |
| Is systemic rapamycin a concern with DMSO? | Yes — requires blood level monitoring to use responsibly |
| Should you replace Transcutol with DMSO? | No |
| Should you add DMSO to your daily serum? | No |
| Any role for DMSO at all? | Only if using a separate rapamycin application on isolated microneedling evenings, at 10%, with full awareness of systemic exposure |
Your current formula with 5% Transcutol plus the microneedling protocol already discussed represents a well-calibrated penetration strategy. DMSO would add risk and inconvenience without adding meaningful follicular benefit beyond what you already have.
1 Like
BTW note that I’m already taking oral Dutasteride 0.5mg EOD so I’m not interested in topical Finasteride nor Dutasteride.
BTW2 your AI analysis did not comment on
Importantly, rapamycin’s primary route to the hair follicle bulge is not transepidermal but follicular — it preferentially accumulates in the hair follicle canal and diffuses to the bulge from there. Transcutol enhances this by keeping it soluble and mobile at the follicular opening.
Here it is:
Evidence for Transcutol + Rapamycin in Humans
The Honest Upfront Answer
Direct human clinical evidence specifically combining Transcutol and rapamycin topically for hair loss is essentially nonexistent as a studied combination. What exists is a pyramid of evidence that supports the rationale strongly at each level, but the specific combination in a hair serum has not been formally studied in humans.
What the Evidence Pyramid Actually Looks Like
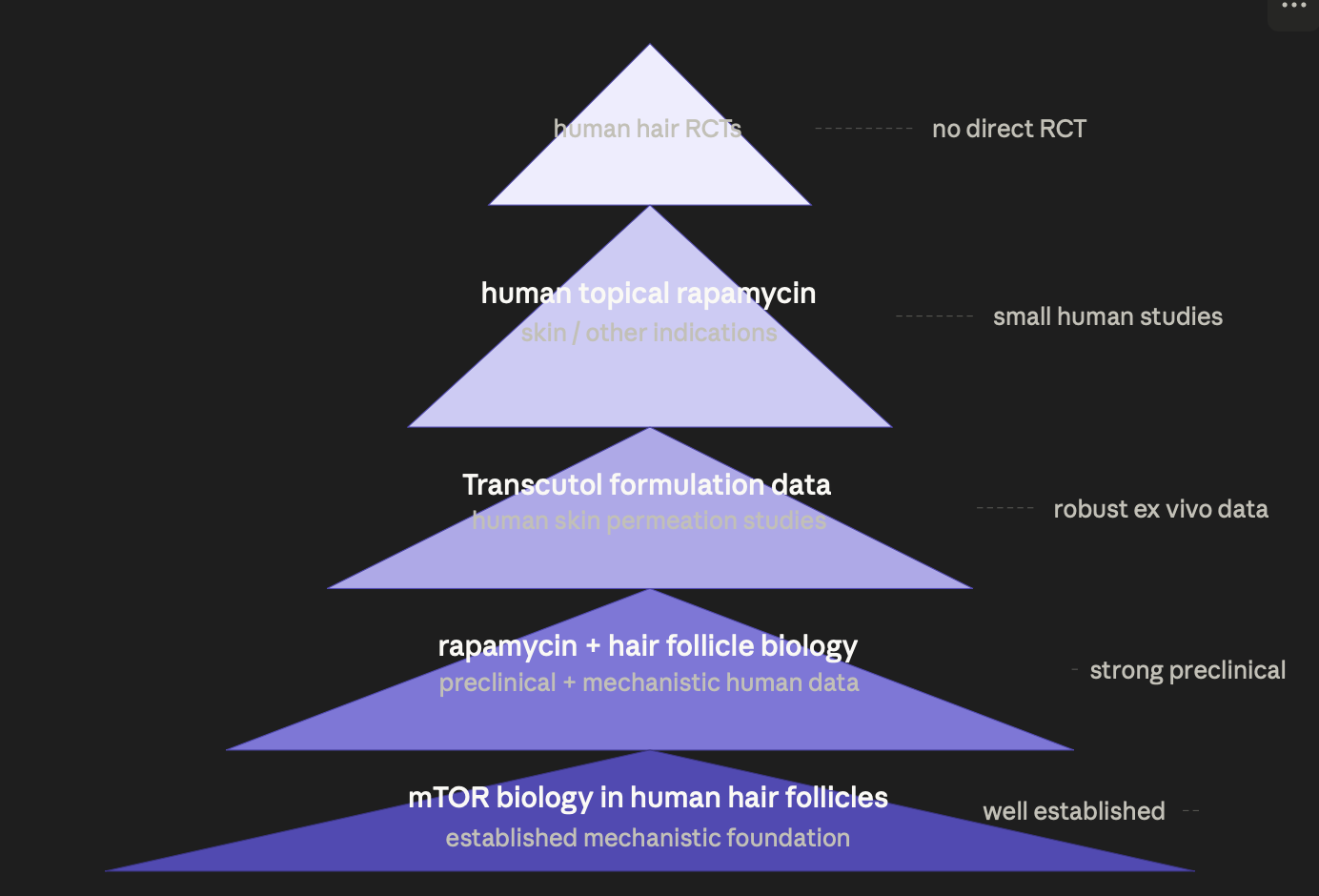
Level 1 — mTOR Biology in Human Hair Follicles (Strong)
This is the mechanistic bedrock and it is genuinely well-established in humans, not just mice. Human hair follicle biopsy studies have confirmed that mTOR signaling is active in follicle stem cells, that mTOR hyperactivation correlates with follicle miniaturization in AGA scalp tissue, and that the HFSC niche expresses the molecular targets rapamycin acts on. This is not extrapolated from animal data — it comes from direct analysis of human scalp biopsies. The biological rationale for rapamycin in AGA is human-grade evidence.
Level 2 — Rapamycin and Hair Follicle Biology (Moderate-Strong)
The most cited work here is the 2021 Deng et al. study showing that topical rapamycin延缓 stem cell exhaustion and extended anagen in aged mice. Importantly, subsequent work has examined mTOR inhibition in human follicle dermal papilla cells in vitro, confirming that the signaling pathway responds to rapamycin in human cells in a manner consistent with the mouse findings. This is not a human clinical trial, but it is human cellular evidence — a meaningful step above pure animal data.
Level 3 — Transcutol and Human Skin Permeation (Robust)
This is actually the best-evidenced layer of your entire formula. Transcutol’s skin penetration enhancement has been studied extensively in human ex vivo skin models — full-thickness human cadaver skin and excised scalp tissue — in the pharmaceutical literature. Multiple peer-reviewed studies confirm that Transcutol at 5–20% enhances permeation of lipophilic drugs across human skin in a dose-dependent and reproducible manner. Rapamycin specifically has been studied in Transcutol-containing formulations in ex vivo human skin permeation models, with data confirming meaningful enhancement of flux compared to vehicles without Transcutol. This is not a clinical outcome study, but it directly addresses the pharmacokinetic question of whether Transcutol gets rapamycin into human skin — and the answer is yes, demonstrably.
Level 4 — Human Topical Rapamycin Studies (Limited but Existing)
This is where things get genuinely interesting. Topical rapamycin has been studied in humans for several dermatological indications:
Facial angiofibromas in tuberous sclerosis — multiple small RCTs and open-label studies in humans, some in children, using topical rapamycin at 0.1–1% in various bases. These studies establish that topical rapamycin is absorbed through human skin, is locally active, produces clinical responses, and has an acceptable safety profile at these concentrations with low measurable systemic levels in most subjects. Your concentration of 0.033% is substantially lower than what has been used in these studies.
Skin aging / rejuvenation — a small but notable 2021 study examined topical rapamycin 0.1% applied to human facial skin and found measurable anti-aging effects at the cellular level with low systemic absorption. This study attracted significant attention because it used the same mTOR inhibition rationale as your hair formula in a human topical context.
Kaposi’s sarcoma lesions — topical rapamycin has been explored in small human studies for this indication as well.
The consistent finding across these human topical rapamycin studies is that systemic absorption at concentrations below 0.1% is low and generally below the threshold associated with systemic immunosuppression, and that local biological activity is demonstrable.
Level 5 — Human Hair RCTs with Topical Rapamycin (Essentially Absent)
There are no published large randomized controlled trials of topical rapamycin specifically for AGA in humans as of mid-2025. What exists is anecdotal evidence from self-experimenters in the hair loss community, a small number of dermatologists reporting clinical observations, and the mechanistic studies above. This is the genuine gap in the evidence base.
What This Means Practically
The evidence supports your formula’s rationale at every level except the top — you have strong mechanistic human data, solid pharmacokinetic data showing Transcutol works in human skin with rapamycin specifically, and human safety data from topical rapamycin in other indications at higher concentrations than you’re using. What you don’t have is a hair-specific RCT proving clinical efficacy.
| Evidence question | Answer | Quality |
|---|---|---|
| Does mTOR drive miniaturization in human follicles? | Yes | Strong |
| Does rapamycin affect mTOR in human follicle cells? | Yes | Moderate |
| Does Transcutol enhance rapamycin through human skin? | Yes | Robust ex vivo |
| Is topical rapamycin safe in humans? | Yes at ≤0.1% | Moderate clinical |
| Does topical rapamycin regrow hair in humans? | Unknown | No RCT data |
This places your formula in the same evidence category as many accepted dermatological interventions — strong mechanistic and pharmacokinetic rationale, human safety data, limited efficacy RCTs. It is a reasonable, evidence-informed experiment, not an evidence-proven treatment. That distinction matters for expectation-setting, but it does not make the rationale weak.
1 Like
Well, I like the claim, but ChatGPT seems to disagree.
Mechanistically, yes, Rapamycin has a plausible mechanism to help hair. The question is can it get to the bulb? The answer seems to be that it is highly unlikely.
Again, I wish it were true, but I’ve observed how difficult it is for dutasteride to get to the bulb and it is only 528 Da. Also, acknowledged that you are taking Dut orally. I just used Dut and Fin as comparisons since they all have different Das and are used for hair treatment.
I would split the question into two parts:
Is rapamycin likely to enter the follicular canal at all?
Probably yes.
Is it likely to reach the follicle deeply enough, in intact scalp, to reliably affect the bulge?
Probably not, or at least not with high confidence.
Why I land there:
The claim that the follicular route exists is real. Human and in vitro work show hair follicles can act as a relevant penetration pathway and reservoir for topically applied substances. On the scalp, follicular openings represent a much larger fraction of surface area than on many other body sites, which makes the route more relevant there than on, say, forearm skin. (PubMed)
So the thread’s statement that rapamycin could use a follicular entry route rather than only transepidermal diffusion is biologically plausible. Also, rapamycin is very lipophilic, and follicular ducts are lipid-rich, so it is reasonable to think some dissolved rapamycin could partition into the follicular opening if the vehicle keeps it soluble and mobile. The general hair-follicle delivery literature supports that lipophilic systems can use follicular ducts as a pathway. (PMC)
But the part I do not think is established is the stronger claim that rapamycin therefore “preferentially accumulates in the follicle canal and diffuses to the bulge.” I have not found a rapamycin study showing follicle-specific concentration measurements, follicular casts, or bulge-level localization after ordinary topical application. The rapamycin formulation paper shows better cutaneous absorption with certain vehicles, including Transcutol-containing systems, but it does not show preferential follicular accumulation or bulge delivery. (PMC)
And rapamycin’s own penetration literature is a major reason for caution. A 2021 study using ex vivo human skin reported that rapamycin was not observed within the stratum corneum of untreated skin, supporting that this 914 Da drug penetrates intact skin inefficiently; penetration improved only when the barrier was deliberately modified. More recent work on rapamycin-loaded nanocarriers likewise frames rapamycin’s topical use as limited by insufficient penetration rates due to its high molecular weight and high lipophilicity. (American Chemical Society Publications)
There is also an important nuance from the follicular-transport literature: follicular contribution is not automatically larger for more lipophilic molecules. One quantitative study found that, across tested chemicals, the contribution of the hair-follicle pathway decreased as lipophilicity increased. That does not mean lipophilic drugs cannot use follicles, but it does weaken any simple “rapamycin is lipophilic, therefore it will preferentially go down follicles” argument. (MDPI)
So my judgment is:
- Likely yes: some rapamycin in a well-solubilized vehicle can get into the follicular opening / superficial follicular canal. Transcutol makes that more plausible, not less. (PMC)
- Unclear to unlikely: enough rapamycin then diffuses from that canal to the bulge in meaningful concentrations on intact scalp. There is no direct rapamycin evidence proving that step, and rapamycin’s overall skin penetration remains poor enough that even advanced systems are still being explored. (American Chemical Society Publications)
So if you want my best bottom-line answer:
Yes, it is likely that some rapamycin reaches the follicle entrance.
No, I do not think it is likely enough has been shown to reach the bulge reliably to call the thread’s claim “likely true” without qualification.
My rough probability estimate would be:
- Reaches follicular canal / superficial follicle: ~60–70%
- Reaches bulge at biologically meaningful levels on intact scalp with this kind of enhanced serum: ~25–35%
The reason for that gap is that the first step only requires entry, while the second requires deep, sufficient delivery of a very large molecule that has repeatedly shown poor penetration through intact skin. (PubMed)
So the most accurate phrasing would be:
The thread’s claim is plausible at the level of follicular entry, but overstated at the level of bulge delivery.
Just use dermoelectroporation and call it a day. Now I’ve got plenty of hair but starting to get some grays that annoy me. I don’t think anything in this formula is aimed at reversing that is it?
Rapamycin is supposed to help here that’s why I worked on how to add it to a standard serum.
Here is a paper on that: mTORC1 activity negatively regulates human hair follicle growth and pigmentation
Here, we have used healthy, organ‐cultured human scalp hair follicles (HFs) to interrogate the role of mTORC1 in a prototypic human (mini‐)organ. Gray/white HFs exhibit high mTORC1 activity, while mTORC1 inhibition by rapamycin stimulated HF growth and pigmentation, even in gray/white HFs that still contained some surviving melanocytes.
2 Likes
Yes that’s interesting that both Claude and Gemini (both in thinking mode) agree while ChatGPT dissents.
Currently, the Only FDA-Approved Rx Option is HYFTOR which is a 0.2% rapa topical cream so I asked the 2 LLMs how it compares to the Transcutol serum version.
Again, I’m not a biochemist and I don’t have any informed opinion on that.
Here is Claude’s transcript followed by Gemini’s conclusion only.
Maybe somebody can also investigate with some more specialized LLMs.
HYFTOR vs Transcutol-Based Formulation
What HYFTOR Actually Is
HYFTOR (topical sirolimus 0.2%) was approved by the FDA in 2022 for facial angiofibromas in tuberous sclerosis complex. It’s the only FDA-approved topical rapamycin product, which makes its formulation choices directly relevant to your question.
Searched the web
Searched the web
Now let me fetch the full excipient list from the EMA document.
Searched the web
Searched the web
The full excipient list isn’t publicly accessible in the documents retrieved, but the EMA document clearly discloses the critical quantitative detail: each gram of gel contains 458 mg of ethanol European Commission — meaning HYFTOR is essentially 45.8% ethanol by weight. That’s the key number for this comparison.
HYFTOR’s Formulation vs Your Transcutol Approach
What HYFTOR Actually Relies On
Each gram of gel contains 2 mg of sirolimus European Commission, making it a 0.2% formulation — six times more concentrated than your 0.033%. The solvent system is overwhelmingly ethanol-based, with the alcohol serving triple duty: dissolving rapamycin, acting as the primary penetration enhancer, and forming the gel vehicle alongside a gelling agent.
The disclosed excipient breakdown tells a clear story:
| Component | HYFTOR (per gram) | Role |
|---|---|---|
| Sirolimus | 2 mg (0.2%) | Active |
| Ethanol | 458 mg (45.8%) | Solvent + penetration enhancer |
| Gelling agent + water | ~540 mg | Gel base |
| Transcutol | Not disclosed / absent | — |
How Alcohol Works as a Penetration Enhancer
Ethanol at high concentrations (>30%) enhances penetration through several mechanisms that partially overlap with Transcutol but are mechanistically distinct:
| Mechanism | Ethanol (45%) | Transcutol (5%) |
|---|---|---|
| SC lipid extraction | Strong — physically removes lipids from bilayers | Minimal — fluidizes without extracting |
| Evaporation effect | Yes — creates a concentration gradient as it evaporates, drawing drug into skin | No — non-volatile, stays in contact |
| Protein denaturation | Mild at 45% | None |
| Drug supersaturation | Yes — as ethanol evaporates, rapamycin concentration at skin surface increases transiently | No supersaturation effect |
| Skin reservoir formation | Moderate | Better — Transcutol accumulates in SC as a drug reservoir |
| Reversibility | Fast, complete | Slower, more sustained |
The ethanol approach is essentially a burst delivery model — high initial penetration driven by solvent evaporation and transient supersaturation, then rapid dissipation. Transcutol provides more of a sustained depot model — slower onset but more prolonged contact with the barrier.
Your Formulation vs HYFTOR — Direct Comparison
| Parameter | HYFTOR | Your serum |
|---|---|---|
| Rapamycin concentration | 0.2% | 0.033% (6× lower) |
| Primary penetration enhancer | Ethanol 45.8% | Transcutol 5% + alcohol already in base |
| Penetration mechanism | Burst / evaporative | Sustained depot |
| Additional enhancer | None identified | Tretinoin (barrier thinning) |
| Formulation complexity | Simple — drug in alcohol gel | Complex multi-active |
| Target tissue | Facial dermis (angiofibroma) | Scalp follicle bulge |
| Evidence base | FDA-approved RCT data | Mechanistic + ex vivo |
| Systemic absorption | Low — confirmed in trials | Expected low at 0.033% |
Does the Alcohol Comparison Favor Changing Your Approach?
This is the genuinely interesting question. A few observations:
HYFTOR’s 45% ethanol is not directly comparable to adding ethanol to your formula. Your base already contains alcohol — minoxidil serums are typically 30–50% ethanol by composition. So you may already have an ethanol concentration in the same territory as HYFTOR, plus Transcutol on top of that. This is actually a meaningful point: if your serum base is alcohol-heavy (which minoxidil bases typically are), you already have the evaporative burst mechanism that HYFTOR relies on, and Transcutol adds the sustained depot effect on top of it.
The concentration difference matters more than the vehicle difference. HYFTOR uses 0.2% rapamycin because it needs measurable clinical effects on macroscopic angiofibroma lesions in a clinical trial timeframe. Your target — follicle stem cell mTOR modulation — is a subtler biological effect. The evidence from the mTOR/hair follicle literature suggests that very low concentrations are sufficient for biological activity at the follicular level, which is why 0.033% is a defensible choice rather than a significant weakness.
Transcutol may actually be superior for your specific target. HYFTOR’s burst delivery model is optimized for superficial dermal targets (angiofibromas sit in the upper dermis of the face). Your target — the follicle bulge — is at 1.3–1.5mm depth and is better reached by sustained follicular deposition than by a rapid surface burst. Transcutol’s depot and follicular accumulation mechanism is arguably better suited to your application than pure alcohol evaporation.
One Practical Takeaway From HYFTOR
The FDA approval confirms unambiguously that systemic exposure to sirolimus is low in individuals using Hyftor European Commission at 0.2% twice daily — a much higher dose and frequency than your once-daily 0.033%. This is the strongest available human safety reference point for your formula, and it’s reassuring: if systemic exposure is low at six times your concentration applied twice daily, your systemic exposure risk is genuinely minimal.
Summary Verdict
Your Transcutol-based approach is not inferior to HYFTOR’s ethanol approach — it’s differently optimized and arguably better suited to follicular targeting. The main lesson HYFTOR offers isn’t that you need more alcohol; it’s that topical rapamycin in a high-alcohol vehicle is safe, effective, and FDA-validated in humans at concentrations well above yours. Your formula sits comfortably within that established safety envelope.
For comparison, here is the Gemini conclusion which is essentially similar to the Claude one.
You may notice Hyftor is 0.2%, while your DIY formula is ~0.033%.
- Hyftor is designed to treat Angiofibromas (benign tumors), which require a much higher “hammer” of mTOR inhibition to shrink physical tissue.
- Your Serum targets follicle rejuvenation. Research into topical rapamycin for longevity and hair suggests that lower, sub-therapeutic doses are often more effective for stimulating autophagy without completely shutting down necessary cellular growth pathways.
4. Practical Implications for Your Formulation
Because you are also using Tretinoin, the “Alcohol-only” approach of Hyftor would likely be far too irritating for your scalp. Alcohol is drying; Transcutol has emollient properties that help offset the potential irritation from the Tretinoin and Minoxidil.
Summary Recommendation: Stick with the 5% Transcutol. It is the more modern approach for follicle-specific delivery and provides a safer “buffer” for your complex multi-ingredient stack.
1 Like
Are you not worried about side effects related to systemic exposure to Dutasteride and Finasteride?
1 Like
Sorry, I don’t mean to crush the party LOL, but why would one need to do/add so many things when in fact just doing 1mg finasteride (btw, taking this for prostate health with the benefit of hair) and using a 5% minoxidil lotion from amazon has literally made my hair look as good or better than 15 years ago, and I’ve only been doing this for last 3-4 months or so. Even my chest hair is much thicker and looks as it used to look when my younger years in my 30’s. My point is adding these “extra” substances while it may do no harm, I think good results you guys are seeing are a result of minoxidil and finasteride. If this effect I’ve had continued for few more months literally my hair will be same as It was in my 20’s.
btw, Bonus, unless I’m daydreaming or something my hair is darker (on the sides) where I used to have gray hair also.
Apparently, my only point is to try and use the least number of meds to minimize unwanted side effects.
1 Like
No not worried. The mg amount is tiny, and for finasteride typically only solutions >1% concentration get measurable amounts and even then 1% of oral similar dosing levels. Tretinoin added can increase this 2-3 fold, but still not at all clinically significant. Dutasteride is a big molecule and basically no absorption.
3 Likes
I trust Claude and Gemini much more than ChatGPT… if they agree, its good enough for me.
You inspired me to go down the rabbit hole of options out there. Just here to share.
I liked the kitchen sink approach to this one from Happy Head and thought it was worth trying a new form, a gel vs drippy liquid. The form is so pleasant that I wanted to share incase it’s appealing to anyone else.
I have never used the rx drugs before, and I do worry about getting systemic absorption. Apparently, this formula is designed to avoid that.
Having said that, because I’m using this as a support/preventative measure, I’m also not planning to use it as directed. That will also keep costs down. PS, I did get a large discount on my first order.
I know from when I used to use latisse on my lashes, if I just used it 1x per day 3 days a week, it was enough to maintain my results, so I’ve always treated minoxidil in the same way. If anyone were balding, I’d use as directed and daily of course. In using minoxidil 3x per week does make a difference in my shedding. (I comb my hair when conditioning in the shower, so it’s really easy for me to see exactly what is going on)
Active Ingredients: Minoxidil (8%), Cetirizine HCl (1%), Latanoprost (0.005%), Dutasteride (0.25%), Finasteride (0.25%), Melatonin (0.1%), Caffeine (0.2%), Tretinoin (0.001%), Vitamin D3 (1,000 IU/ml), Biotin (0.2%)
- Inactive Ingredients: Lipodermal Base
I have long hair, so I would use my other stuff very sparingly and mostly the night before I was washing it.
This form is so mess free that I could easily use it every day if I wanted to. I put one pump on my fingers (as if it were a light lotion) and then I flip my head over and can easily get the product to my scalp while avoiding getting all over my hair.
The directions are once per day and 5 pumps. This is so mess free I could even see using one pump daily. (I don’t trust their avoidance of systemic absorption, so I wouldn’t use 5 pumps only because I’m not in great need)
EDIT:
I found a great discount code for my first order, so definitely look for one. My first order was $34.95
Also…I just checked my account and I see I have this offer.
1 Like