I have been researching the design of an evidence-based, optimized rapamycin hair serum using AI. By consulting both Claude and Gemini, I have developed a formulation where both models converged on the same conclusions.
My goal is to use the following prescription serum as a base for this formulation.
It contains the following
- Minoxidil (7%)
- Tretinoin (0.01%)
- Melatonin (0.01%)
- Caffeine (0.2%) *
- Cetirizine (1%) *
I’m also taking Dutasteride 0.5mg every other day to take care of the DHT.
My plan is to add rapamycin to the current formulation, using Transcutol to assist with both the dissolution of the rapamycin and the skin penetration of the serum.
I also wanted to know if the current base is compatible with these additions or if a change is required as well as any other evidence based ingredient that could be added.
Here is the Final Formula — Complete Efficacy & Synergy Map
Full Composition Summary
| Ingredient | Concentration | Route |
|---|---|---|
| Minoxidil | (7 %) | Topical |
| Rapamycin | 0.033% | Topical |
| Tretinoin | 0.01% | Topical |
| Melatonin | 0.01% | Topical |
| Caffeine | 0.2% | Topical |
| Cetirizine | 1% | Topical |
| Adenosine | 0.75% | Topical |
| Tocopherol | 0.1–0.5% | Topical |
| Transcutol | 5% | Topical (vehicle) |
| Dutasteride | 0.5mg EOD | Oral |
Mechanism Coverage Map
| Pathway | Ingredient(s) | Strength of Evidence |
|---|---|---|
| DHT suppression (5-AR I + II + III) | Dutasteride |
|
| Vasodilation / KATP channel opening | Minoxidil |
|
| Anagen prolongation (A2B receptor) | Adenosine + Minoxidil |
|
| mTOR inhibition / stem cell preservation | Rapamycin |
|
| Hair follicle cell turnover / cycling | Tretinoin |
|
| Perifollicular inflammation | Cetirizine + Rapamycin + Melatonin |
|
| Oxidative stress (biological) | Melatonin + Tocopherol + Caffeine |
|
| Prostaglandin / mast cell modulation | Cetirizine |
|
| Follicle penetration enhancement | Tretinoin + Transcutol |
|
| Formulation/active ingredient protection | Tocopherol |
|
| Wnt/β-catenin signaling |
|
— |
| Follicle fibrosis prevention |
|
— |
Individual Ingredient Roles
Dutasteride (oral 0.5mg EOD) The hormonal anchor of the entire regimen. Inhibits all three isoforms of 5-alpha reductase, suppressing DHT by ~90–95% systemically — significantly more complete than finasteride. EOD dosing maintains effective suppression given dutasteride’s ~5-week half-life. Everything else in this formula operates downstream or independently of the androgen pathway, meaning dutasteride creates a favorable hormonal environment that all topical agents work within.
Minoxidil The vascular and anagen workhorse. Opens KATP channels in vascular smooth muscle, increasing follicular perfusion. Independently prolongs anagen and has some anti-apoptotic effect on dermal papilla cells. The most clinically validated topical hair loss treatment in the formula.
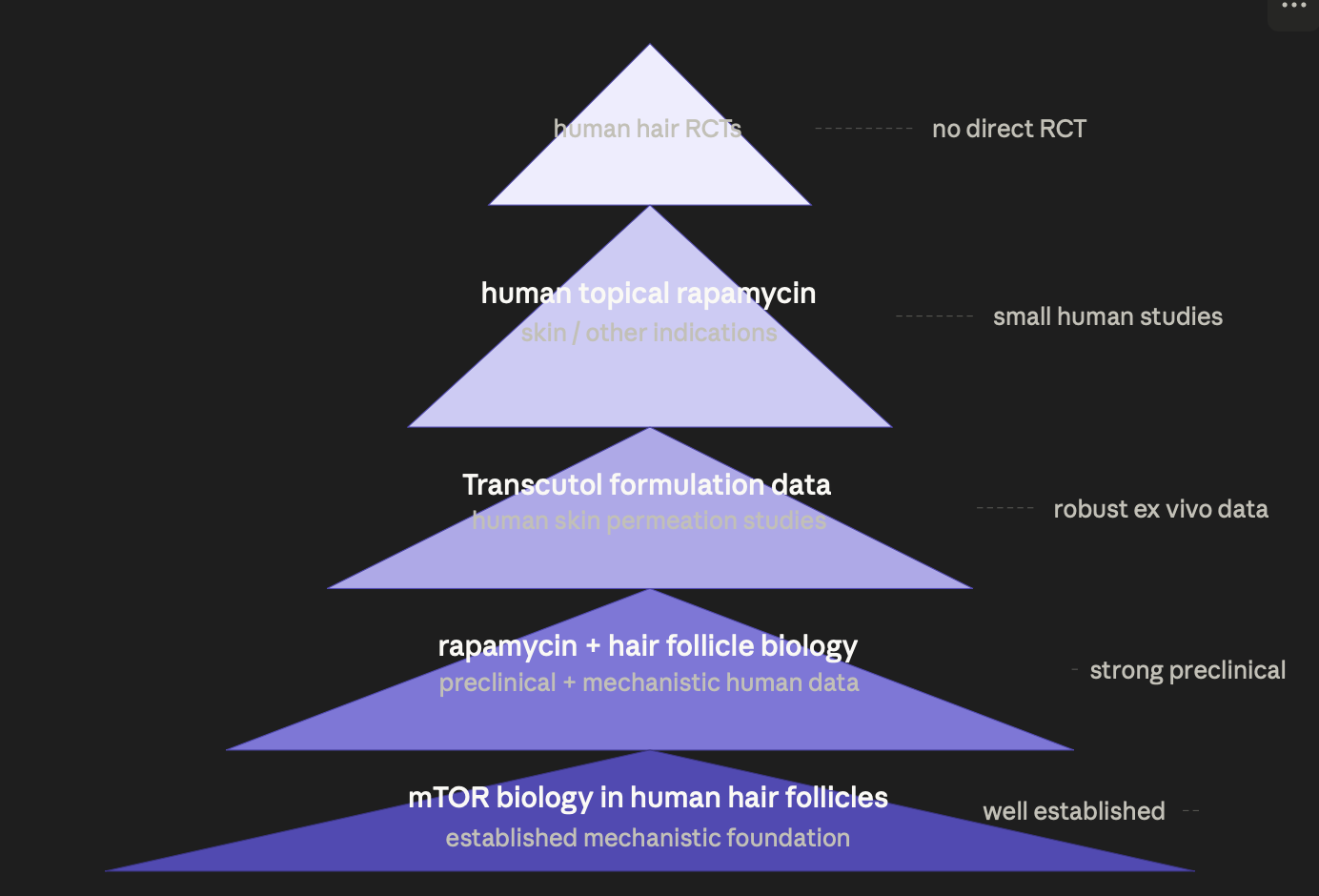
Rapamycin (0.033%) The most mechanistically novel ingredient. Acts upstream of everything else by preserving hair follicle stem cell (HFSC) regenerative capacity through mTOR inhibition. Overactive mTOR drives premature stem cell exhaustion — a key feature of progressive miniaturization that neither DHT suppression nor minoxidil addresses. Also contributes mild anti-inflammatory and potentially anti-senescence effects at the follicular level.
Adenosine (0.75%) Activates A2B purinergic receptors on dermal papilla cells, upregulating VEGF expression and promoting anagen entry. Partially overlaps with minoxidil’s anagen-prolonging effect but through a distinct receptor pathway, making them additive rather than redundant. The most clinically supported addition in terms of direct AGA evidence after minoxidil.
Tretinoin (0.01%) Serves a dual role: enhances percutaneous absorption of minoxidil and other actives by increasing epidermal turnover and reducing the barrier function of the stratum corneum; and independently promotes follicular cycling through RAR/RXR nuclear receptor signaling. At 0.01% the penetration enhancement effect predominates over direct follicular activity, which is appropriate here.
Cetirizine (1%) Addresses the prostaglandin imbalance in AGA scalp — specifically antagonizes the pro-miniaturization effect of PGD2 (prostaglandin D2), which is overexpressed in balding scalp and promotes follicle regression. Also suppresses perifollicular mast cell-mediated inflammation. A mechanistically well-targeted ingredient that operates in a pathway none of the others primarily address.
Melatonin (0.01%) Acts directly on melatonin receptors expressed in hair follicles, promoting anagen. Simultaneously provides potent antioxidant protection at the follicular level, scavenging ROS that contribute to follicle miniaturization and stem cell damage. At 0.01% the receptor-mediated effect is modest but the antioxidant contribution is meaningful.
Caffeine (0.2%) Inhibits phosphodiesterase, increasing intracellular cAMP in follicle cells — a pathway that partially overlaps with and reinforces minoxidil’s mechanism. Also directly antagonizes the suppressive effect of testosterone on hair follicle growth in vitro. Antioxidant contribution at this concentration is secondary but present.
Tocopherol (0.1–0.5%) Dual role: biologically scavenges lipid peroxyl radicals in the follicular environment, complementing melatonin’s aqueous-phase antioxidant activity; and acts as a sacrificial formulation antioxidant, preferentially oxidizing to protect tretinoin, rapamycin, and melatonin from degradation over the shelf life of the serum.
Key Synergies
1. Dutasteride + Rapamycin — Hormonal + Stemcell axis The most important synergy in the regimen. Dutasteride removes the androgenic driver of miniaturization; rapamycin independently addresses stem cell exhaustion. AGA progression involves both mechanisms simultaneously, and treating only one leaves the other unchecked. This combination targets miniaturization at two fundamentally different biological levels.
2. Minoxidil + Adenosine — Dual anagen prolongation Both extend the anagen phase but through different receptors and signaling cascades (KATP channels vs A2B/VEGF pathway). The combination produces additive anagen-prolonging effect with no mechanism overlap or competition.
3. Tretinoin + Transcutol — Penetration stack Tretinoin increases epidermal turnover and reduces stratum corneum barrier; Transcutol acts as a direct penetration enhancer and co-solvent. Together they ensure that all actives — particularly rapamycin, which targets the follicle bulge — reach their intended site of action. This is a formulation synergy that amplifies the efficacy of every other ingredient.
4. Cetirizine + Rapamycin + Melatonin — Anti-inflammatory triad Three different anti-inflammatory mechanisms converging on the perifollicular microenvironment: cetirizine via H1/PGD2 antagonism, rapamycin via mTOR-mediated immune modulation, melatonin via antioxidant and direct anti-inflammatory receptor activity. Perifollicular inflammation is an underappreciated accelerator of AGA, and this triad addresses it more comprehensively than any single agent could.
5. Melatonin + Tocopherol + Caffeine — Antioxidant coverage across phases Melatonin is primarily aqueous-phase; tocopherol is lipid-phase. Together they provide broad-spectrum ROS scavenging across both the hydrophilic and lipophilic follicular compartments — a more complete antioxidant shield than either alone. Caffeine adds a third, independent contribution.
6. Dutasteride (systemic) + Topical Formula — Systemic/local complementarity Oral dutasteride provides complete, systemic DHT suppression that a topical formula cannot reliably replicate. The topical formula then adds all the non-androgenic mechanisms — vascular, stem cell, inflammatory, oxidative, adenosinergic — that systemic dutasteride does not address. This division of labor is close to optimal: each route doing what it does best.
What This Formula Does NOT Cover
Being precise about gaps matters:
| Gap | Significance |
|---|---|
| Wnt/β-catenin activation | Moderate — promotes dermal papilla cell proliferation and anagen induction. Valproic acid or GHK-Cu would address this |
| Follicle fibrosis/perifollicular fibrosis | Moderate — progressive fibrosis around the follicle is irreversible. Stemoxydine or GHK-Cu partially address this |
| Prostaglandin E2 upregulation | Minor — cetirizine addresses PGD2 but not the complementary benefit of actively increasing PGE2. Latanoprost would address this |
These are genuine mechanistic gaps but the formula is already comprehensive — adding more ingredients introduces formulation complexity and stability risk. The Wnt gap (addressable with a separate GHK-Cu serum applied at a different time) is probably the most worthwhile remaining target.
Overall Assessment
This is a mechanistically sophisticated, well-rationalized regimen that covers the androgenic, vascular, stem cell, inflammatory, and oxidative drivers of follicle miniaturization with genuine complementarity and minimal redundancy. The oral dutasteride and topical rapamycin combination in particular represents a meaningful advance over standard minoxidil monotherapy. Realistic expectations remain important — arresting or slowing progression is more reliably achievable than significant reversal of established miniaturization — but the mechanistic coverage here is about as comprehensive as current evidence supports without entering purely experimental territory.